
Abstract

Dear Sir,
A recent study with hand surgeons using loupes revealed a high variability of visual performance in a clinical setting (Perrin et al., 2016). Some of the tested surgeons could detect structures that were three times smaller than those detected by other surgeons. The visual performance was also influenced by the type of loupe and by the surgeons’ age. Baker and Meals (1997) reported that Keplerian (prismatic) loupes performed significantly better than Galilean, which could be expected owing to their higher magnification factor and their sophisticated optics (Baker and Meals, 1997).
The inevitable presbyopic decline with increasing age begins at an age of about 40 years and involves not only reduced accommodation, but also more sensitivity to glare, a reduced ability to recognize contrasts and an increased need for light. A self-assessment using a visual analogue scale hardly correlated with the objective results of the visual performance (Perrin et al., 2016). This finding implicates the need for an adequate visual test. Traditional near visual tests cannot accommodate the size of the structures that surgeons can see with optical aids, and the miniaturized tests used in the mentioned study with hand surgeons are not commercially available. Most banknotes incorporate miniaturized structures or letters printed with a sophisticated technique to prevent forgeries.
We evaluated different currencies and values and determined that the new 10 EUR-bill is suitable for an easy-to-perform and readily available near vision test with loupes. The banknote was mounted on a black A5 paper sheet to obtain a standardized contrast. The self-declared yes/no result indicates whether or not the repeated number 10 in the balustrade of the arch bridge could be read in the usual clinical setting and with the standard operating light (Figure 1).
Visual triage test with a 10 EUR banknote. The number 10 is continuously repeated in the balustrade of the arch bridge and can be seen with loupes under an operating lamp.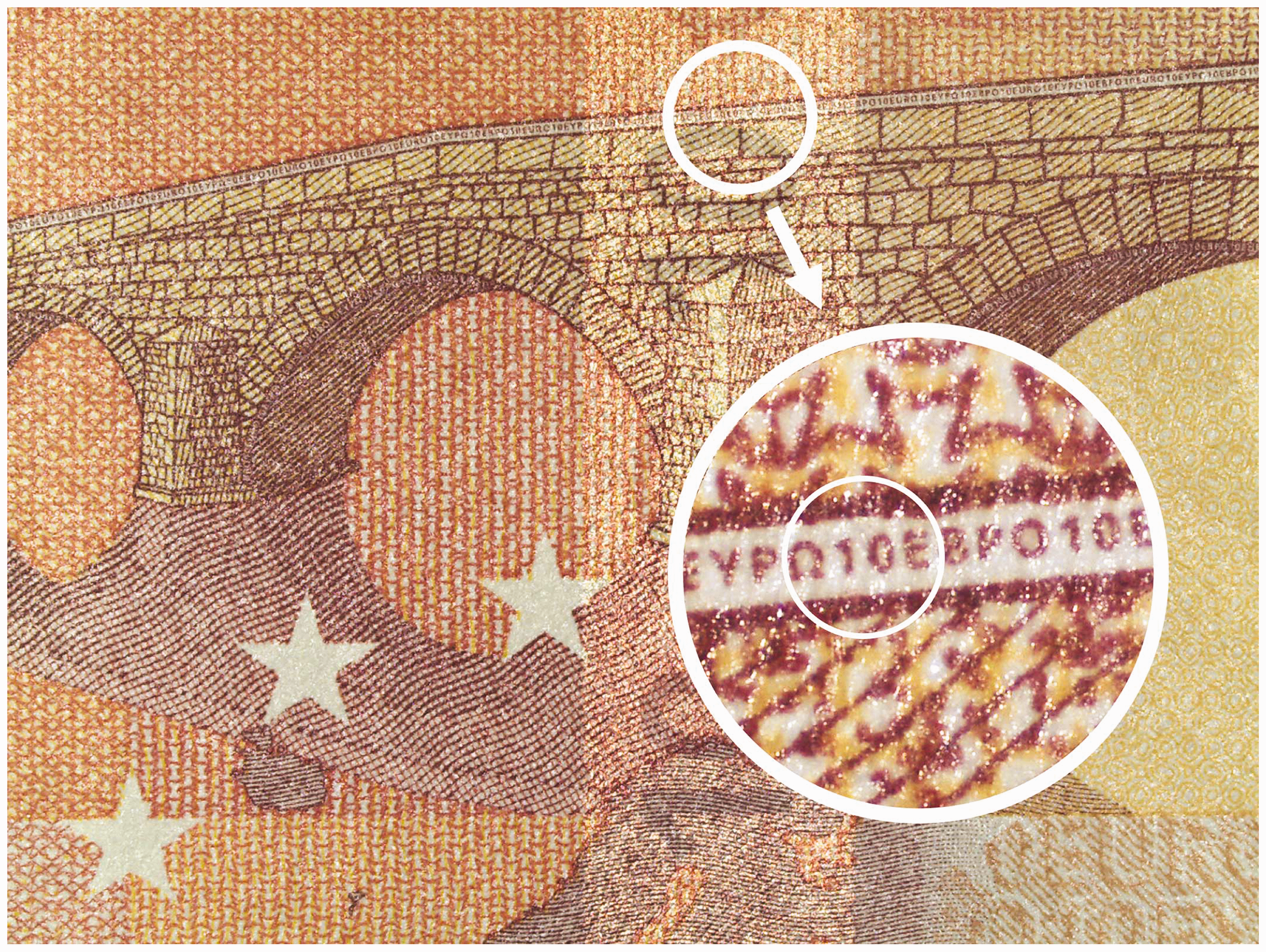
To validate this test, 46 hand surgeons (range of age 30–65 years, mean 45 years) performed this test in comparison with the validated E-optotype test from Perrin et al. (2016) using their own loupe systems. Sixteen of the surgeons used Galilean, 30 used Keplerian loupes. The correlation between the two tests (banknote/E-optotype test) was evaluated according to the method of Kendall, which can correlate continuous and binary results with Kendall’s rank correlation coefficient. The sensitivity and specificity of the 10 EUR test (yes/no) was calculated to determine whether surgeons detected a size smaller or larger (respectively equal) than the median of the validated E-optotype test of the peer group.
We found that Kendall’s rank correlation coefficient between the two tests was 0.608 (95% confidence interval: 0.436, 0.743), which indicates a moderate positive correlation. The null hypothesis that the two tests do not correlate was rejected with high significance (p < 0.01). The banknote test allowed for the ranking of a surgeon’s vision with high sensitivity (0.808) and specificity (0.850) in relation to the validated median of the entire peer group (Figure 2). This result reveals the suitability of the 10 EUR-test as a triage test for surgeons using loupes.
In the two-by-two table, the banknote test with the standard loupes resulted in an almost equal distribution of yes (24 surgeons) and no (22 surgeons). The banknote test evaluates with high sensitivity and specificity the visual performance of a surgeon relative to the peer group.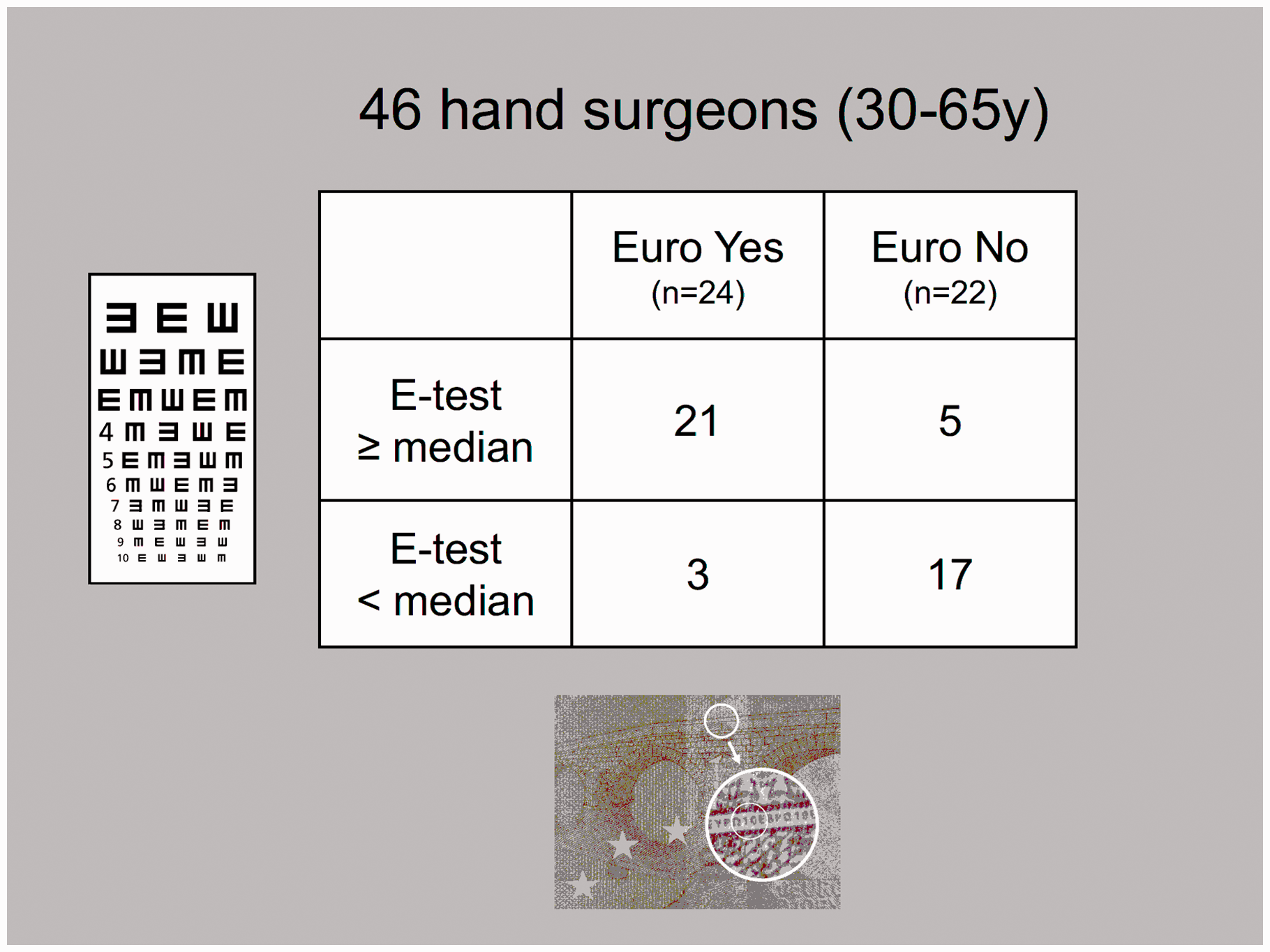
Visualization of the operating field is an obvious precondition to perform surgery (Stanbury and Elfar, 2013). A valuable threshold of required acuity is not scientifically defined, but the proposed test may be a pragmatic and available screening tool to reveal subtle visual constraints. Furthermore, it can prompt additional optical examination by an optometrist or change to an adequate magnification device. Presbyopia is an inevitable part of a surgeons’ professional life and deserves periodic assessment.
Footnotes
Acknowledgements
The authors would like to thank Lukas Martig and Gabriel Fischer (significantis GmbH, Bern, Switzerland) for the statistical analysis.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was conducted in accordance with all the provisions of the local human subject’s oversight committee guidelines and policies of the local ethics committee. KEK Kantonale Ethikkommission Bern, Murtenstrasse 31, CH-3010 Bern, Req-2017-00818.