
Abstract

Dear Editor,
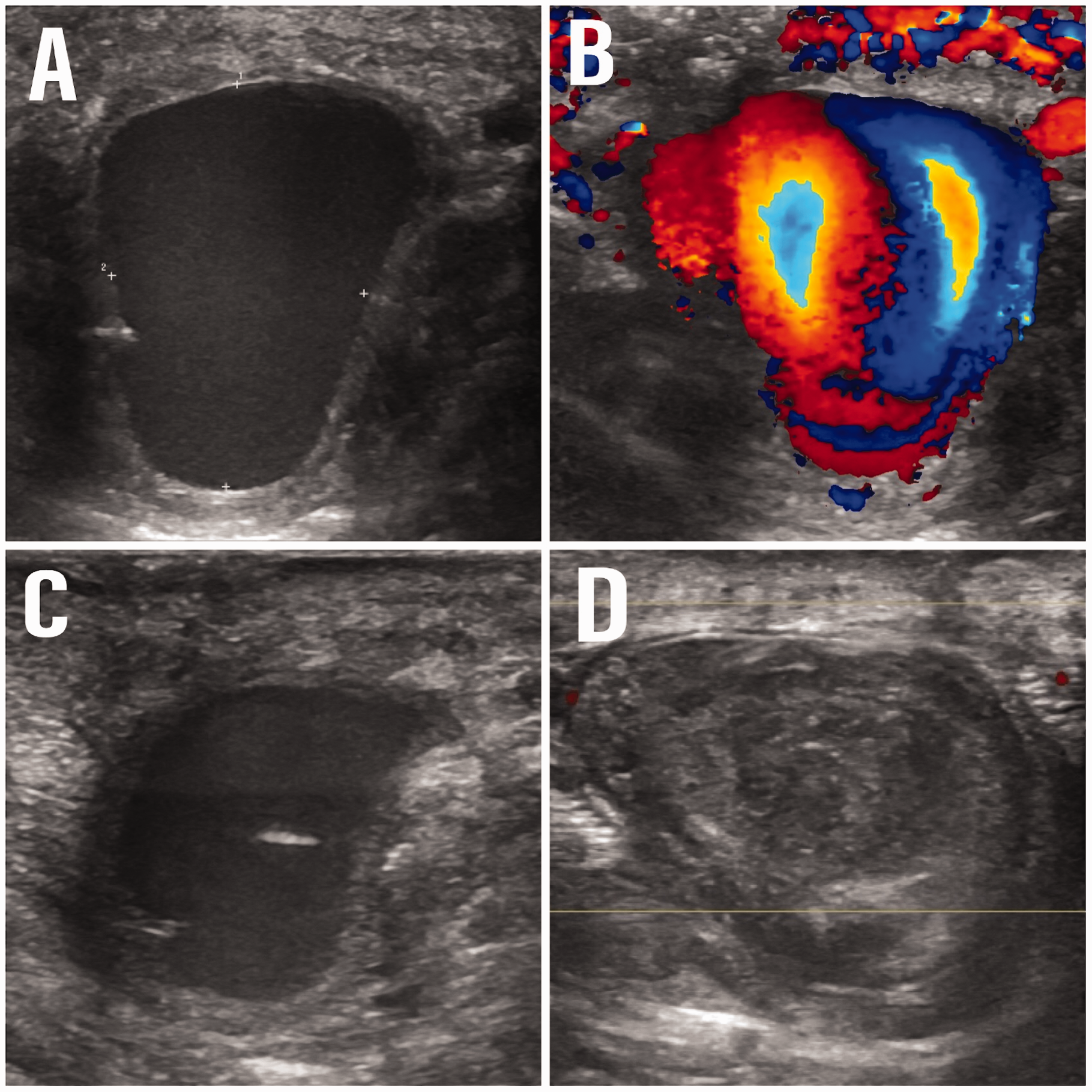
An 86-year-old male sign-maker was cutting a plexiglass sheet which shattered, penetrating his hand over Guyon’s canal causing a 1 cm bleeding wound. He had no neurological deficit and satisfactory perfusion of the digits with a normal Allen’s test and capillary refill. The wound was sutured after excluding a foreign body. Past medical history included atrial fibrillation, a pacemaker for heart block and he was taking the anticoagulant rivaroxabon. He attended 3 weeks later with spontaneous significant bleeding. A computed tomographic (CT) angiogram revealed a pseudoaneurysm of the superficial palmar arch between the flexor tendons of the middle and ring fingers (Figure 1). High resolution ultrasonography (US) confirmed the presence of a 21 × 19 mm pseudoaneurysm with ulnar artery inflow and a classical ‘yin-yang’ sign (Figure 2).
Three-dimensional reconstruction of computed tomographic angiogram showing a pseudoaneurysm in the palm (arrows) arising from the ulnar artery. (a) Ultrasound image showing anechoic pseudoaneurysm in the palmar soft tissue. (b) Colour Doppler image showing turbulent internal flow producing the classic ‘yin yang’ sign, consistent with a pseudoaneurysm. (c) Ultrasound image showing the needle tip (echogenic dot) within the pseudoaneurysm. (d) Follow-up ultrasound image after thrombin injection confirming complete exclusion of the lesion with echogenic thrombus filling the pseudoaneurysm.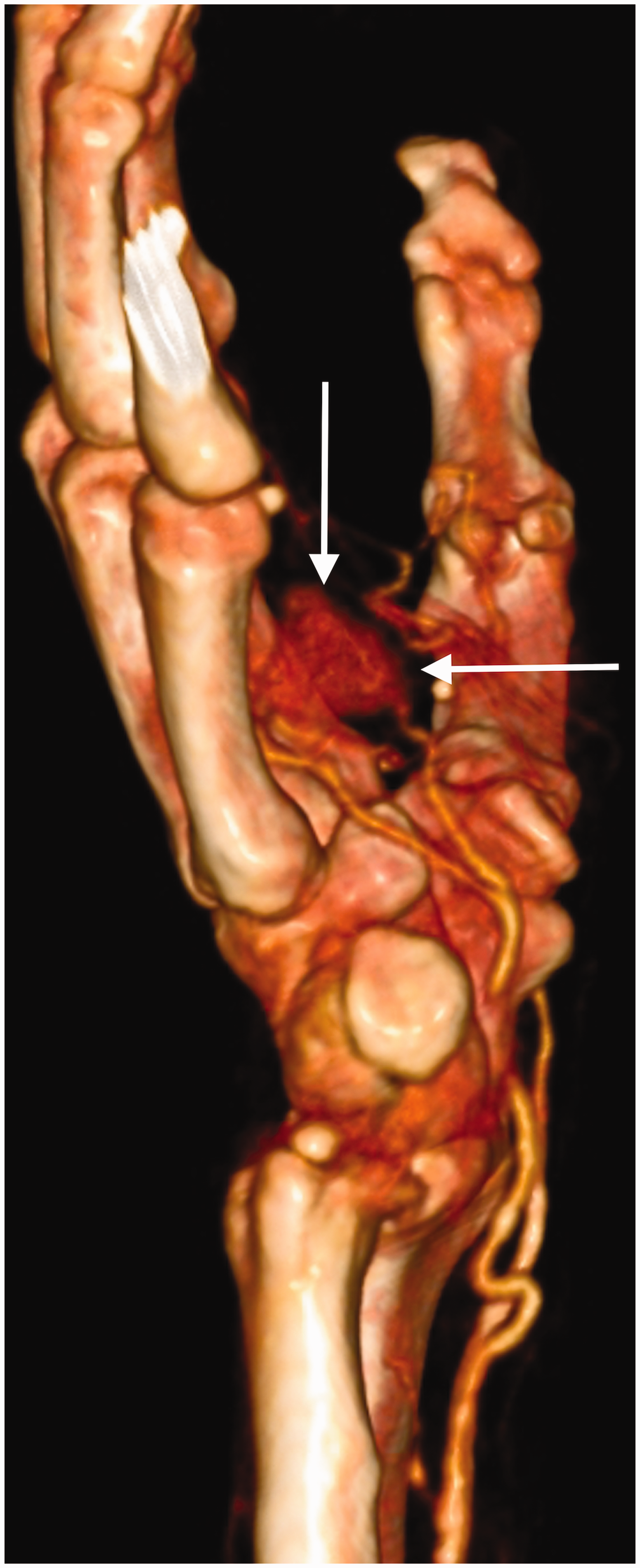
A consultant interventional and musculoskeletal radiologist with experience of treating pseudoaneurysms in the groin used US to map the anatomy of the pseudoaneurysm sac, identify the inflow and confirm patency of the digital artery outflow at the margin of the sac. A fine bore (25 gauge) needle was introduced into the pseudoaneurysm, adjacent to the inflow. Human thrombin 5000 IU in 10 ml normal saline (Floseal; Baxter Healthcare, 8010 Zurich, Switzerland) was injected in aliquots of 0.1 ml, using a 1 ml syringe. The growing thrombus ball at the needle tip was monitored in size, until the entire false aneurysm was excluded (after 0.5 ml thrombin had been injected), ensuring preserved flow throughout into the digital artery outflow on a Doppler scan. Follow-up US at 3 days showed partial recanalization of the aneurysmal sac. The injection was repeated, using the same technique to achieve complete thrombosis. The patient made a good recovery after the second injection with no further bleeding and returned to normal function. A further US confirmed complete thrombosis of the pseudoaneurysm.
Pseudoaneurysms occur after arterial wall damage leading to extraluminal blood flow and haematoma formation. Unlike true aneurysms, pseudoaneurysms do not contain all layers of the arterial wall. They are rare in the hand despite the high incidence of penetrating trauma. Standard treatment includes exploration with microsurgical arterial repair or resection and grafting. US-guided thrombin injection has been used extensively for femoral pseudoaneurysms (Krueger et al., 2005) and in single cases in the forearm (Polytarchou et al., 2016) and hand (Bosman et al., 2016). It is a generally safe and reliable procedure that does not require use of the operating theatre. It is around 97% successful in femoral pseudoaneurysms, but less so in anticoagulated patients (Powell et al., 2002).
The US-guided thrombin injection technique appears to be a safe treatment for palmar artery pseudoaneurysms. It is particularly useful for patients who are unable to tolerate lengthy microsurgical procedures.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.