
Abstract
We performed a cadaver study to evaluate how six different static heat-moulded splints affect flexor tendon relaxation. Each splint positioned the wrist and metacarpophalangeal (MCP) joints in different positions. We evaluated the tendon relaxation in 12 fresh adult cadaver forearms by measuring the flexor tendon displacement between two solid markers for each splint. The wrist position ranged from 30° flexion to 45° extension and the MCP joints from 30° to 60° flexion. For each splint, tendon relaxation was achieved relative to the neutral reference position. Tendon relaxation was greatest when the MCP joints were positioned in 60° flexion. We also noted the persistence of tendon relaxation when the wrist was positioned in extension (30° or 45°) as long as MCP joint flexion was maintained (30° or 60°). We conclude that the wrist extension with the MCP joints flexion may optimize tendon relaxation during immobilization after flexor tendon repairs.
Introduction
Multistrand repair techniques have significantly improved the quality and strength of flexor tendon repairs in the hand (Cao et al., 2005; Dona et al., 2004, Sandow and McMahon, 2011; Savage and Risitano, 1989). However, postoperative rehabilitation protocols and immobilization positions are numerous. Rehabilitation protocols should be customized to the severity of injury, repair quality and patient characteristics (Peck, 2012). Early active motion of primary flexor tendon repair is used when the patient complies with the protocol (Cullen et al., 1989; Elliot, 2002; Rigó et al., 2017, Sandow and McMahon, 2011; Tang, 2007, 2018a). Savage (1988) suggested that 45° of wrist extension is the best position to reduce the forces required during the work of digital flexion when using an early active mobilization protocol. Peck et al. (2014) reported a short dorsal splint to allow maximal wrist flexion and up to 45° of wrist extension with a block to 30° of metacarpophalangeal (MCP) joint extension. In this study, we evaluated how six different static heat-moulded splints impacted tendon relaxation using cadaveric hands.
Methods
Design of splints
We analysed and compared six different static heat-moulded splints that placed the wrist and MCP joints in six different positions. The interphalangeal (IP) joints were always straight. The first splint immobilized the wrist at 0° and the MCP at 60° flexion (0°/−60° splint). This splint was considered the reference splint in our current clinical practice. Five other splints were made to immobilize the wrist at 30° flexion and MCP at 60° flexion (−30°/−60° splint), the wrist at 30° extension and the MCP at 60° flexion (+30°/−60° splint), the wrist at 30° extension and MCP at 45° flexion (+30°/−45° splint), the wrist at 30° extension and the MCP at 30° flexion (+30°/−30° splint), and the wrist at 45° extension and MCP at 30° flexion (+45°/−30° splint) (Figure 1). Designing and measurement of angles (goniometer, Prestige® Medical, Jasper, GA, USA) for each splint was performed by an independent examiner (AT) with more than 10 years of clinical experience in physical and rehabilitation medicine.
Design of the different static heat-moulded splints positioning the wrist and MCP joints in different positions. (a) The wrist could be positioned at 30° flexion, 0°, 30° extension or 45° extension. (b) MCP joints could be positioned at 30° or 45° or 60° flexion.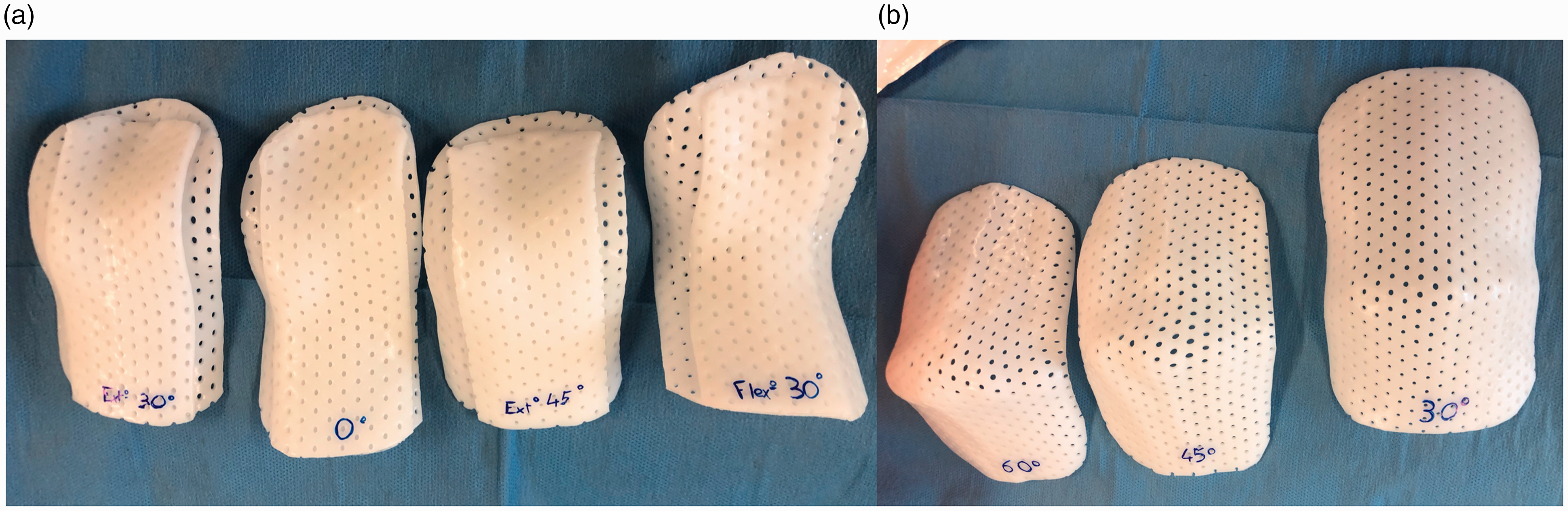
Study protocol
We carried out a cadaver study using 12 fresh adult elbows, forearms and hands provided by the anatomy laboratory of our medical school. The specimens included six right upper limbs and six left. The limbs were disarticulated at the shoulder and prepared in a manner similar to that described by Pollock et al. (2010). None had any pre-existing lesions of the hand, fingers or wrist. All wrists were prepared by two senior surgeons (LA and RD, Level 4, specialist – highly experienced, Tang and Giddins, 2016) using the same protocol, which consisted of longitudinal incisions along the entire volar aspect of the forearm and wrist to locate the flexor tendons (flexor digitorum superficialis [FDS] and flexor digitorum profundus [FDP]). First, a 0.45-kg weight was applied in the forearm axis to the muscle bodies of the flexor tendon unit to simulate physiological tension. Next, we placed two markers. The first was fixed above the medial epicondyle (fixed marker) and the second, 20 cm distally (movable marker). The resting position of the hand and wrist before application of each splint was standardized, with the wrist, MCP and IP at 0° (neutral reference position). We used a Fiberwire™ 2-0 (Arthrex®) suture to whip stitch all the flexor tendons (FDP and FDS); this served as the second marker (Figure 2). The limb was then positioned horizontally on a specially designed workstation to stabilize it. Each splint was tested on each upper limb.
Photographs of the study protocol. (a) Incisions along the entire volar aspect of the forearm and wrist to locate the flexor tendons. The two markers: fixed marker above the medial epicondyle and movable marker at 20 cm distally (movable marker). (b) A 0.45 kg weight was applied in the forearm axis to the muscle bodies of the flexor tendon unit to simulate physiological tension (arrow).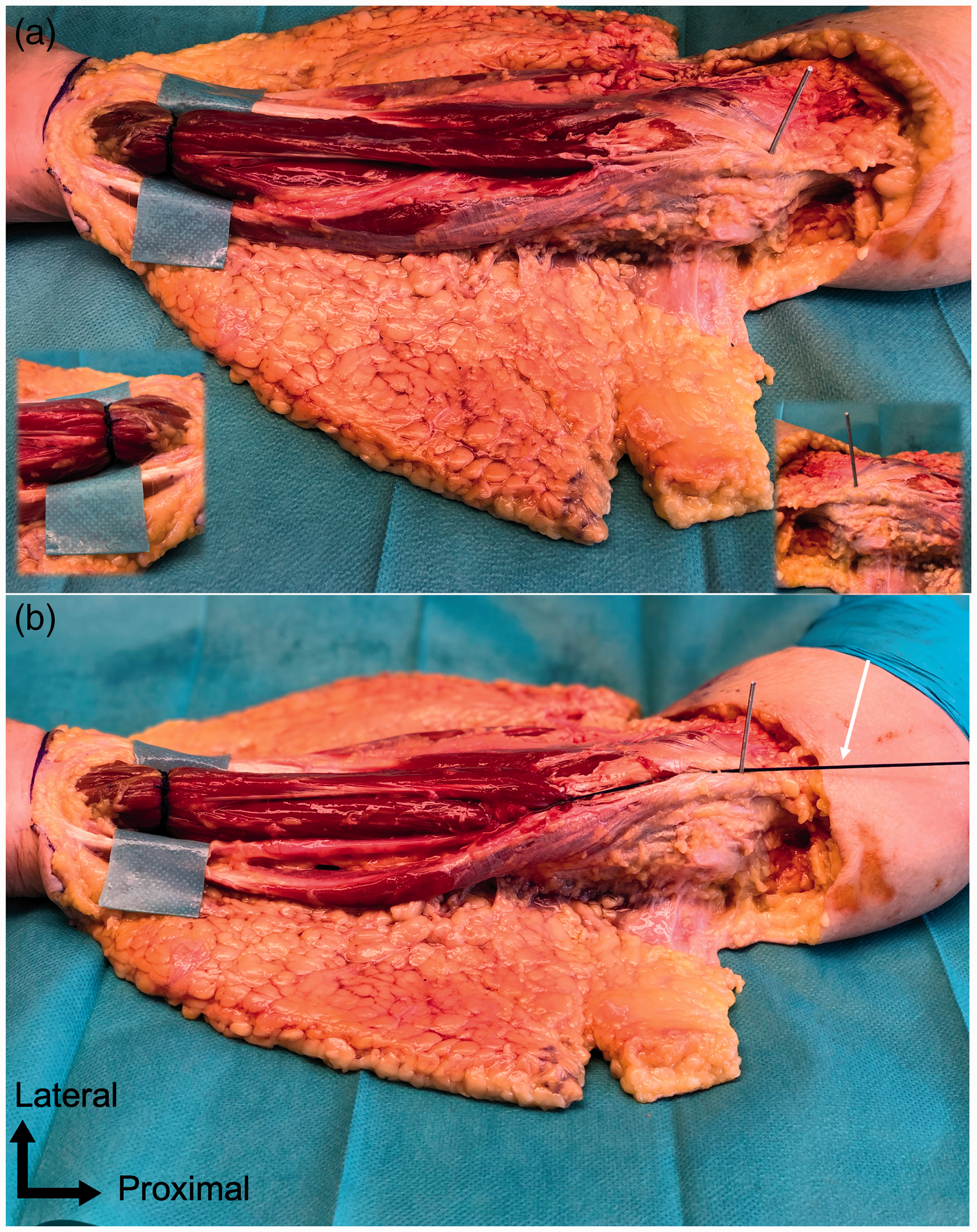
Tendon excursion measurement
To evaluate tendon excursion, an independent examiner calculated the displacement, in millimetres, of the second marker induced by the position of each splint. Proximal displacement (toward the medial epicondyle) was rated positively and considered a relaxation effect; a distal displacement (toward the hand) was rated negatively and considered a tension effect (Figure 3).
An example of the neutral reference position (a) and tendon relaxation with the 0°/−60° splint (b) and the +30°/−60° splint (c).
Statistical analysis
The recorded data were summarized using mean values and ranges. The mean values obtained were compared using paired Student’s t-test. p < 0.05 was considered statistically significant.
Results
Tendon relaxation (mean and range) for the different type of splints (n = 12) compared to the reference 0°/−60° splint.

+: extension; −: flexion.
When we compared the results between the 0°/−60° splint (reference splint) and the other splints (Table 1), there was no significant difference in tendon relaxation with the −30°/−60° splint (p = 0.07). However, we found a significant difference in tendon relaxation with all the other splints positioning the wrist in extension (+30° and +45°) (p < 0.05). The smallest difference was observed with the +30°/−60° splint (p = 0.024).
Discussion
Our measurements indicate that the greatest tendon relaxation may be induced as of 30° MCP flexion and is independent of wrist position, whether in flexion (30°), neutral (0°) or in extension (30° and 45°). However, tendon relaxation seemed most effective when the MCP joints were positioned in 60° flexion. We did not find a significant difference between our reference splint (0°/−60°, current clinical practice) and the splint with a slightly flexed wrist (−30°/−60°). Furthermore, comparison of our reference splint with the other splints showed the least tendon relaxation with the +30°/−60° splint.
Leiber et al. (1996, 1999) and Zhao et al. (2002) suggested the forces exerted on flexor tendons are dependent on wrist position and there is increased passive tendon excursion during wrist tenodesis. Savage (1988) examined the influence of wrist position on the forces required to move the IP joints and concluded that 45° of wrist extension is the optimal position to minimize the work of digital flexion when using an active mobilization protocol. However, this position is uncomfortable when wearing a splint for 6 weeks continuously. We consider the position in 30° wrist extension could be an alternative.
With regard to the MCP joint, we found tendon relaxation induced by the position at 30° flexion. According to Wehbé and Hunter (1985), 30° MCP flexion makes it easier to initialize flexion with the FDP tendons and to achieve differential sliding between the flexor tendons. Positioning the MCP joints in excessive flexion would bias active motion in favour of the proximal IP joints. Confining active motion to the proximal IP joint only would encourage adhesions between flexor tendons and patients would attempt distal IP joint flexion only at the end of its range (Peck et al., 2014). Active motion should be initiated from the distal IP joint; this is facilitated in most patients by positioning the wrist joint in 10° to 30°extension and the MCP joints in 30° flexion (Bigorre et al., 2018). In addition, wrist extension significantly increases the excursion of the FDP and FDS tendons relative to the neutral position or the flexion position (Amadio et al., 2005).
In our study, we analysed tendon relaxation on non-sutured tendons and this study remains an anatomical investigation. We therefore could not assess tendon healing or repair rupture in the different wrist and MCP positions. This was a cadaver study, which cannot include assessment of other factors, such as the patient’s co-morbidities, injury mechanism, associated injuries, size of suture used, impingement with pulleys, oedema, haematoma, joint stiffness, size of dressing and patient compliance. All these factors play a role in tendon relaxation and excursion after tendon repair clinically. Tendon displacement may suggest tendon relaxation, but we concede that it is not equal to tension reduction in tendon in vivo.
In recent publications, authors consider wrist position not important and the MCP joint is usually in a functional position (Giesen et al., 2018; Lalonde 2018; Moriya et al., 2017; Pan et al., 2017; Reissner et al., 2018; Tang, 2018a, 2018b). There were no or few repair ruptures associated with these positions (Giesen et al., 2018; Pan et al., 2017). It is also considered that after pulley-venting and strong surgical repair, exact position of splinting the wrist is no longer a major concern and out of splint active motion is practised (Tang 2018b). However, our current cadaveric study provides information that the +30°/−60° and +30°/−30° splints can be most favourable for tendon relaxation, an anatomical finding that may provide surgeons with information of tension on tendons at different wrist and hand positions.
Footnotes
Acknowledgements
The authors thank Dr. Joanne Archambault for English language editing assistance
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The participants had given informed consent for the use of their bodies for medical research.