
Abstract
We report the outcomes of zone 2 tendon repairs in 60 fingers using a strong core suture, sparse peripheral stitches and early active motion. From January 2014 to April 2016, we repaired 60 flexor digitorum profundus tendons with a tensioned 4-strand or 6-strand core suture and three to four peripheral stitches. The A2 or A4 pulleys were vented as necessary. Following early active flexion of the repaired tendons, no repairs ruptured and 52/60 (87%) fingers recovered to good or excellent function using the Tang criteria after follow-up of 8–33 months. We conclude that tensioned multi-strand strong core repairs only require sparse peripheral stitches and are safe for early active flexion. Standard peripheral sutures are not necessary. The core sutures should be properly tensioned to prevent gapping at tendon repair site and pulleys should be sufficiently vented to allow tendon motion.
Introduction
Traditional teaching has been that a standard peripheral suture is necessary to supplement a core suture in repairing flexor tendon lacerations in zone 2 (Caulfield et al., 2008; Moriya et al., 2017; Rigó et al., 2017; Tang, 2005, 2007). A variety of peripheral sutures has been proposed and some surgeons used rather complex ones (Rigó and Røkkum, 2016; Sirotakova et al., 2004; Wieskötter et al., 2018). Giesen et al. (2018) reported that without a peripheral suture a 6-strand core suture was sufficient to prevent gapping and rupture during early active finger flexion exercise. Their ultrasound examination revealed no gapping during early active motion in the absence of peripheral sutures (Reissner et al., 2018).
From January 2014 to April 2016, we repaired 60 flexor digitorum profundus (FDP) tendons using a tensioned 4-strand or 6-strand core suture and three to four peripheral stitches. These fingers underwent early active motion and none of the repairs ruptured. We report outcomes of these patients with a mean follow-up of 13 months (range 8–33).
Patients
Inclusion criteria
We included a consecutive series of patients with complete divisions of the FDP tendon in zone 2 from January 2014 to April 2016. We excluded cases with: (1) complete, or incomplete, amputation of fingers; (2) tendon injuries with concomitant phalangeal fractures or joint dislocations or skin or soft tissue defect in the involved finger(s); (3) accompanying extensor tendon injury; (4) segmental loss of the flexor tendon >1 cm; or (5) wound contamination with a great risk of infection.
Patients with concomitant digital nerve injuries in the finger were included, provided the digital nerve could be repaired directly. Injuries with concomitant unilateral digital artery division were also included in the study, as long as the blood supply of the finger was good.
Eleven patients were not followed for >2 months because they were unable to come back for further follow-up. Therefore, 41 patients with tendon repairs in 60 fingers were included in this report.
Surgical methods
Surgeons with expertise levels 2 and 3 according to the criteria of Tang and Giddins (2016), with assistance from other junior surgeons, performed the procedures. All fingers were repaired under axillary block with pneumatic tourniquet control; six patients (seven fingers) were repaired under local anaesthesia (1% lidocaine with epinephrine) without using a tourniquet (Lalonde, 2017). The wounds were washed thoroughly before proceeding to tendon repair.
The primary wound in the finger was extended by about 2 cm using a Bruner incision to expose the tendon sheath. The sheath was opened through a small midline incision of 1.5–2 cm in length. Flexion of the wrist and metacarpophalangeal (MP) joints was used initially to advance the retracted FDP tendon stump into the sheath opening. When this technique was not successful, a separate incision at the distal palmar crease was made to find the proximal stump, which was then fed distally to the wound site. The proximal tendon stump was then advanced distally through the intact sheath to approach the distal end of the tendon. The proximal tendon stump was immobilized with a 25-gauge hypodermic needle passed through the proximal sheath.
The FDP tendon was repaired with a 4-0 looped suture (Holycon, Nantong, Jiangsu, China) using a 4-strand U-shaped core suture (Cao and Tang, 2005). Core suture purchases were at least 7 mm, ideally 10 mm, from the tendon ends (Figure 1). To increase gapping resistance, we always added slight tension to the core suture, with slight bunching of the repair, by producing a 10% tendon-segment shortening or 30% increase in tendon diameter at the repair site (Wu and Tang, 2014). After completing the core suture repair, we performed digital extension-flexion testing (Tang, 2018a, 2018b; Tang et al., 2013, 2017). If any gap occurred between the tendon ends when the finger was passively extended fully by the operator or with active finger motion by the patient, another core suture was inserted, converting the core repair to a 6-strand core suture of M-shaped configuration (Tang, 2007). Eventually, 18 fingers had a 4-strand core suture repair and 42 fingers had a 6-strand core repair. Three to four passes of simple running peripheral 6-0 nylon suture sparsely located palmarly extending to lateral aspect of the tendon were added after a 4-strand U-Tang repair methods. The peripheral sutures included the dorsal aspect in only a few FDP tendons because the dorsal aspect was not often easily accessible. For tendons with a 6-strand M-Tang repair, two to three simple running 6-0 nylon stitches or separate figure-of-eight stitches, or two figure-of-eight stitches plus one single stitch, were then added to complete the repair. The peripheral stitches were added on the palmar and lateral aspects of the tendon but not usually on the dorsal aspect of the tendon (Figure 1). We did not repair the flexor digitorum superficialis (FDS) tendon in any of the fingers in order to allow greater space within the tendon sheath for FDP tendon gliding. In patients with complete FDS tendon cut in zones 2B and 2C, each FDS tendon stump was excised 2 cm proximal to its insertion on the middle phalanx.
Four-strand U-Tang or 6-strand M-Tang core repairs and sparse peripheral stitches. (a) One looped suture is used to complete a U-shaped 4-strand repair. (b) Addition of another looped suture in the middle part of the tendon to make a M-shaped 6-strand repair (M-Tang repair). (c) The sparse peripheral sutures with either 4- or 6-strand core suture include: sparse palmar running suture; separate stitches (shown in the left); two or three figure-of-eight sutures; or a mixture of two figure-of-eight with a separate stitch (shown in the right).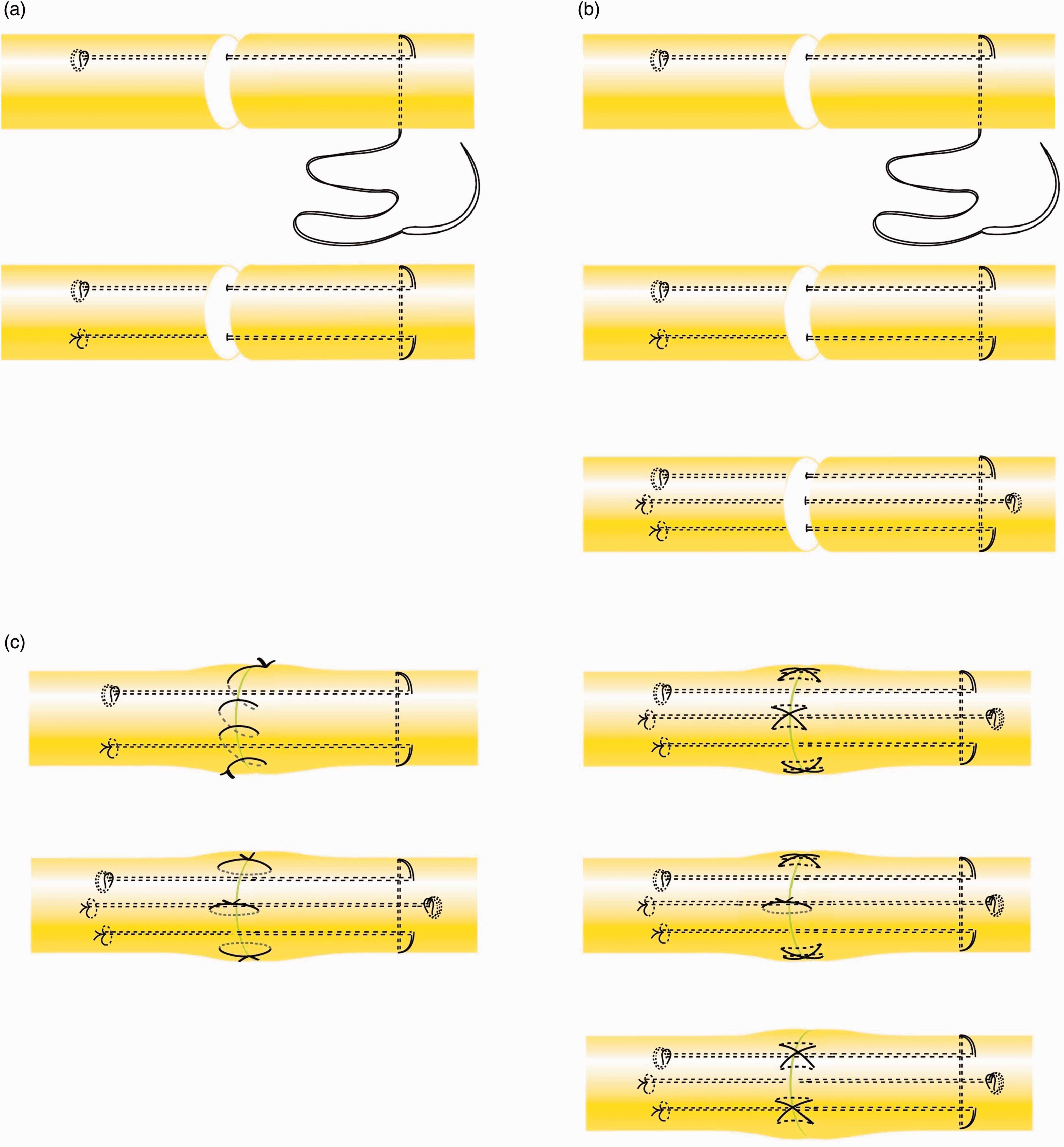
The synovial sheath was not repaired. When the tendon repair was located near the A4 pulley (14 fingers), the A4 pulley was vented entirely to make the repair easier and avoid restriction of tendon gliding (Kwai Ben and Elliot, 1998; Moriya et., 2016b; Zhou et al., 2017). If the injury site was under, or in the vicinity of, the A2 pulley (40 fingers), one-half to two-thirds of the A2 pulley was vented. All of the venting was done in the volar midline and included excision of a small part of the adjacent sheath (Tang, 2014; Moriya et al., 2016a) (Figure 2). Finally, any divided digital nerves were repaired and the skin wound closed.
An example of the repaired FDP tendon after a 6-strand core suture with sparse separate palmar peripheral stitches. The core suture repair was with tension and distal 2/3 of the A2 pulley was vented to allow ample tendon gliding.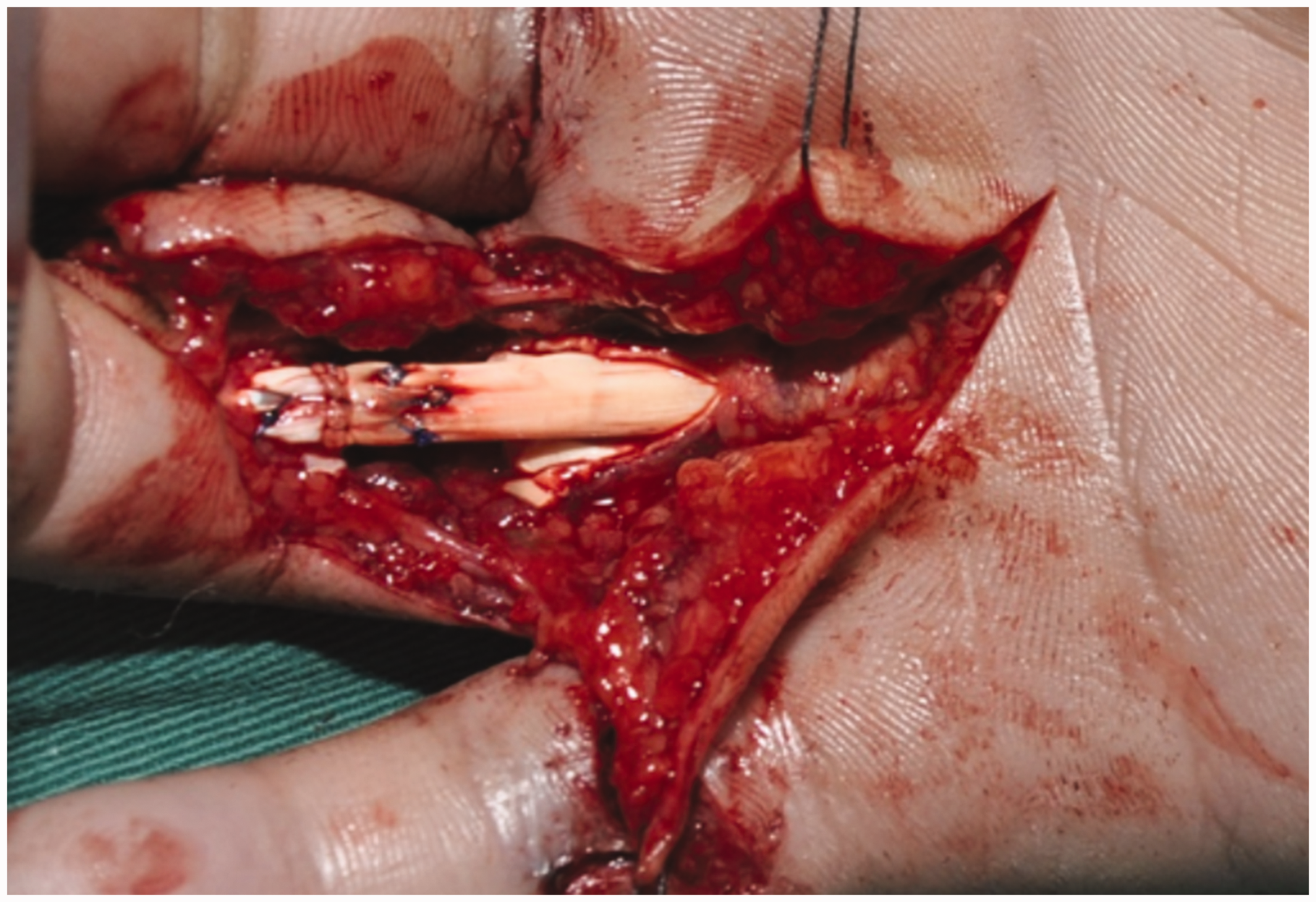
Postoperative rehabilitation
After surgery, the hand was protected in a splint 6–8 cm above the wrist to the tip of the fingers with the wrist in 20–30° of flexion, the MP joints in 30–50° of flexion and the interphalangeal joints fully extended.
The mobilization protocol used was a combined passive–active motion protocol. Mobilization started 4 days after surgery. The fingers rested in extension against the splint between exercise sessions, which were performed 5–6 times per day. A full range of passive digital motion (repetitions) was carried out 10–30 times before initiation of active digital flexion at each session. During the first and second weeks after surgery, active finger flexion was restricted to one-third of the total range of finger flexion from the fully extended position. The range of active flexion was increased to two-thirds in week 3 and full flexion was achieved in week 4. Each session included 20–30 repetitions of active motion. The splint was removed 6 weeks after surgery. Passive then active exercises were continued for 10–12 weeks after surgery.
Follow-up and functional assessment
The mean follow-up time was 13 months (range 8–33). The functional outcomes at the final follow-up were evaluated using the Tang criteria (2013). Rupture of the repairs and the fingers which needed tenolysis were also recorded. The total range of active motion of the interphalangeal joints of the injured fingers was calculated.
Results
Patients included
A total of 60 fingers in 41 consecutive patients (14 female and 27 male) met the inclusion criteria of this study. The mean age of patients was 37 years (range 16–60). The injuries included 19 index, 17 middle, 14 ring and 10 little fingers with complete FDP division in zone 2 as a result of sharp injuries. Four patients had flexor tendon repairs in two fingers, six had tendon injuries in three fingers and one had tendon injuries in four fingers. Thirty-nine fingers had associated digital nerve and/or artery injuries. All repairs were performed within 7 days after injury except two cases, in which the time between injury and operation was 21 and 31 days, respectively.
The good and excellent rates of functional recovery
The outcomes of the 60 fingers based on range of active motion of the fingers.
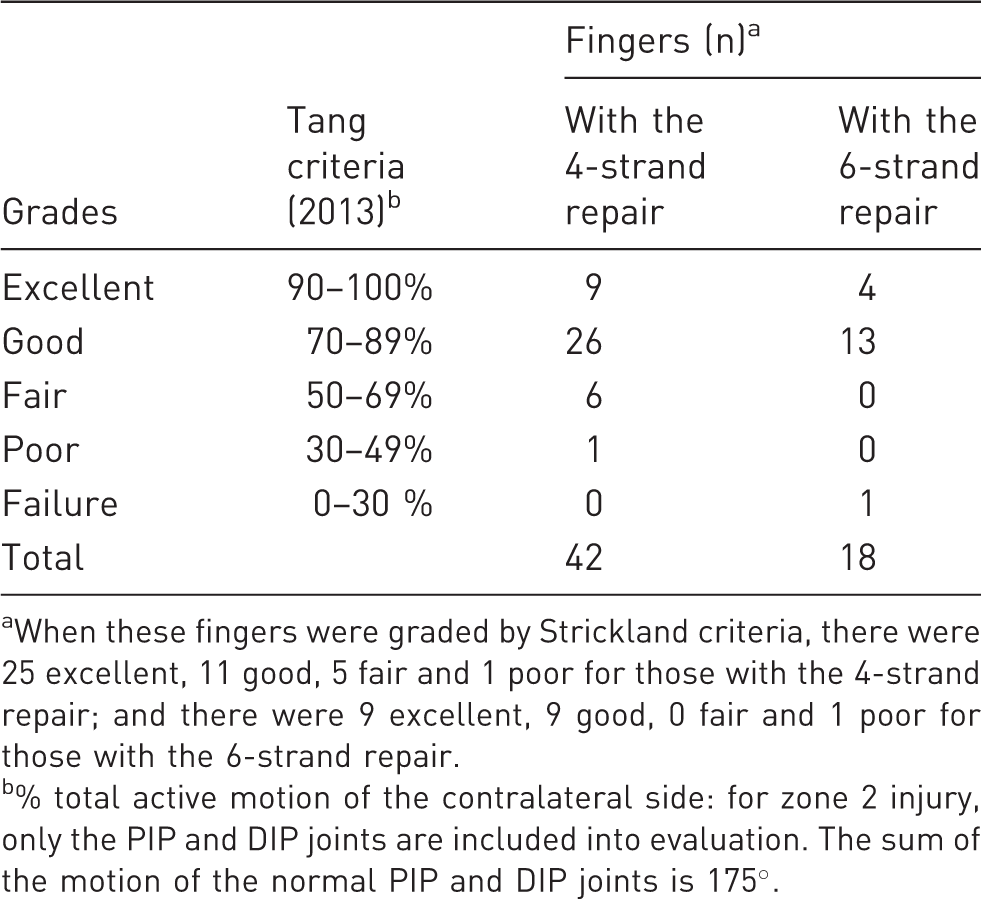
When these fingers were graded by Strickland criteria, there were 25 excellent, 11 good, 5 fair and 1 poor for those with the 4-strand repair; and there were 9 excellent, 9 good, 0 fair and 1 poor for those with the 6-strand repair.
% total active motion of the contralateral side: for zone 2 injury, only the PIP and DIP joints are included into evaluation. The sum of the motion of the normal PIP and DIP joints is 175°.
Repair rupture or tenolysis
None of the 60 fingers ruptured the repair. One finger rated a failure needed tenolysis 4 months after primary repair. This was a 56-year-old man with a flexor tendon repair in the right little finger with a 6-strand M-Tang method the following day after complete FDP tendon laceration in zone 2A. Follow-up 6 months after tenolysis indicated active distal interphalangeal joint flexion 25°, proximal interphalangeal joint flexion 60° and MP joint flexion 90°. The function after tenolysis was fair.
The ranges of active interphalangeal joint motion
The range of active interphalangeal joint motion of the fingers was 152° ± 32°. Extension deficits of a mean of 18° (range 5–70) occurred in 14 fingers (23%).
Discussion
Without a standard peripheral suture, we had no repair rupture in a consecutive series of 60 zone two flexor tendon repairs, after exclusion of 11 patients who we could not assess for final follow-up. The good and excellent results recorded in 52 of 60 fingers were comparable to those with more standard peripheral sutures. Our results indicate that peripheral sutures are not important when a well-tensioned strong core repair has been implemented.
Clinically, complex peripheral sutures are hard to perform, especially on the dorsal aspect of the repaired tendon, and a suture exposure may lead to adhesion formation and increase gliding resistance during early active motion. In contrast, sparse peripheral sutures save operating time, decrease suture exposure and simplify surgical procedures. We suggest that the term ‘circumferential suture’ should be avoided when these sparse ‘peripheral sutures’ are located on only the palmar or lateral aspects of the tendon. ‘Peripheral suture’ or ‘peripheral stitches’ are preferred for such sparse volar or lateral stitches.
The peripheral sutures serve to tidy up the repair site and prevent gapping (Tang et al., 2017). The function of the peripheral suture is largely replaced by tensioning the core sutures and the use of multi-strand repairs (Chen et al., 2018; Hay et al., 2018; Kozono et al. 2016; Lalonde, 2017; Lim et al., 2018; Myer and Fowler, 2016; Pan et al., 2017; Wu and Tang, 2014). The tension over the core suture serves to resist gapping and a multi-strand repair adds stability of repair constructs, thereby tidying up the junction of the repair site. In the report by Giesen et al. (2018) of ‘core suture only’ tendon repairs, all core sutures had knots outside the tendon surface, not between two repaired tendon ends. Chang et al. (2018) demonstrated that placement of knots between tendon ends reduced the force to create gapping in experimental settings. In all our patients, the knots of the core sutures were all located on the tendon surface, rather than between two tendon stumps. This appears to be important to the repair without peripheral suture or with sparse peripheral stitches.
A key in making an effective core suture is to have certain tension, which could make the approximation site of two tendon ends somewhat bulky. However, with the critical pulley vented, potential for snagging of the repair sites decreased even the junction site has certain bulkiness, which would not cause snapping but would prevent gapping at the repair site. If the tendons were not repaired with some tension and without a standard peripheral suture, the tendon could easily gap. Therefore, few peripheral sutures should only be used when a tensioned strong core suture has been used for tendon repair.
In our patients, we did not perform the standard simple running peripheral suture in the majority of fingers, but we decided according to degrees of smooth approximation after core suture. For instance, after 4-strand repairs, approximation is usually loose and rough, so we added deep running continuous peripheral suture palmarly and laterally and sometimes dorsally. Also, after 6-strand repairs, approximation is usually much better and acceptable without a peripheral suture, but the degree of approximation also varied individually, so we made individual decisions. If the approximation is very good, we used 2–3 simple stitches with or without a separate figure-of-eight suture palmarly and laterally, but without dorsal peripheral stitches. If the approximation is not good in general, we added a sparse running suture.
In this study, we are unable to analyse the outcomes of the 4-strand versus 6-strand repairs statistically because of a lack of sufficient power after division into the two groups. In the period of study, we noted greatly improved approximation and smoothness of tendon end junctions and greater repair site stability after a 6-strand compared to 4-strant core suture. After a 6-strand core suture, we only needed two to three simple stitches and/or figure-of-eight repairs as peripheral sutures, which were easy to add. These observations prompted us to use the 4-strand repair less frequently and to use the 6-strand M-Tang repair in most of our FDP tendon repairs since mid-2017. The 6-strand core suture with two to three peripheral stitches is currently our preferred way of repairing a FDP tendon laceration.
Footnotes
Acknowledgements
We express sincere gratitude to Dr Ya Fang Wu in the Hand Surgery Research Center, Affiliated Hospital of Nantong University for her beautiful illustrations of the surgical methods in ![]() . The data in this report are from Yixing Hospital, with the lead author (ZJP) leading the surgical team and follow-up of patients.
. The data in this report are from Yixing Hospital, with the lead author (ZJP) leading the surgical team and follow-up of patients.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors’ clinical work was partially funded by Jiangsu Medical Research Center.