
Abstract
The dorsal cutaneous branch of the ulnar nerve can be easily injured during surgery at the ulnar side of the wrist. We sought to identify the surgical anatomy, the pathway around the ulnar styloid process and the safe zone of the dorsal cutaneous branch of the ulnar nerve. In 44 forearm dissections, we found that the dorsal cutaneous branch of the ulnar nerve originated at a median distance of 6.8 cm proximal to the tip of the ulnar styloid. We classified the crossing pattern of the dorsal cutaneous branch of the ulnar nerve at a vertical axis into three types. The most common type featured the dorsal cutaneous branch of the ulnar nerve crossing the vertical axis at a median distance of 10.0 mm distal to the tip of the ulnar styloid. In 14% of specimens, the dorsal cutaneous branch of the ulnar nerve crossed the vertical axis at the level of the tip of the ulnar styloid. By mapping the course of the nerve using a Cartesian coordinate system, it was found that the areas located proximal and palmar to the tip of the ulnar styloid had a very high density of dorsal cutaneous branches of the ulnar nerve. We were unable to establish a safe zone. We recommend identifying the dorsal cutaneous branch of the ulnar nerve in every patient undergoing surgery at the ulnar side of the wrist.
Introduction
The dorsal cutaneous branch of the ulnar nerve (DCBUN) arises from the medial aspect of the ulnar nerve at a mean distance of 6.4 cm proximal to the ulnar styloid process. It crosses the flexor carpi ulnaris tendon, then pierces the deep antecubital fascia and becomes subcutaneous on the medial aspect of the forearm at a mean distance of 5.0 cm proximal to the pisiform bone (Botte et al., 1990). At the level of the ulnar styloid process, the DCBUN further divides into multiple branches to innervate the dorso-ulnar skin of the hand and wrist (Botte et al., 1990; Root et al., 2013). This anatomical location puts it at risk of injury during surgery at the ulnar side of the wrist. Traumatic or iatrogenic injury to the DCBUN may lead to paraesthesia in the innervated skin area and painful neuroma which disturb the patient’s daily activity. Previous studies have concluded that there are two types of the DCBUN based on the location of its crossing toward the ulnodorsal aspect either proximal or distal to the ulnar styloid process (Goto et al., 2010). However, we found that 10% (five in 50 cases) of patients who underwent operation at the ulnar styloid process had clinical symptoms of an injury of the DCBUN. These findings suggested that there may be another type of course of the DCBUN that lies directly on the ulnar styloid process. Our purposes were to study the anatomical course of the DCBUN at the ulnar aspect of the wrist by using a Cartesian coordinate system and assess whether it was possible to identify a safe zone of the DCBUN, to prevent iatrogenic injury to this nerve.
Methods
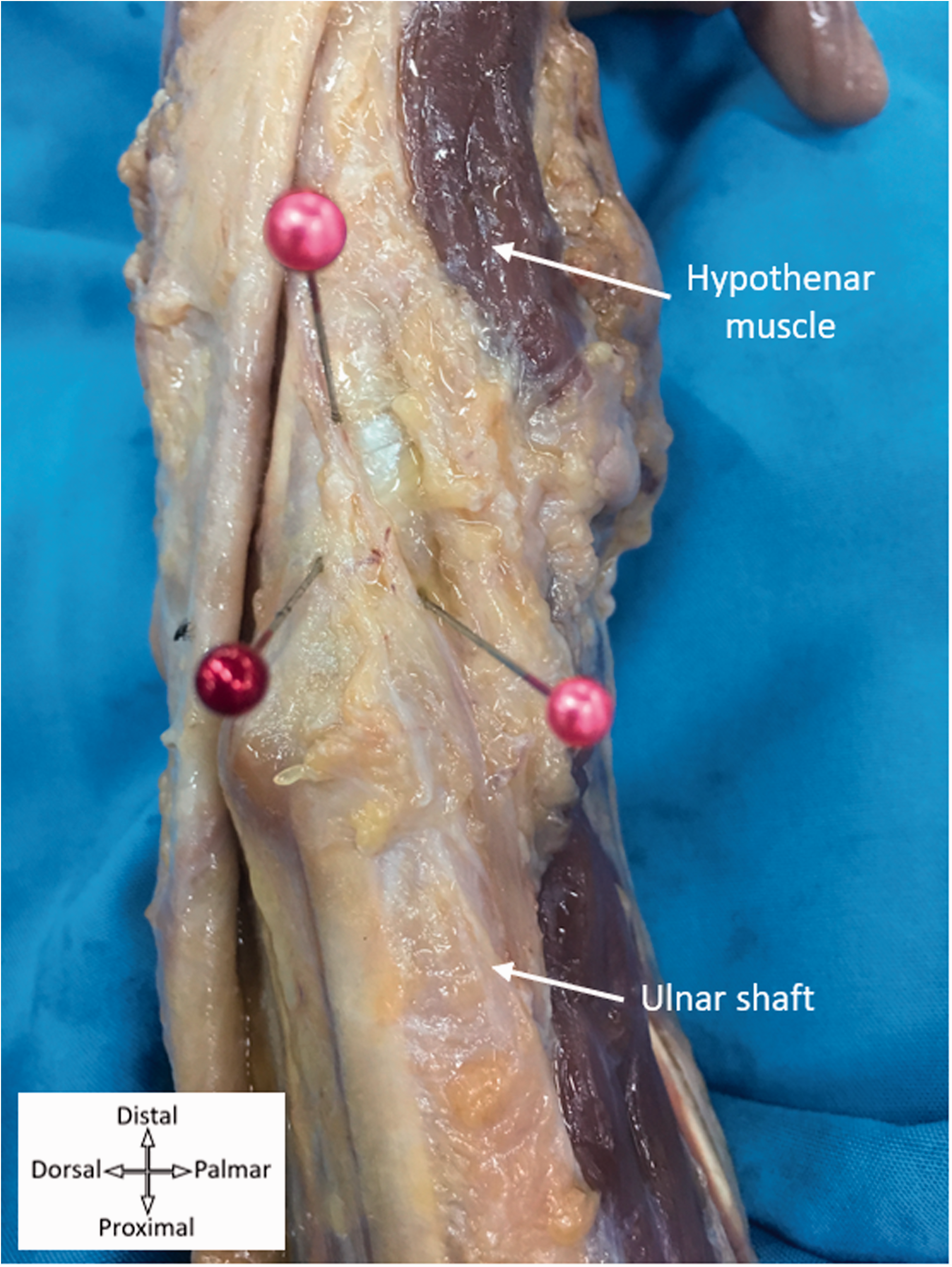
Forty-four forearms from 22 fresh cadavers were included in this study. These comprised 18 men and four women. Their mean age was 68 years (range 55–85). None had gross deformity or history of severe trauma causing fracture. The cadavers were placed in a supine position with the forearm in supination. A long ulnar-based skin flap incision was made from the proximal third of the forearm to the distal palmar crease. The subcutaneous plane was gradually developed and dissection was carried out in a radial to ulnar direction until the whole of the ulnar head was exposed. Every care was taken to ensure that all soft tissue around the nerves was preserved. Before further dissection, all nerves were left undisturbed and pinned in their original location (Figures 1 and 2). The DCBUN was then clearly dissected and traced proximally to its origin from the main ulnar nerve. Again, the DCBUN was carefully dissected to preserve its original course. It was then pinned to the soft tissue of the forearm.
Cadaveric dissection at the ulnar aspect of the right forearm and wrist showing the ulnar-based flap approach that was used for exposure of the main ulnar nerve and the dorsal cutaneous branch of the ulnar nerve. The nerves were pinned at their original sites. The tip of the ulnar styloid (red-headed pin); the dorsal cutaneous branch of the ulnar nerve (pink-headed pin).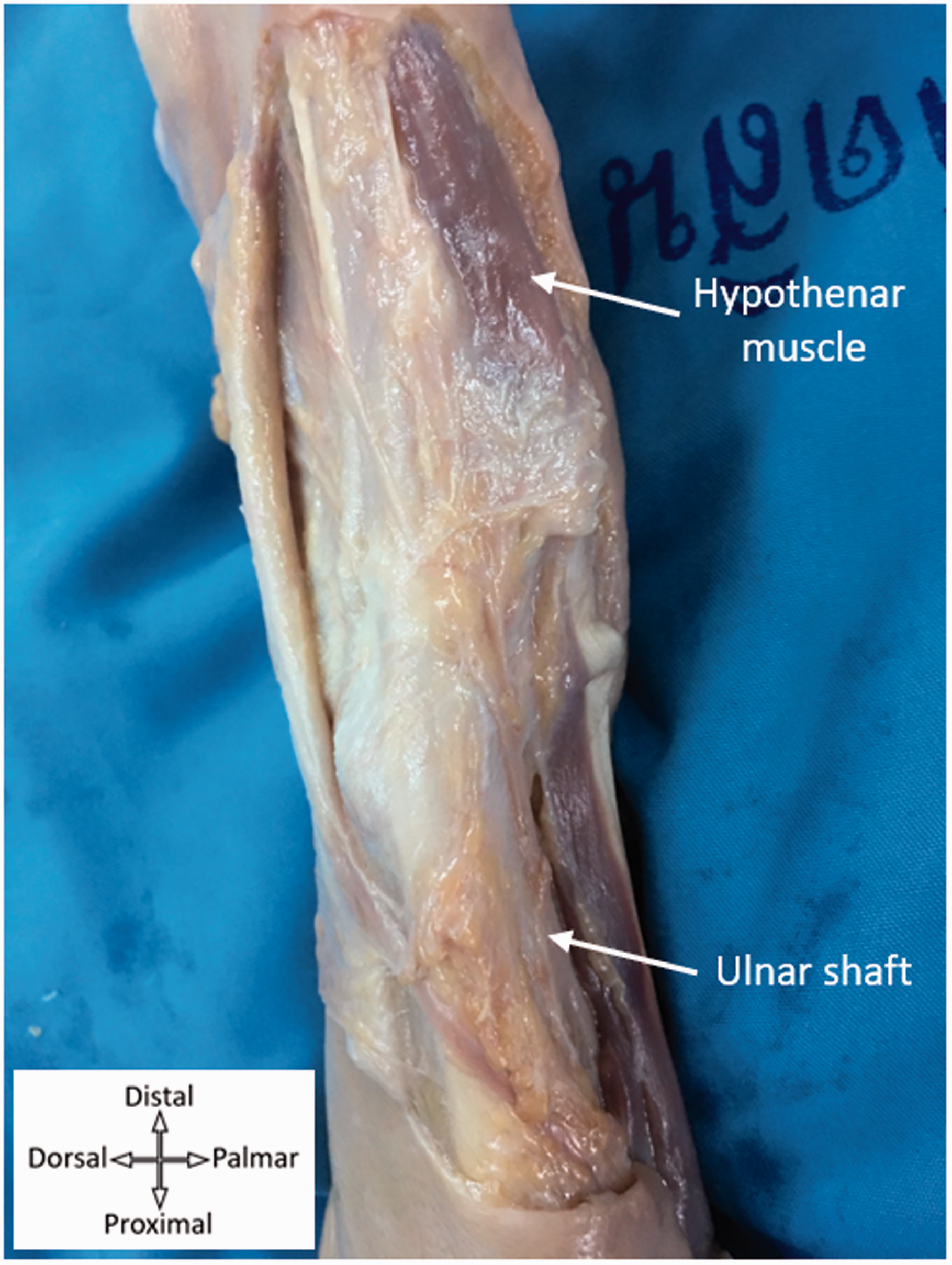
After marking the DCBUN and the ulnar nerve, with the elbow in flexion, the forearm was brought into a position of mid-rotation. The complete pathway of the DCBUN and the ulnar nerve was recorded. We measured the distance from the ulnar styloid tip at three points. The first point was where it arose from the main ulnar nerve. We set a horizontal line passing through the tip of the ulnar styloid as a transverse imaginary line and a line passing from the ulnar border of the hand through the tip of the ulnar styloid and ulnar crest as a vertical imaginary line. The second and the third points were where the DCBUN crossed the transverse and vertical imaginary lines, respectively. We also measured the length of the forearm from the tip of the ulnar styloid to the tip of olecranon process and the width of the ulnar head. We used a digital Vernier caliper (Digimatic Caliper; Mitutoyo Corp., Kanagawa, Japan; resolution 0.01 mm; accuracy ± 0.02 mm) for measurement. All measurements were carried out three consecutive times with a repetition interval of 5 minutes. The mean values were recorded. We also did an intraclass correlation coefficient (ICC) to analyse the reliability of the measurement. Since one observer (DP) did all the measurements, a two-way random effects model with absolute agreement analysis was used.
To study the anatomical course of the DCBUN, we used a Cartesian coordinate system projected onto the ulnar aspect of the wrist. The x- and y-axes represented the transverse and vertical imaginary lines, respectively. The tip of the ulnar styloid tip was set as the origin (0, 0) in the Cartesian coordinate system. All measured distances were recorded as positive values when they were palmar or distal to the tip of the styloid. Quadrant I represented the area distal-palmar to the ulnar styloid tip while Quadrant II represented the distal-dorsal to the ulnar styloid tip area. Quadrants III and IV represented the proximal-dorsal area and proximal-palmar area, respectively (Figure 3). All the DCBUN pathways were standardized to the same ratio and were mapped into the Cartesian coordinate system. The percentages of the DCBUNs passing through each quadrant were calculated.
The tip of the ulnar styloid was used as a reference point to measure the distance at which the dorsal cutaneous branch of the ulnar nerve crosses the transverse and vertical axes.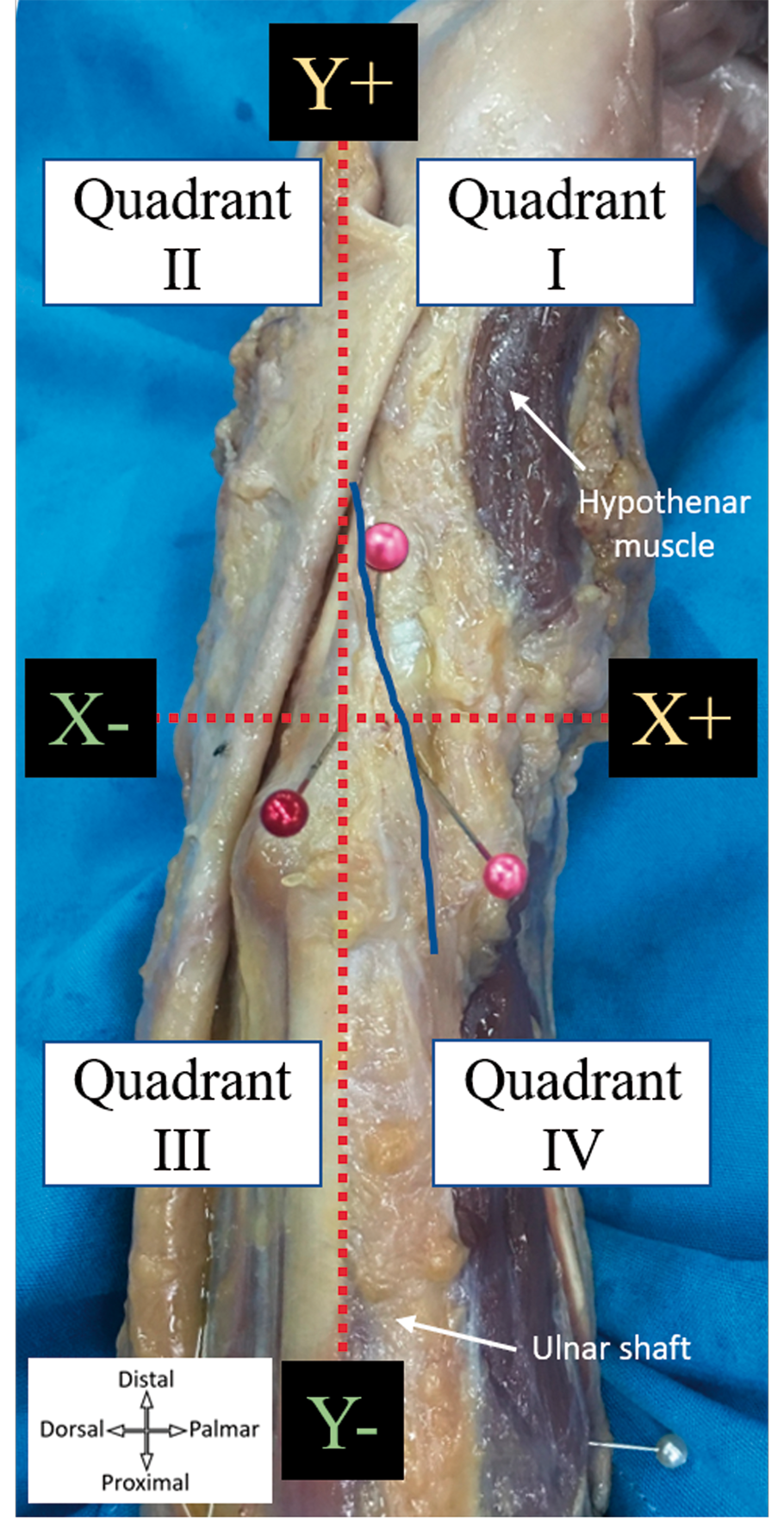
The measurement data were not normally distributed and are therefore presented as median values with interquartile ranges (IQR) and the range.
Results
The median length of the forearms was 26.9 cm (IQR 26.1–27.4; range 22.5–28.3). The DCBUN arose from the ulnar nerve at a median distance of 6.8 cm (IQR 6.2–8.5; range 4.3–10.6), proximal to the tip of the ulnar styloid and approximately at distal 25% of the length of the forearm. The median width of the ulnar head was 18.3 mm (IQR 17.3–19.4; range 13.1–21.7). The course of all the DCBUNs was from a palmar to dorsal direction to become a subcutaneous nerve.
In 34 of the 44 forearms, the DCBUN crossed the vertical imaginary line (y-axis) distal to the ulnar styloid tip at a median distance of 10.0 mm (IQR 6.6–14.2; range 3.5–21.2). In four forearms, the DCBUN crossed the y-axis proximal to the ulnar styloid tip at a median distance of 11.2 mm (range 3.5–18.6). There were six forearms in which the DCBUN passed over the tip of the ulnar styloid. There were 34 forearms in which the DCBUN crossed the x-axis palmar to the ulnar styloid tip at a median distance of 5.6 mm (IQR 4.2–6.9; range 2.6–17.5), while in four specimens, the DCBUN crossed the x-axis at a median distance of 1.5 mm (range 0.2–8.1) dorsal to the ulnar styloid tip.
Reliability analysis revealed an ICC value of 1.00 in all measurements (distance of the origin of the DCBUN to the tip of the ulnar styloid, distance from where the DCBUN crossed the vertical imaginary line to the tip of the ulnar styloid, and distance from where the DCBUN crossed the horizontal imaginary line to the tip of the ulnar styloid).
To identify the safe zone of the DCBUN around the tip of the ulnar styloid, the minimal distances the DCBUN crossed the horizontal imaginary line were 2.6 mm at the palmar side and 0.2 mm at the dorsal side on the x-axis. On the y-axis, the minimal distances the DCBUN crossed the vertical imaginary line were 3.5 mm distally and 3.5 mm proximally. As noted, in six of 44 forearms (14%), the DCBUN traversed directly over the tip of the ulnar styloid (0, 0). Therefore, there was no absolute safe zone of the DCBUN within a radius of 1 cm around the tip of the ulnar styloid.
When we projected the pathways of all the DCBUNs into the Cartesian coordinate system, we found that the area containing the highest percentage of nerves passing through was proximal-palmar to the ulnar styloid tip, Quadrant IV (98%). The second highest percentage area was distal-palmar, Quadrant I (91%). The third was distal-dorsal, Quadrant II (75%). The lowest percentage area was proximal-dorsal to the ulnar styloid tip, Quadrant III (9%) (Figure 4).
All the dorsal cutaneous branch of the ulnar nerve courses were projected into the Cartesian coordinate system. The blue lines represent type 1, proximal type. The yellow lines represent type 2, distal type. The pink lines represent type 3, ulnar styloid tip type. Quadrants IV, I and II have high densities of the nerve passing through them. Quadrant III has the least risk of injury to the dorsal cutaneous branch of the ulnar nerve.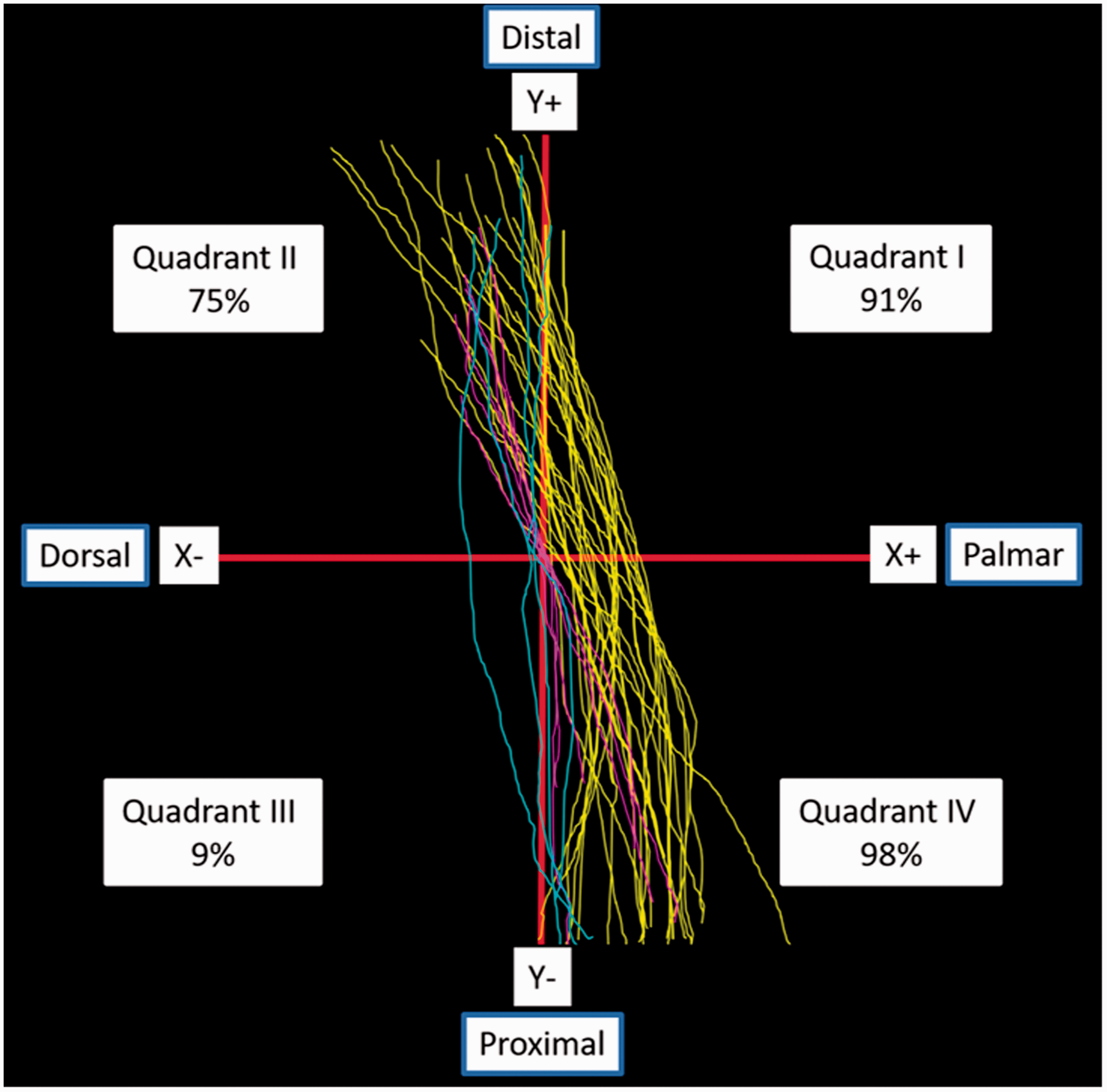
Discussion
The origin of the DCBUN has been reported to be in the range of 3.4–6.4 cm proximal to the ulnar styloid process (Botte et al., 1990; Goto et al., 2010; Le Corroller et al., 2013; Puna and Poon, 2010). Its anatomical course has also been previously reported (Goto et al., 2010). In our study, the data were not normally distributed; we found that the DCBUN originated at a median distance of 6.8 cm, which is comparable to previous studies.
Goto et al. (2010) studied 30 embalmed cadaver specimens and classified the DCBUN into two types, proximal and distal, according to their relationship to the ulnar styloid process. They reported that the incidence of proximal and distal types was 70% and 30%, respectively. They also reported that the distance from the point at which the DCBUN crossed the vertical line to the ulnar styloid process in proximal and distal types was a mean of 11 and 17 mm, respectively. However, we found that there were three types of DCBUN at the ulnar side of the wrist (Figure 5). Type 1 is the proximal type accounting for 9% (4/44) of the specimens. It crossed the vertical axis at the median distance of 11.2 mm proximal to the tip of the ulnar styloid. In type 2, the distal type, the nerve crossed the vertical axis at a median distance of 10.0 mm distal to the tip of the ulnar styloid. This most common type accounted for 77% (34/44) and thus our findings are different from the study by Goto et al. (2010). Six specimens (14%) were considered to be type 3, in which the DCBUN ran across the vertical axis at the ulnar styloid process level.
Classification of the three types of dorsal cutaneous branches of the ulnar nerve at the ulnar aspect of the wrist.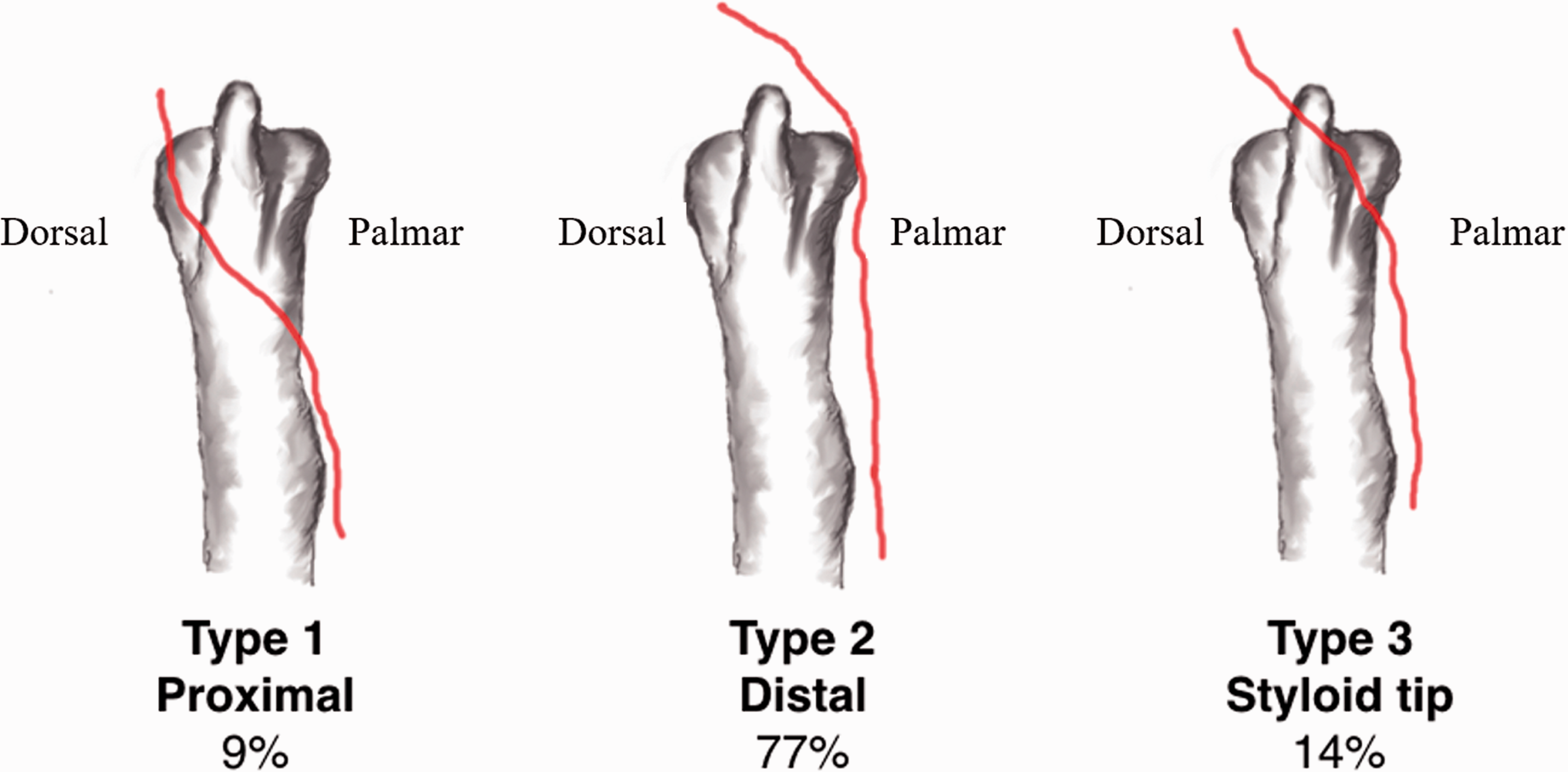
In type 1, in which the DCBUN crossed ulna shaft proximally, its course became subcutaneous around the medial border of the ulna at the median of 11.2 mm proximal to the tip of the ulnar styloid. When compared to the median width of the ulnar head, 18.3 mm, the DCBUN in this type crossed this vertical axis at approximately 61% of the width of the ulnar head proximal to the tip of the ulnar styloid.
In type 2, the most common type, the DCBUN crossed the midline distal to the tip of the ulnar styloid tip at a median distance of 10.0 mm or 54% of the width of the ulnar head. Therefore, the distance of 54% of the ulnar head width from the tip of the ulnar styloid in a vertical line, proximally and distally, may be used as the topographic anatomical landmark for types 1 and type 2 of the DCBUN. A circle of this 54% of ulnar head width, centred at the tip of the ulnar styloid, would seem to be a safe zone for both types 1 and 2. Unfortunately, in the 14% of specimens in which the DCBUN traversed the ulnar styloid tip (type 3), an incision or pinning at the ulnar styloid may cause an injury to the DCBUN.
The DCBUN has been considered to be at risk when the 6R portal is created during wrist arthroscopy. It has been recommended to spread the soft tissue and move the nerve away (Goto et al., 2010). Poublon et al. (2016) reported that they could not identify a completely safe zone for the DCBUN. They also agreed with the technique of spreading the soft tissue down to the capsule to prevent injury to the DCBUN. Risk of injury to the DCBUN at the 6R, 6U and mid-carpal ulnar portals during wrist arthroscopy has also been reported clinically and anatomically (McAdams and Hentz, 2002; Root et al., 2013; Tsu-Hsin Chen et al., 2006). Taking into account all the minimal distances of the DCBUN to the tip of the ulnar styloid and the three types of DCBUN, we conclude that there is no absolutely safe zone for the DCBUN around the tip of the ulnar styloid. We advise using the spreading technique in closed methods or carefully identifying the DCBUN in open techniques for all operations in this particular area.
We found that Quadrants IV, I and II had high density of DCBUNs passing through with percentages of 98%, 91% and 75%, respectively. Quadrant III, proximal-dorsal, had the least density at 9%. These percentages may be helpful for surgeons in preventing DCBUN injuries during operations in the area of the ulnar styloid. From our study, we suggest that incision or pinning in the area proximal-dorsal to the ulnar styloid, Quadrant III, carries the smallest risk of injury to the DCBUN. Surgery in Quadrants I, II and IV, however, pose very high risks of injury to the DCBUN.
Some anatomical variances of the DCBUN have been reported. Sulaiman et al. (2015) found that there was a connection between the DCBUN and the superficial radial nerve in 26%. They also found that 2.9% of the DCBUNs and superficial radial nerves overlapped, contributing to the innervation of the same area. They found absence of the DCBUN in which the entire dorsum of the hand was innervated by the superficial radial nerve in 6.6%. These findings may explain subtle variations in clinical symptom in patients who sustain a DCBUN injury. However, we did not find such variants of the DCBUN in our study.
Previous studies have used other landmarks as reference points for measuring distances of the DCBUN. Cavusoglu et al. (2011) measured the distance between the DCBUN and the pisiform bone in order to understand the anatomy for designing a neurocutaneous flap. However, the pisiform bone may not be a good reference point because it is a mobile structure. Its location can also be easily changed with wrist movement. We used the ulnar styloid tip as the reference point because of its immobility and the ease of palpation. It is also the most commonly used landmark in wrist arthroscopic surgery.
There are some limitations to this study. Displacement of the DCBUN may occur during cadaveric dissection. We were concerned about this problem and sought to minimize this error by pinning the DCBUN at all points while dissection was progressing. This allowed the initial anatomical course of the DCBUN to be preserved. The Cartesian coordinate system used in this study is a two-dimension coordinate system that specifies a point in a plane. Projection of this system onto the ulnar side of the wrist, which is three-dimensional, might not be a perfect match and the measured values might not represent true values. However, we used the Cartesian coordinate system mainly to study the courses and percentages of the DCBUNs passing through each quadrant. Moreover, the dimension of the study area on the ulnar surface of the wrist was so small that the slight convexity of the ulnar head surface may be disregarded.
Footnotes
Acknowledgements
We would like to express our respect and thank to all donors of the cadavers in this study. We also would like to thank Dr. Sitha Piyasilakul for cadaver preparation process and Dr. Kraisuvit Nuchman for data collection.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the ethics committee of Lerdsin General Hospital.