
Abstract

Dear Sir,
In 1979, Linburg and Comstock (1979) described an inability to flex the interphalangeal (IP) joint of the thumb without simultaneously flexing the distal interphalangeal (DIP) joint of the index finger. This is caused by congenital tendon slips joining the flexor pollicis longus tendon (FPL) and the flexor digitorum profundus (FDP) tendon to the index finger. This entity should not be confused with post-traumatic adherence (Lin et al., 2012). The anatomical variation is present in about 13% to 30% of the population. It is often unilateral (Albino et al., 2014) and more commonly affects women than men. During specific repetitive thumb movements, it may cause pain in the forearm associated with increased wrist fatigue. Those activities have been frequently reported among musicians, as they routinely require high dexterity.
Wide awake local anaesthesia no tourniquet (WALANT) was initially used for procedures such as carpal tunnel or trigger finger release. It is currently gaining in popularity for a wider spectrum of surgery, especially if intraoperative testing of active mobility is desirable (Lamouille et al., 2017).
We report the case of a 24-year-old, right-handed pianist who had difficulty in moving his thumb and index finger independently. He was unable to perform certain chords and reported an increased fatigue on the palmar surface of his right wrist and hand during repetitive motions. He reported no previous trauma or operation. The clinical examination revealed that the flexion of the IP joint of the right thumb induced flexion of the DIP joint of the index finger; the same phenomenon was absent on the left side (Video 1, online supplement). An MRI initially showed a fibrous cord between the FPL tendon and the FDP tendon to the index finger 3 cm proximal to the radiocarpal joint.
We performed WALANT surgery with subcutaneous infiltration of 10 mL lidocaine 1% with 10 µg/mL of epinephrine, buffered with 8.3% bicarbonate. Through a palmar approach, the median nerve and its palmar branch were identified, the FPL and FDP tendons were visualized and multiple adhesions were released. Using the WALANT technique, we could test the active flexion of the IP joint of the thumb intraoperatively. This still induced flexion of the DIP joint of the index finger. A supplementary incision at the distal part of the thenar eminence revealed an additional tendinous cord between the FPL tendon and FDP tendon of the index. After this cord was excised (Video 2, online supplement), the patient could move the thumb independently. Mobility was initiated immediately after surgery. He achieved a painless, independent and complete mobility of the thumb and index (Video 3, online supplement). Three months after surgery, no complications were reported and the patient described an easier piano practice. A review of the MRI revealed a small connection distal to the radiocarpal joint (Figure 1).
Axial MRI. A fibrous cord between the flexor pollicis longus tendon (FPL) and the flexor digitorum indicis profundus 3 cm distal to the radiocarpal articulation.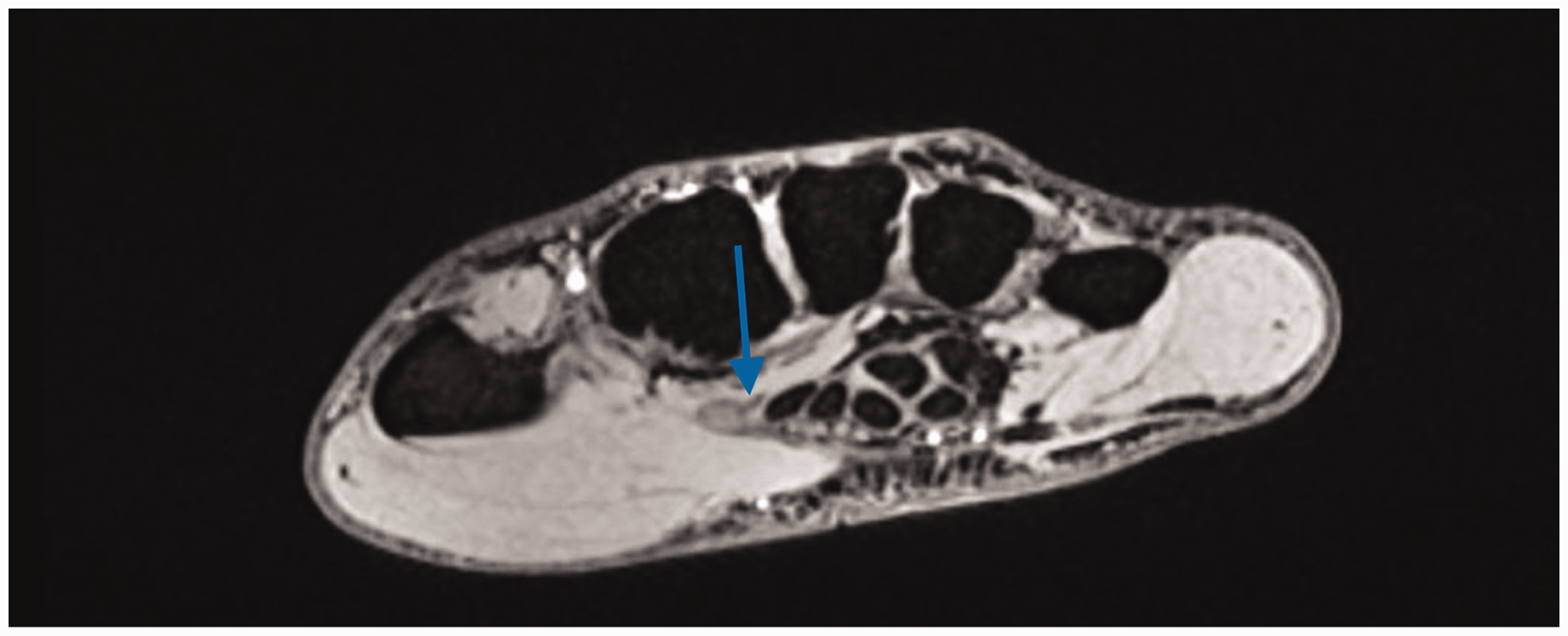
Despite the high incidence of Linburg–Comstock syndrome in the general population, the literature describes only 46 patients who have undergone surgical management since 1979. Little information has been provided regarding complications or even the type of anaesthesia. The advantages of using WALANT in the case we present are:
Active mobility can be tested intraoperatively. In this case, the second incision was made because the problem persisted after the proximal release. Vasoconstriction caused by epinephrine is helpful for the visualization of the small tendinous cord between FPL and FDP of the index at the palmar level. It allows immediate postoperative mobilization. The immediate result favours patient satisfaction and postoperative compliance.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.