
Abstract
Osborne’s modified decompression involves repairing Osborne’s ligament beneath the ulnar nerve after simple decompression for idiopathic cubital tunnel syndrome. In this retrospective interrupted time series, 31 patients underwent modified simple decompression and 20 patients underwent conventional simple decompression. In the modified simple decompression group, the ulnar nerve length was measured at operation in full elbow flexion and extension before and after repair of Osborne’s ligament. Ulnar nerve instability during elbow motion was measured using ultrasonography before operation and at 12 months after operation. In patients treated by modified simple decompression, the ulnar nerve length in full elbow flexion reduced significantly after repair of Osborne’s ligament. At 12 months after surgery, the grade of ulnar nerve instability was lower in the modified simple decompression group than in the conventional simple decompression group. The clinical outcomes did not differ significantly between the groups at 24 months after operation.
Introduction
The aetiology of cubital tunnel syndrome includes nerve compression, nerve traction, friction, nerve instability, ischaemia and the presence of osteophytes in the medial joint space (Baek et al., 2006; Filippi et al., 2002; Hicks and Toby, 2002; Palmer and Hughes, 2010). Although compression is considered a leading cause of idiopathic cubital tunnel syndrome, nerve traction is also cited as a possible cause. Although a direct correlation between idiopathic cubital tunnel syndrome and ulnar nerve traction has not been identified, evidence from experimental studies supports the presence of such a relationship. Several studies have reported that blood flow in the nerve is decreased by traction (Clark et al., 1992; Ogata and Naito, 1986) and the amplitude of nerve conduction is also decreased (Wright et al., 2001). Cadaveric studies have shown that substantial ulnar nerve excursion at the epicondyle is required during upper arm motion (range 14–16.4 mm) and that the strain is maximized during elbow flexion (range 5.2–29%) (Grewal et al., 2000; Hicks and Toby, 2002; Toby and Hanesworth, 1998; Wright et al., 2001). These results suggest that ulnar nerve traction usually occurs at the epicondylar level during elbow flexion and may lead to ulnar nerve symptoms by disturbing the blood supply and nerve conduction. In addition, unstable ulnar nerves tend to show toward increased irritability on provocation testing (Calfee et al., 2010), and it has been reported that ulnar nerve instability may occur after simple decompression (Matzon et al., 2016; Tang, 2017). To manage the ulnar nerve instability after simple decompression, some have recommended anterior subcutaneous transposition (Boone et al., 2015; Matzon et al., 2016), and others have attempted to stabilize the ulnar nerve at the retrocondylar groove (Hsu et al., 2013; Hurvitz et al., 2017; Tang, 2017).
Osborne described decompression of the ulnar nerve by dividing the aponeurosis between the two heads of flexor carpi ulnaris, which formed the roof of the cubital tunnel and later modified this simple decompression by suturing ‘the fascial band and aponeurosis’ beneath the nerve to prevent recurrence as a result of spontaneous regeneration (Osborne, 1970). Subsequent authors have referred to various structures as ‘Osborne’s ligament’, ‘Osborne’s fascia’ and ‘Osborne’s band’ (Wali et al., 2018). However, it is clear from his article that he regarded the fibrous tissue between the medial epicondyle of the humerus and the olecranon at the mouth of the cubital tunnel as being a major constrictive factor and this is what we refer to as ‘Osborne’s ligament’ (Figure 1).
Overview of the two surgical techniques used in this study. (a) Preoperative state. (b) Conventional simple decompression. (c) Osborne’s modified simple decompression.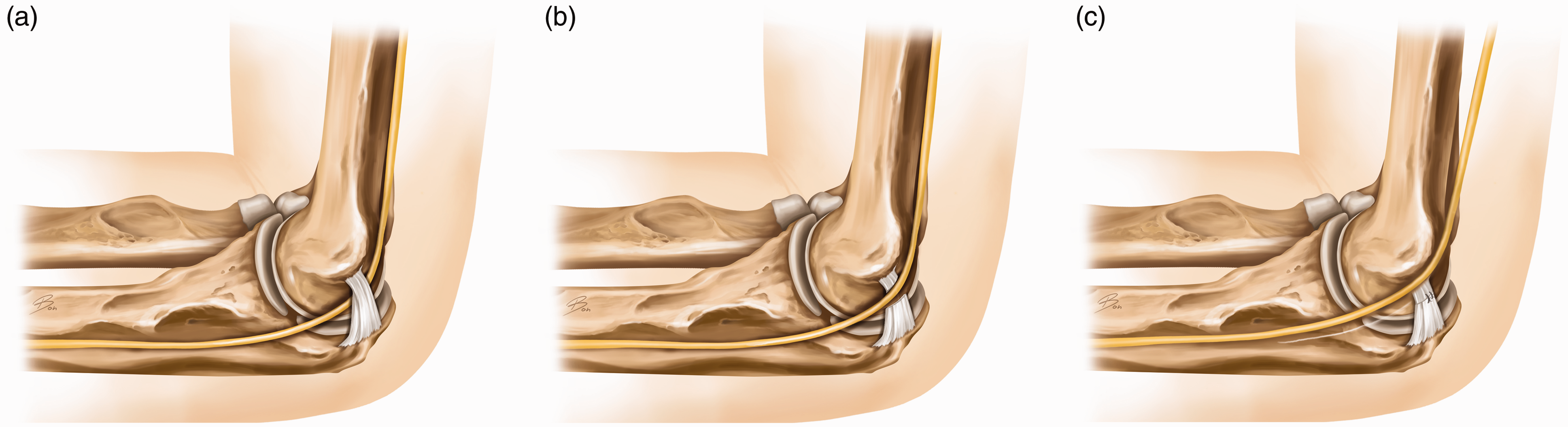
We hypothesized that repairing Osborne’s ligament beneath the ulnar nerve may reduce ulnar nerve traction and instability by preventing the return of the ulnar nerve to the retrocondylar groove. We aimed to understand how repairing Osborne’s ligament affects the ulnar nerve length, and also to determine whether Osborne’s modified simple decompression (MSD) and conventional simple decompression (CSD) show any differences in ulnar nerve instability and the clinical outcomes at 12 and 24 months after operation, respectively.
Methods
After approval of the study protocol by the Institutional Review Board, we retrospectively reviewed patients who underwent surgery for idiopathic cubital tunnel syndrome. Between March 2012 and December 2015, 89 consecutive patients underwent surgery for cubital tunnel syndrome at our institution. Eight patients who underwent additional nerve decompression surgery on the same side (n = 2, cervical root; n = 1, ulnar tunnel; n = 5, carpal tunnel) were excluded. We excluded patients with angulation deformity due to previous trauma (n = 8), limited range of motion (<90°) with stiffness (n = 2), severe degenerative arthritis on radiography (n = 5), revision surgery (n = 2) and follow-up <24 months (n = 6). Patients with diabetes mellitus (n = 7) were also excluded. Finally, 51 consecutive patients were included in the study, of whom 20 underwent CSD (CSD group, n = 20; treated between March 2012 and February 2014) and 31 underwent MSD (MSD group, n = 31; treated between March 2014 and December 2015).
Surgical methods
Surgery was carried out by two orthopaedic surgeons (JYB, SHK) who had been trained by the same senior surgeon. Both surgeons were level 4 (specialist – highly experienced) for the CSD technique and were level 2 (specialist – less experienced) for the MSD technique (Tang and Giddins, 2016). All surgical procedures were done under general anaesthesia. A tourniquet was applied to the upper arm, and a medial longitudinal skin incision was made along the medial epicondyle. Protecting the medial antebrachial cutaneous branch, the ulnar nerve was released from the medial intermuscular septum through dissection of Osborne’s ligament, to the fascia between the two heads of flexor carpi ulnaris. To preserve extrinsic blood supply the ulnar nerve was not stripped of soft tissue. In patients treated by MSD, adequate blood supply was identified in the loose areolar connective tissue between the ulnar nerve and surrounding soft tissue, and a 2 × 2 cm2 opening was made at the level of the medial epicondyle (Kleinman, 1999). The dissected Osborne’s ligament was passed through this opening and repaired beneath the ulnar nerve using 2-0 PDS suture (Ethicon, Inc., Johnson & Johnson, Somerville, NJ, USA). Since Osborne’s ligament is taut in elbow flexion, the repair was carried out in full elbow flexion to prevent elbow stiffness. Except for repairing Osborne’s ligament, the size of the incision and extent of decompression were identical for CSD and MSD. A drain was inserted, and the incision was closed by subcuticular suture. The drain was removed after 24 hours. A long arm splint was applied with the elbow flexed at 90° and maintained for 24 hours. Thereafter, elbow range of motion was not restricted.
Ulnar nerve length before and after repairing the Osborne’s ligament
In patients treated by MSD, the ulnar nerve length was measured at operation. A white multifilament suture material (3-0 silk) was used to measure the length from the proximal medial intermuscular septum to the first motor branch of the ulnar nerve entering the flexor carpi ulnaris (Tsujino et al., 1996). Using a mosquito forceps, one side of the thread was temporarily attached to the most proximal part of the released intermuscular septum, where the ulnar nerve passed into the septum. Taking advantage of the surface tension of the moisturized ulnar nerve, the silk thread was stretched along the nerve. The location of the first motor branch entering the flexor carpi ulnaris was marked on the silk thread using a medical marker. Measurements were obtained with the elbow in full flexion and extension before and after repairing the Osborne’s ligament. Each task was repeated twice by the two orthopaedic surgeons, and the mean of the measurements reported by each surgeon was retained.
Ultrasonographic grade of ulnar nerve instability
Ultrasonographic assessment was done by a radiology specialist who was not informed of the operative technique, preoperatively and at 12 months after operation (Cho et al., 2018; Okamoto et al., 2000). The ulnar nerve was examined in transverse view in elbow full extension, mid-flexion (about 90°) and full flexion. Based on its position, the nerve was classified as not-dislocated (N; located within the retrocondylar groove, not passing the tip of the epicondyle), subluxed (S; located at the tip of the epicondyle) or dislocated (D; located anteriorly, beyond the tip of the epicondyle) (Figure 2) (Okamoto et al., 2000). The ulnar nerve instability was then classified as follows: Grade 0 instability (unchanged nerve position across the entire range of motion of the elbow; N–N, S–S, D–D); Grade 1 instability (the nerve position changed from the original position to its adjacent position; N–S or S–D); and Grade 2 instability (the nerve position changed from not-dislocated position to dislocated position; N–S–D). The change in position of the nerve was assessed five times, and the maximum value was retained.
Representative images illustrating nerve position. (a) The probe was applied transversely to the cubital tunnel, and a diagram of the transverse view on sonography. (b) Appearance of the ulnar nerve in the not-dislocated position in elbow extension and mid-flexion and the dislocated position in elbow full flexion, indicating Grade 2 instability. (c) Appearance of the ulnar nerve in a dislocated position in elbow extension, mid-flexion and full flexion (white arrow), indicating Grade 0 instability.
Assessing clinical outcomes
A trained nurse blinded to the study allocation performed the following measurements of physical function preoperatively and at 24 months postoperatively: grip strength, key pinch strength, pain on the visual analogue scale (VAS) score range 0–10) and recorded the score of the Quick Disabilities of the Arm, Shoulder, and Hand (QuickDASH) self-reported questionnaire. The two surgeons did preoperative and 24-month postoperative assessments of the McGowan grade, in which patients with subjective symptoms but without objective findings were classified as Grade I. Patients with good intrinsic strength (Medical Research Council (MRC) Grade 4) without detectable intrinsic atrophy were classed as Grade IIA; patients with fair intrinsic strength (MRC Grade 3) with intrinsic atrophy, as Grade IIB; and patients with profound motor weakness (MRC Grade 3 or less) with marked intrinsic atrophy and sensory disturbance, as Grade III (Goldberg et al., 1989). At 24 months postoperatively, assessment was done by the Wilson and Krout (1973) criteria: ‘excellent’ refers to minimal motor and sensory changes and no tenderness at the incision site; ‘good’ refers to occasional ache and mild sensory or motor changes; ‘fair’ refers to improved but persistent sensory or motor changes; and ‘poor’ refers to no improvement or a worsened condition.
Statistical analysis
All statistical analyses were carried out using SPSS version 19.0 (IBM Co., Armonk, NY, USA). The Shapiro–Wilk test for normality test was used. According to the result of the normality test, the paired t-test was used for paired parametric continuous variables and the Wilcoxon signed-rank test was used for paired non-parametric continuous variables. Student’s t-test was used for independent parametric continuous variables and the Mann–Whitney U-test was used for independent non-parametric continuous variables. The chi-squared test and Fisher’s exact test were used to compare discrete variables. The linear-by-linear association test was used to compare ulnar nerve instability between the groups, and simple linear regression analysis was used to find the relationship between chronological order and the assessment according to the Wilson and Krout criteria. The results for continuous variables are presented either as mean values with standard deviation (SD) or as median values with 25th–75th percentiles (IQR) and ranges. Statistical significance was set at p < 0.05.
Results
Demographics
Demographic data.
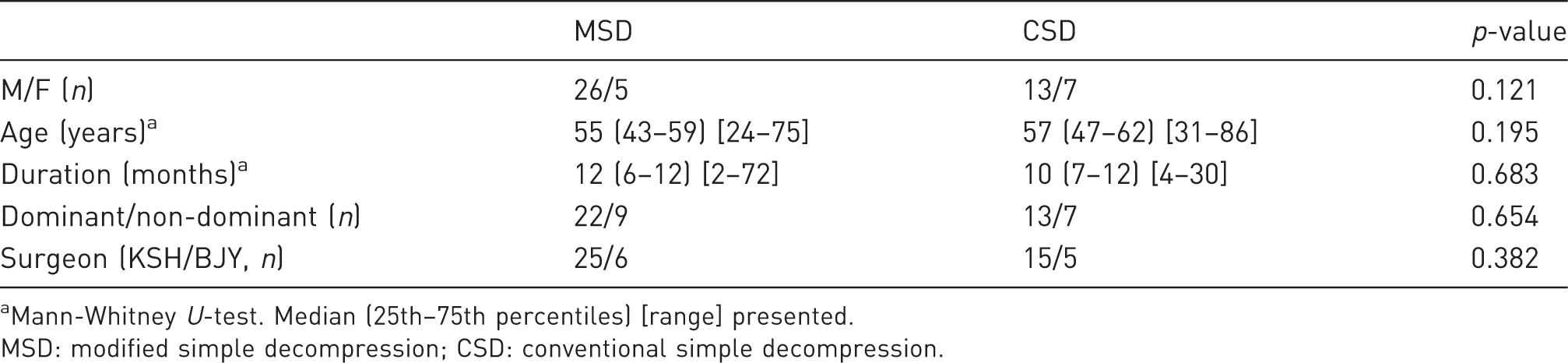
Mann-Whitney U-test. Median (25th–75th percentiles) [range] presented.
MSD: modified simple decompression; CSD: conventional simple decompression.
Ulnar nerve length before and after repairing Osborne’s ligament
Results of the ulnar nerve length after each procedure.

Wilcoxon-signed rank test. Median (25th–75th percentiles) [range] presented.
Significant values shown in bold.
Ultrasonographic grade of ulnar nerve instability at 12 months after operation
Ulnar nerve instability tendency after each technique.
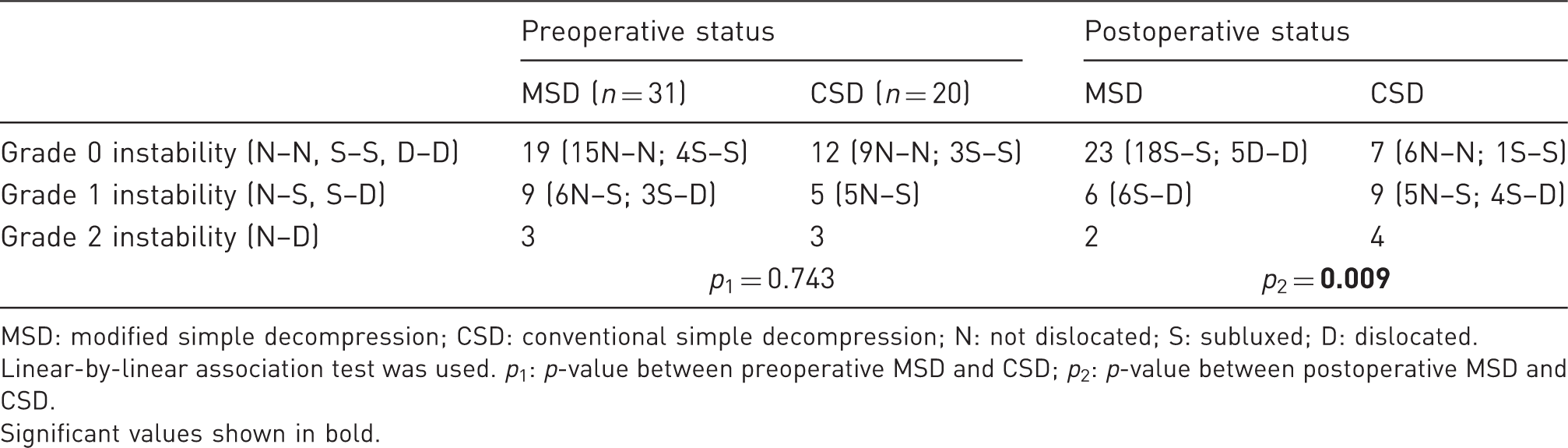
MSD: modified simple decompression; CSD: conventional simple decompression; N: not dislocated; S: subluxed; D: dislocated.
Linear-by-linear association test was used. p1: p-value between preoperative MSD and CSD; p2: p-value between postoperative MSD and CSD.
Significant values shown in bold.
Clinical outcomes measured preoperatively and at 24 months after operation
Pain score, QuickDASH score, grip and key pinch strengths.
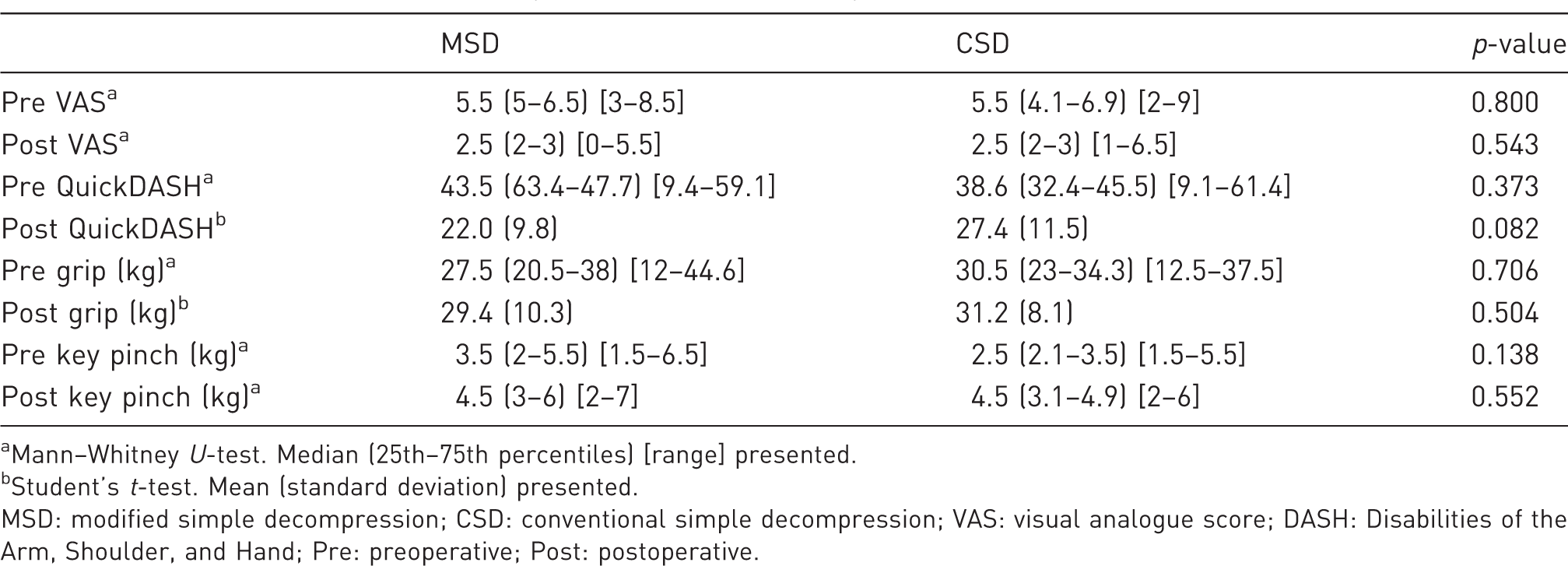
Mann–Whitney U-test. Median (25th–75th percentiles) [range] presented.
Student’s t-test. Mean (standard deviation) presented.
MSD: modified simple decompression; CSD: conventional simple decompression; VAS: visual analogue score; DASH: Disabilities of the Arm, Shoulder, and Hand; Pre: preoperative; Post: postoperative.
Discussion
We found that the ulnar nerve excursion in elbow flexion decreases significantly after repair of Osborne’s ligament and that, compared with CSD, MSD provides a lower grade of ulnar nerve instability without negative effect on the clinical outcomes at 24 months.
The evidence from cadaveric studies indicates that, although medial epicondylectomy and anterior subcutaneous transposition consistently result in substantial strain reduction, there is little change in nerve strain following simple decompression (Hicks and Toby, 2002; Mitchell et al., 2015; Tsujino et al., 1996). A common limitation of cadaveric studies is the lack of information regarding idiopathic cubital tunnel syndrome status; specifically, it is often not known whether the donors had idiopathic cubital tunnel syndrome, and it is likely that most donors did not. Our study included only patients with idiopathic cubital tunnel syndrome, and found that the repair of the Osborne’s ligament after simple decompression reduced the length of the ulnar nerve by approximately 5.6% in elbow flexion. However, we did not measure the ulnar nerve length before simple decompression and we cannot compare the change in the ulnar nerve length noted in the present study with that reported by previous cadaveric studies.
Overall, excellent or good clinical outcomes were observed in 88% of patients at 24 months postoperatively, which is higher than the rate reported in previous studies (Adelaar et al., 1984; Bartels et al., 2005; Biggs and Curtis, 2006; Bimmler and Meyer, 1996). However, because MSD involves an additional procedure, complications, including nerve adhesion around the repaired ligament, nerve kinking and perineural fibrosis, may occur. Moreover, after MSD, the ulnar nerve is often located directly over the medial epicondyle (S position). Because this position is superficial, the ulnar nerve is more vulnerable to external pressure, which could eventually lead to ulnar neuropathy (Abdel-Salam et al., 1991; Dekelver et al., 2012). Previous studies reported that, in such cases, revision surgery is typically required after 2–22 months (Krogue et al., 2015; Rogers et al., 1991), although recurrences have been noted even at 4–6 years after the original surgery (Bacle et al., 2014). Thus, 24 months is still a short period to confirm the clinical outcomes and complication rate after surgery for idiopathic cubital tunnel syndrome, and the long-term clinical outcomes and the incidence of recurrence remain uncertain.
Certain advantages of MSD should be considered. MSD can stabilize the ulnar nerve and reduce the ulnar nerve length without requiring a bony procedure, wide perineural devascularization or creation of a fascial sling, thus reducing the risk of complications, such as elbow instability, medial joint pain, segmental nerve ischaemia and secondary compression. MSD can be used when a small ganglion cyst is found in the retrocondylar groove during the operation, although no such patient was included in our study. Repairing Osborne’s ligament below the ulnar nerve provides a smooth and safe cushion for the ulnar nerve, and recurrence owing to regeneration of the ligament above the ulnar nerve does not occur.
Our study had several limitations. The patients were not randomized and instead were allocated to each group according to the date of surgery; therefore, potential bias related to patient selection or surgical proficiency cannot be excluded. It was not possible to carry out a prospective, randomized study because, since March 2014, the two surgeons in this study only performed MSD for idiopathic cubital tunnel syndrome. Six male patients were not followed-up for 24 months. We did not consider these missing data because the results are hard to predict using other factors. Although this deficit did not seem to be skewed in one group, the result might be affected. Only one radiologist assessed ulnar nerve stability, and the inter- and intra-observer reliability of such measurements could not be determined. The measurement of nerve length measurement was not blinded because it was done intraoperatively, which could have introduced detection bias. Moreover, the reliability and validity of the ulnar nerve length measurement technique using a silk thread and surgical marker were not verified. Because of the thickness of the surgical marker, it was difficult to determine exact points, which could lead to an error of up to 1–2 mm. Considering that the difference in the ulnar nerve length is 0.67 cm, this possible error would contribute to 15%–30% of the total difference. The length of the ulnar nerve was measured from the proximal medial intermuscular septum to the first motor branch, and this might not accurately represent the actual nerve length. The results were obtained in a small sample and thus may have limited statistical power.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by the ethics committee of Pusan National University Yangsan Hospital, 05-2016-048.