
Abstract
Metacarpal neck fractures with severe displacement are commonly treated surgically with intramedullary Kirschner wires. We present the results of treatment of fifth metacarpal neck fractures using a light curable intramedullary photodynamic polymer (IlluminOss™, IlluminOss Medical Inc., East Providence, RI, USA). Twenty-nine patients with isolated displaced fifth metacarpal neck fractures were included and followed up for 12–24 weeks. All fractures had radiologically healed after 3 months. In two cases, a secondary loss of reduction was seen, which did not require further correction. During the follow-up period, range of motion of the metacarpophalangeal joint was 89% after 6 weeks and increased to 100% after 3 months compared with the uninjured side. Grip strength improved over time from 61% to 85%. No implant removal was necessary. We conclude that osteosynthesis using an intramedullary photodynamic polymer is a reliable treatment option for displaced fractures of the fifth metacarpal neck.
Keywords
Introduction
Metacarpal neck fractures account for 10% to 20% of all fractures in the hand (Hove, 1993). The fifth metacarpal in particular is prone to impact injuries, such as a fall on the closed fist or punching. Owing to compressive forces and the pull of intrinsic muscles, the metacarpal head takes up a flexed position leading to shortening of the metacarpal bone and possibly malrotation. Most fractures of the neck of the fifth metacarpal are treated conservatively by buddy taping and early active motion (Beredjiklian, 2009). While rotational deformity and severe palmar displacement or shortening are widely accepted indications for surgical treatment, the amount of acceptable angulation deformity is still unclear and subject to discussion (Beredjiklian, 2009; Strub et al., 2010; Westbrook et al., 2008). Cadaveric studies however suggest that fracture angulations greater than 30° result in dysfunction of small finger motion at the metacarpophalangeal (MCP) joint (Ali et al., 1999; Birndorf et al., 1997).
Because of unfavourable results from plate osteosynthesis in the treatment of phalangeal or metacarpal fractures in close proximity to the MCP joint, the use of an intramedullary technique is preferred in the surgical treatment of metacarpal neck fractures (Facca et al., 2010; Page and Stern, 1998). Since its first description by Foucher et al. (1976), variations of antegrade intramedullary osteosynthesis with Kirschner (K)-wires have become a commonly used method of fracture fixation. The advantages of this procedure are thought to be the preservation of the already compromised soft tissue surrounding the fracture site, reducing the risk of soft tissue adhesions and concomitant loss of motion (Foucher, 1995; Yammine and Harvey, 2013). The reported complications of K-wire osteosynthesis vary widely (Yammine and Harvey, 2013). Possible risks are secondary complications, such as perforation of wires through the skin, intraarticular migration of wires into the MCP joint, extensor carpi ulnaris tendon wear or pin track infection in the case of percutaneous placement (Facca et al., 2010; Foucher, 1995; Ridley et al., 2017; Schädel-Höpfner et al., 2006; Strub et al., 2010). Implants may have to be removed, which adds to the patient’s discomfort and results in additional costs (Koç et al., 2012).
Light curable resins have been used in dentistry since the early 1970s (Rueggeberg, 2011). Since 2009, an implant system consisting of a light curable resin, enabling the formation of custom intramedullary implants, has been available for use in orthopaedic surgery (IlluminOss™, IlluminOss Medical, Inc., East Providence, RI, USA). With this system, a monomer delivered in a thin walled polyethylene terephthalate (PET)-balloon catheter is advanced in the medulla and is then polymerized in situ by application of light at a certain wavelength (Zani et al., 2015). Its use in different anatomical locations in orthopaedic surgery has been described (Gausepohl et al., 2017). In the treatment of metacarpal neck fractures, as with antegrade K-wire osteosynthesis, the intramedullary application of the implant avoids further soft tissue impairment. Recent biomechanical data suggests that intramedullary osteosynthesis of metacarpal neck fractures using this implant is significantly stronger in monocyclic loading than K-wire osteosynthesis (Gick et al., 2019). In contrast to most other forms of osteosynthesis, implant removal is not necessary.
This study reviews our results in the treatment of fifth metacarpal neck fractures with an intramedullary photodynamic polymer (IPP).
Methods
Surgical technique
The surgical approach is the same as that of antegrade fracture fixation with K-wires. Under regional anaesthesia and the use of a tourniquet, a short incision is made proximal to the entry point at the dorsoulnar base of the fifth metacarpal. Careful dissection preserves the dorsal branch of the ulnar nerve. The cortex of the bone is opened and a blunt flexible K-wire is introduced into the medullary canal. After reduction of the fracture, it is advanced to just below the subchondral cortex of the metacarpal head. Using a flexible reamer, the medullary canal is opened and, if feasible, gradually widened in 1 mm steps.
The implant consisting of the PET-balloon and the central light pipe is then introduced into the medullary canal and advanced as far as possible into the metacarpal head. After confirming the correct position of the implant, the balloon is inflated by injecting the resin. Final corrections of the reduction are now possible. The application of visible light activates a catalyst within the monomer, starting the curing process for a predefined amount of time (Figure 1). Upon polymerization of the resin, the light cable is removed and the excess length of the implant cut at bone level. After skin closure and sterile dressings, a splint is applied with the MCP in 90° flexion.
(a) Polyethylene terephthalate balloon filled with monomer ex situ. (b) After implantation the resin is cured in situ by application of visible light.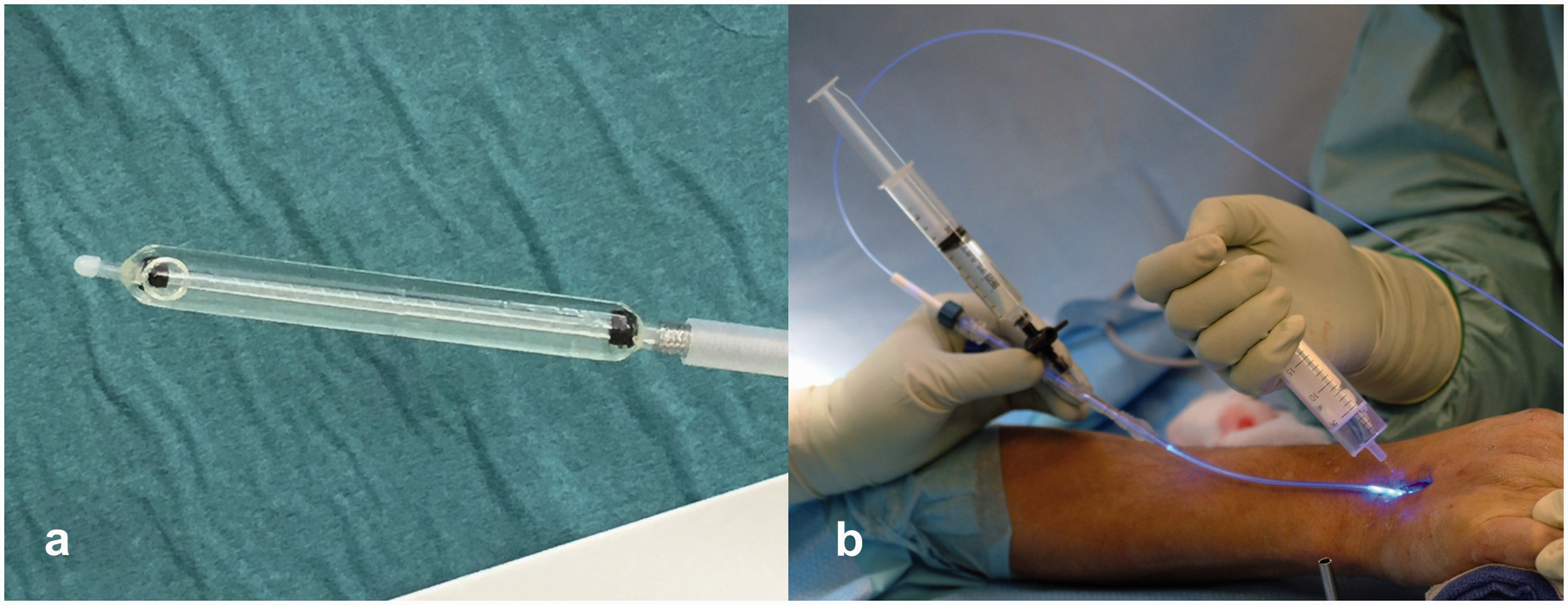
Early active motion is started the day after surgery out of the splint, which is worn only for a few days for analgesia, and then replaced by a metacarpal brace allowing free movement of the wrist and the MCP joint. After 6 weeks, build-up of strength is encouraged.
Patients
This was a single-centre observational cohort study from an academic hand surgical department, with a retrospective chart review of patients with isolated fifth metacarpal neck fractures, treated by closed reduction and fracture fixation with IPP, from December 2015 to April 2018.
Patients with metacarpal neck fractures, as described by Sletten et al. (2014), with angular deformity ≥30°, lateral displacement or malrotation and a clinical and radiological follow up of 12 to 24 weeks were included in the study. Patients younger than 18 years were excluded. Other exclusion criteria were the absence or refusal of informed consent, the use of osteosynthetic material other than IPP, patients with concomitant injuries to the same hand, patients with multiple injuries and patients with acute injuries to the contralateral hand.
Bony consolidation after 12 weeks was chosen as the primary outcome. Secondary outcome measures were radiological loss of reduction (angulation, shortening), range of motion of the MCP joint and total arc of motion (TAM) of the fifth finger compared with the contralateral side, grip strength compared with the contralateral side, duration of sick leave and any complications. Grip strength was measured with a Jamar dynamometer set.
For statistical purposes, continuous variables are described by median (with total range). Categorical variables are described by frequency and percentage.
Demographics and study data were retrieved from the electronic hospital medical record database. Radiological data were analysed using the picture archiving and communication system. Missing, conflicting and ambiguous chart elements were coded as missing data. The abstractors were not blinded to the study question.
For radiological examination, posteroanterior and 45° pronated oblique views of the injured hand were taken at each visit; these are standard views in our clinic and well established practice (Braakman, 1998). During follow-up, radiographs were analysed for signs of fracture healing and loss of reduction (Figure 2).
Fifth metacarpal neck fracture in posteroanterior and 45° oblique radiographs (a) preoperatively and (b) after fracture reduction and osteosynthesis with an intramedullary photodynamic polymer. (c) Radiological follow-up 3 months after operation.
Fracture angulation was determined by measuring the angle of intersection of a mid-medullary line drawn along the metacarpal shaft and a second line drawn from the mid-medullary point at the level of the fracture to the most distal point of the metacarpal head on oblique radiographs (Sletten et al., 2013). Shortening of the fifth metacarpal was measured on posteroanterior radiographs of the injured hand. A line connecting the most distal points of the third and fourth metacarpals was drawn and extended towards the fifth metacarpal. The shortening was then defined as distance from the most distal point of the fractured metacarpal to that line (Sletten et al., 2013). The advantage of this method is that only unilateral radiographs are required.
The study was approved by the local ethics committee and conducted according to the STROBE statement (Elm et al., 2007).
Results
Patient characteristics. Continuous data are shown as median and total range.
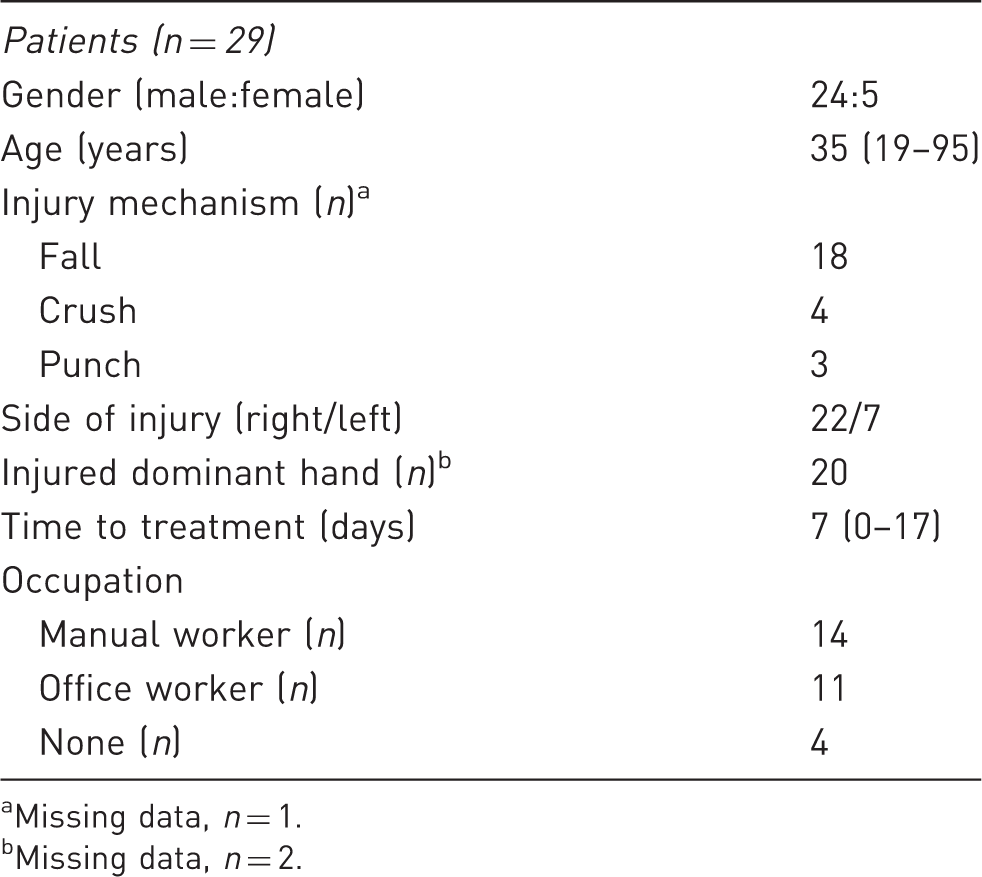
Missing data, n = 1.
Missing data, n = 2.
The mean duration of surgery was 54 minutes (range 27–120). Fixation was carried out with a polymer-filled balloon of the following sizes: 40 × 6 mm (n = 13), 40 × 5 mm (n = 11), 30 × 5 mm (n = 3), 30 × 6 mm (n = 1), missing data (n = 1). All operations were done by either a senior surgeon of the department or a registrar under the supervision of a senior surgeon.
Clinical and radiological follow-up examinations took place after a median of 6 weeks (range 4–9), 13 weeks (range 10–19) and 27 weeks (range 22–32). Ten patients did not attend the last follow-up examination at 27 weeks.
Median sick leave was 47 days (range 11–109; missing data n = 3). Median sick leave in manual workers was 49 days (range 13–109) and in office workers was 36 days (range 11–103). All patients returned to their previous work. Inability to work was not documented in patients without employment.
At the first radiological follow-up, callus formation could be observed in 28 out of 29 patients. At the second follow-up, all fractures had radiologically healed. No delayed union or non-union was seen.
The median shortening of the fractured fifth metacarpal was 5 mm (range 0–11). The median shortening at the first visit after surgery was 2 mm (range −1 to 10) and remained unchanged at the second (median 2 mm; range −2 to 10) and third visit (median 2 mm; range −1 to 7; missing data n = 10) (Figure 3(a)).
Box plots displaying (a) the shortening of the fifth metacarpal and (b) fracture angulation preoperatively and during radiological follow-up. The box indicates the interquartile range (IQR) from the first (Q1) to the third (Q3) quartile and the horizontal bar is the median. The whiskers show the range of values; ‘o’ mark the outliers, ‘x’ marks the mean. Outliers are defined as values larger than Q3 + 1.5 × IQR or smaller than Q1 – 1.5 × IQR.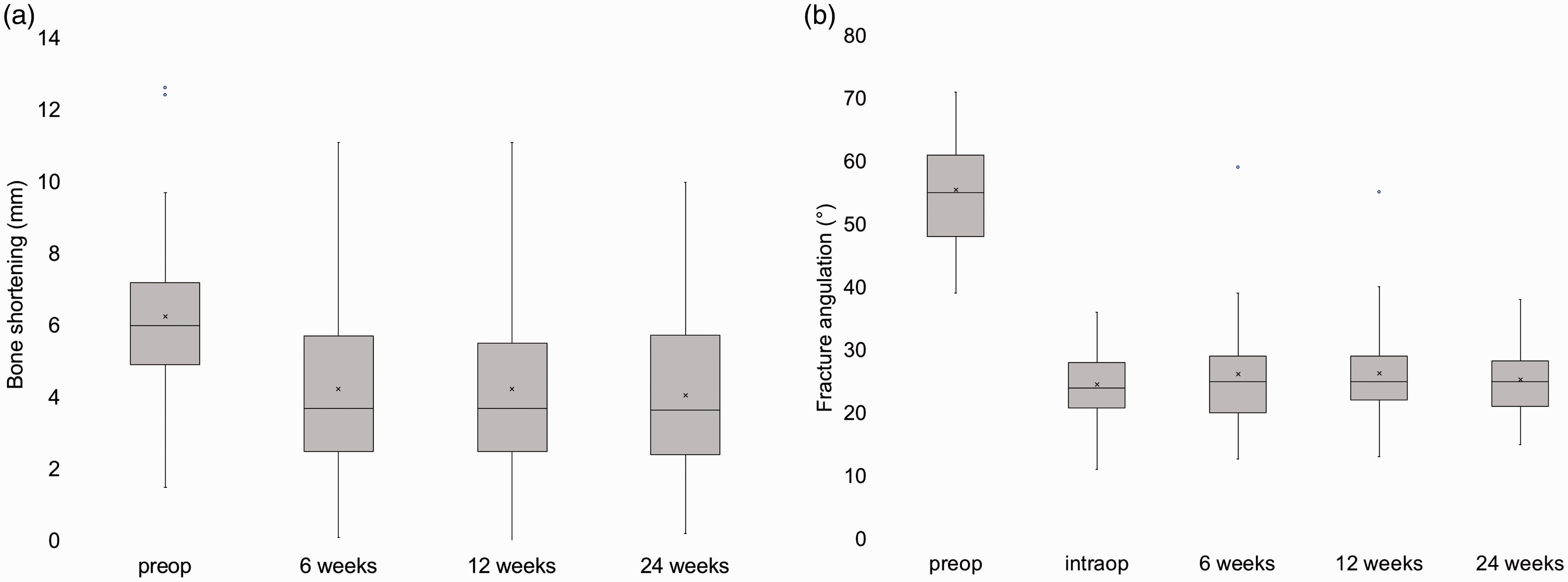
The median palmar angulation of the fracture was 55° (range 39–71) before surgery and was reduced to a median of 24° (range 11–36; missing data n = 9) intraoperatively. During follow-up, median angulation of the metacarpal head measured 25° (range 13–39) at 6 weeks, 25° (range 13–40) at 12 weeks and 24° (range 15–38) at 24 weeks (missing data n = 10) (Figure 3(b)).
In two patients, loss of reduction was seen at the first radiological examination: 5.0 mm shortening and 18° loss of angulation and 8.5 mm shortening and 28° loss of angulation, respectively. No further secondary displacement was observed during the postoperative course.
Outcome at clinical follow-up. Continuous data are given as median and total range. The values in square brackets are percentage values of the uninjured side.
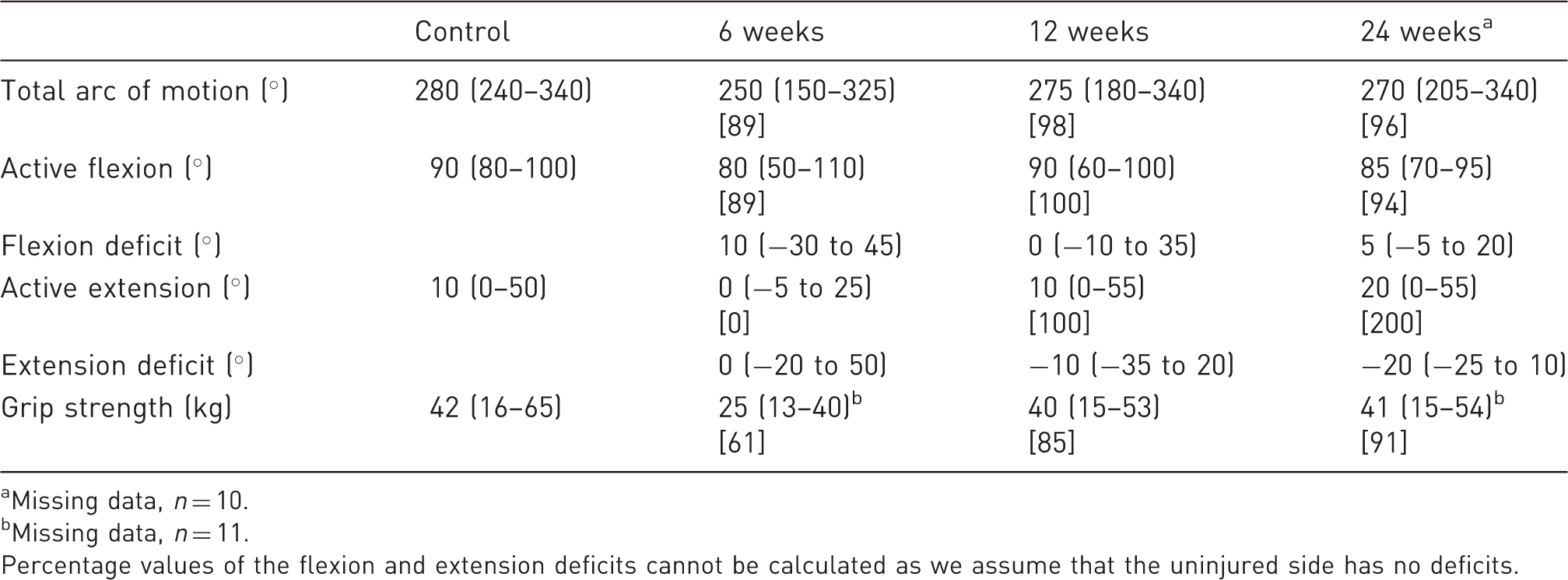
Missing data, n = 10.
Missing data, n = 11.
Percentage values of the flexion and extension deficits cannot be calculated as we assume that the uninjured side has no deficits.
Grip strength was compared with the uninjured hand at each visit. Grip strength improved over time from 61% to 85% to 91% compared with the uninjured side (Table 2).
At the first follow-up, seven patients mentioned mild pain during motion. At the second follow-up, eight patients reported pain under heavy strain and no pain at rest. None of the 19 remaining patients complained of pain at the last follow-up.
One intraoperative complication was encountered with incomplete curing of the resin within the balloon. The most common postoperative complication was transitory diminished sensation in the region of the dorsal branch of the ulnar nerve (n = 5), followed by skin adhesions (n = 4). These symptoms entirely disappeared in the follow-up period.
In one case there was a persistent supination deformity of 10° and in one patient an impingement in the carpometacarpal joint occurred because of excess length of the implant proximally. In one of the two patients with secondary loss of reduction, protrusion of the implant into the MCP joint was seen (Figure 4). Both patients underwent shortening of the excess implant in a further operation, with no further complaints. None of the patients developed complex regional pain syndrome.
Ultrasonographic view of the metacarpophalangeal joint of the little finger after secondary loss of reduction in a patient with a split head fracture. The implant protrudes into the joint. *: tip of the implant passing the joint line of the metacarpal head; **: metacarpal head; ***: base of proximal phalanx.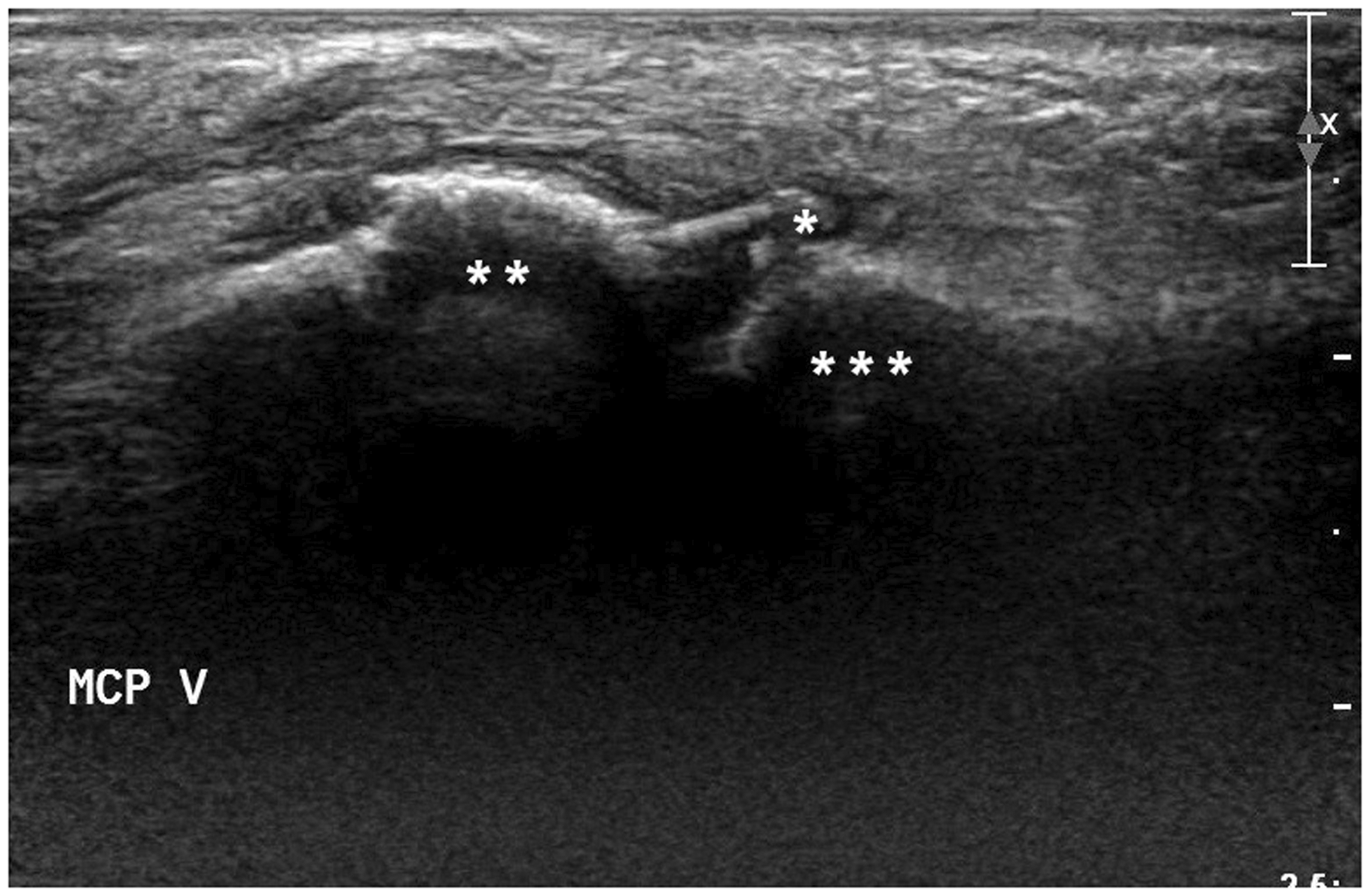
Discussion
We describe the osteosynthesis of fifth metacarpal neck fractures by closed reduction and fracture stabilization using an IPP. The applied IPP enables the formation of a custom implant by applying a photodynamic resin in a PET-balloon. After reduction of the fracture, the balloon is expanded by injecting the resin, and thereby fills the space created in the medullary canal. The light induced polymerization of the resin then renders the implant stable (Vegt et al., 2014).
All but one fracture showed clear signs of healing at the first follow-up after 6 weeks and all fractures had healed at the second follow-up (13 weeks). A near anatomical fracture reduction was achieved, from 55° angulation preoperatively to 24° intraoperatively (not subtracting the physiological tilt of the metacarpal head of 15° (Foucher, 1995)) and improving the shortening of the fifth metacarpal from 5 mm to 2 mm. This position remained unchanged during the follow-up period. The residual angulation of 9° is most likely to be attributed to our radiographic technique (Lamraski et al., 2005). In other studies, the postoperative metacarpal neck angle has been reported to be 9°–17° on true lateral radiographs (Sletten et al., 2014; Strub et al., 2010) and 8° on oblique radiographs (Winter et al., 2007). Facca et al. (2010) recorded the angulation at different time points during follow-up and reported a loss of reduction of 15° between oblique radiographs taken directly after operation and 12 weeks later. In the cited studies, it remains unclear whether or not the 15° physiological tilt was taken into account when reporting the values.
The ranges of movement that we report (Table 2) suggest that the use of IPP yields results comparable with those of patients treated with antegrade intramedullary K-wire (AIM) osteosynthesis. Facca et al. (2010) compared AIM osteosynthesis to plate osteosynthesis resulting in an MCP joint flexion of 98% compared with the contralateral side after 3 months in 20 patients in the K-wire group. Winter et al. (2007) compared AIM using K-wires with percutaneous transverse pinning and showed impressive results with a TAM of 274° and MCP joint flexion of 90° after 45 days and a TAM of 279° and MCP joint flexion of 94° after 90 days in 18 patients in the AIM group. Using AIM osteosynthesis, Strub et al. (2010) reported MCP joint flexion of 92° in 29 patients and Sletten et al. (2014) could show an MCP joint flexion of 95° and a TAM of 260° after 12 months in 42 patients. Sletten et al. (2014) also reported an extensor lag of 2° at the final follow-up. Wong et al. (2006) reported a TAM of 257° after 12 months in 30 patients (Wong et al., 2006).
Grip strength was also comparable with previous articles. Other studies have reported grip strengths of 92% and 93% after 3 months and 97% after 12 months (Facca et al., 2010; Winter et al., 2007; Wong et al., 2006) or around 50 kg after 1 year (Sletten et al., 2014; Strub et al., 2010).
The use of the IPP system is reasonably simple, but because of its design a few possible pitfalls must be mentioned. At the distal end of the implant, the tip of the light pipe is standing out of the balloon. In case of secondary loss of reduction or a split head fracture, this tip can protrude into the joint, from where it needs to be resected. This occurred in one patient who had a protrusion through an intra-articular fracture line. In doubtful cases, a preoperative CT scan may identify fractures extending into the joint. Furthermore, the implant is radiolucent except for two markers. This has to be taken into account when using IPP for fracture stabilization. In order to avoid placing the implant within the joint, in questionable cases an intraoperative ultrasound should be considered for visualization of the joint. We encountered two cases of secondary loss of reduction, which did not affect hand function and therefore were not corrected.
Also, it is important to slide the light pipe into the balloon completely and lock it in that position. Where there was incomplete curing of the resin, we assume that owing to incorrect assembly of the application system and subsequent partial slipping of the light pipe out of the balloon, the light did not reach the most distal part of the balloon and thus did not initiate the curing process.
There are several limitations to this study. Owing to its retrospective nature and the lack of a control group, the results have to be compared with other studies. Comparison with other studies is imprecise because of different follow-up periods or different presentation of results. The follow-up period is too short to identify any long-term sequelae. We did not encounter fractures of the implant, peri-implant fractures or implant-related infections. However, because of the anatomical properties of the medullary canal and the tight fit of the implant a retrograde implant removal is not feasible should such complications occur. An open resection of the implant through either the fracture itself or a longitudinal osteotomy might be necessary. We could not include all patients at the last examination, which is a known problem particularly in this patient group. This may have led to a deterioration in the clinical results at the last examination, assuming that patients with persistent complaints are more likely to attend follow-up examinations. Furthermore, the angular deformity of the fracture is exaggerated in the 45° oblique view (Lamraski et al., 2005; Sletten et al., 2013). Since we applied the same technique to all patients, we decided that this factor is negligible, but it has to be taken into account when comparing with other reports.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Cantonal Ethics Committee Bern (Project ID: 2017-00778).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.