
Abstract
We reviewed outcomes of 230 flexor tendon repairs in 27 thumbs and 203 fingers in Zone 1 and 2 over 7 years. In 2013, we used a 2-strand modified Kessler method followed by passive motion exercise in repairing flexor digitorum profundus tendon injuries in Zone 2 in 30 fingers; 24 fingers were followed, five (26%) had repair ruptures. Between 2014 and 2017, we used a 4- or 6-strand method to repair 111 flexor digitorum profundus tendons in Zone 2, followed by true early active motion. Two had repair ruptures. Among 101 fingers followed over 6 months, two fingers had tenolysis and 87 (87%) good or excellent outcomes. In 2018 to 2019, we used a 6-strand method to repair 42 flexor digitorum profundus tendons in Zone 2 with out-of-splint early active motion. None had repair ruptures or tenolysis. From 2014 to 2019, 27 flexor pollicis longus tendons were repaired in Zone 1 or 2, and 20 fingers had end-to-end flexor digitorum profundus repairs in Zone 1; none had repair ruptures or tenolysis. We conclude that a strong repair and true active motion are necessary for best outcomes of flexor tendon repairs in the thumb and fingers, and out-of-splint true active motion is safe.
Introduction
Analysis of digital flexor tendon repair over a lengthy period can be valuable to determine outcomes of different treatment protocols performed by the same surgeons. In this review, we summarize our patients with digital flexor tendon repairs from 2013 to 2019. In the 7 years, we have consistently audited outcomes associated with three treatment protocols.
This review includes a consecutive series of 181 patients with complete divisions of flexor digitorum profundus (FDP) or flexor pollicis longus (FPL) tendons in Zone 1 and 2 (200 fingers or thumbs in 159 patients) treated from 2014 to 2019, and of FDP tendons in Zone 2 (30 fingers of 22 patients) in 2013. The patients included are adults, being 15 years old or above. We excluded patients with (1) complete, or incomplete, amputation of fingers, (2) tendon injuries with concomitant phalangeal fractures or joint dislocations or skin or soft tissue defect in the involved finger(s), (3) accompanying extensor tendon injury, (4) segmental loss of the flexor tendon greater than 1 cm, or (5) wound contamination with a great risk of infection. Cases with concomitant digital nerve injuries in the finger or thumb were included, provided that the digital nerve could be repaired directly. Injuries with concomitant unilateral digital artery division were also included in the study, as long as the blood supply to the digit was good. We detail the three protocols and the outcomes from these three periods below.
Treatment protocols and outcomes: 2013
In 2013, we repaired Zone 2 flexor tendons in 30 fingers (22 patients). Six fingers (six patients) were lost to follow-up; 24 fingers (16 patients) were followed. Among those 24 fingers, the injuries included four index, seven middle, seven ring, and six little fingers with complete FDP division in Zone 2 as a result of lacerating (sharp) injuries. Six patients had flexor tendon repairs in two fingers, and one had tendon repairs in three fingers. All repairs were performed within 7 days after injury, except two cases, in which the time between injury and operation was 20 and 39 days. The surgical approach to the tendons was through a Bruner incision, and we retrieved the divided tendon ends from the palm through a separate incision in the palm if necessary.
These tendons were repaired with a 2-strand modified Kessler core suture with a 3-0 suture (Ethibond Polyster Suture, Ethicon, Somerville, NJ, USA) and a running circumferential suture with a 5-0 suture (Prolene Polypropylene Suture, Ethicon). Repair was followed by early mobilization in a dorsal splint using passive motion only (without rubber band traction) for 5 weeks. Active finger flexion was started after 4 to 5 weeks. We did not vent the A2 or A4 pulleys and did not use intraoperative extension–flexion testing after completing the tendon repair. We did not pay specific attention to the tensional status of the tendon repair site.
Among 24 fingers followed, five (26%) had repair rupture. We did not evaluate the functional recovery of these patients, and we considered a 26% rupture rate to be unacceptable. Consequently, we decided to alter our treatment protocols.
Protocols and outcomes from 2014 to 2017
Zone 2 repairs and outcomes
From January 2014 to the end of 2017, 111 fingers with Zone 2 FDP tendon repairs in 75 consecutive patients were treated. The mean age of patients was 36 years (16–63). The injuries included 28 index, 28 middle, 31 ring, and 24 little fingers with complete FDP division in Zone 2 as a result of lacerating (sharp) injuries. Eight patients had flexor tendon repairs in two fingers, eight had tendon injuries in three fingers, and four had tendon injuries in four fingers. Fifty-one fingers had associated digital nerve and/or artery injuries. All repairs were performed within 7 days after injury, except two cases, in which the time between injury and operation was 21 and 31 days.
Surgeons of expertise level II and III (Tang and Giddins, 2016), with assistance from other junior surgeons, performed the procedures, in all cases, under axillary brachial block with tourniquet control or under local anesthesia without tourniquet. Three years ago, one surgeon in the team was promoted to expertise level IV (Tang and Giddins, 2016).
In patients undergoing primary repair on the day of injury, the wounds were washed thoroughly before proceeding to tendon repair. The primary wound in the finger was extended by about 2 cm using a Bruner incision to expose the tendon sheath. In delayed primary repair, the incision was made to include the original laceration. The length of Bruner incision was usually less than 2 cm. The sheath was opened through a small midline incision of 1.5 to 2 cm in length. Flexion of the wrist and metacarpophalangeal joints was used initially to advance the retracted FDP tendon stump into the sheath opening. Where this technique was not successful, a separate incision at the distal palmar crease was made to find the proximal stump, which was then fed distally to the wound site using a catheter or by pushing with two forceps (Tang, 2015, 2018c). The proximal tendon stump was then advanced distally through the intact sheath to meet the distal end of the tendon. The proximal tendon stump was then immobilized with a 25-gauge hypodermic needle passed through the proximal sheath.
The FDP tendon was repaired with a 4-0 looped suture (Holycon, Jiangsu, China) using a 4-strand core suture (a U-shaped suture) (Cao and Tang, 2005). Core suture purchases were at least 7 mm, from the tendon ends. To increase gapping resistance, we always added slight tension to the core suture, with slight bunching of the repair, by producing a 10% tendon-segment shortening. After completing the repair, we regularly performed digital extension–flexion testing. If any gap occurred between the two tendon ends when the finger was fully extended, another core suture was inserted, converting the core repair to a 6-strand core suture of M-shaped configuration (Tang, 2007). Only sparse stitches of peripheral sutures were added as we detailed in an earlier report (Pan et al., 2019). We performed the digital extension–flexion test again after that. If needed, a few more peripheral sutures were added. With above techniques, 57 FDP tendons were repaired with the 4-strand U-shaped repair and 54 FDP tendons with the 6-strand M-Tang repair.
We did not repair the flexor digitorum superficialis (FDS) tendon in any of the fingers in order to allow greater space within the tendon sheath for FDP tendon gliding. The FDS tendon stumps were excised for about 2 cm from their attachment on the middle phalanx.
The synovial sheath was not repaired. When the tendon repair was located near the A4 pulley (14 fingers), the A4 pulley was vented entirely to make the repair easier and avoid restriction of tendon gliding (Tang, 2005, 2014). If the injury site was under, or in the vicinity of, the A2 pulley (40 fingers), 1/2 to 2/3 of the A2 pulley was vented (Lalonde and Martin, 2013; Tang, 2007). All of the venting was done in the volar midline and included excision of a small part of the adjacent sheath. The extension–flexion test was repeated to verify that the repair was strong enough to tolerate early rehabilitation and that a full range of free gliding of the repair was possible (Figure 1, supplementary video 1). We sometimes had to add a few separate peripheral stitches as detailed in our previous report by Pan and Chen (2019) to tighten the repair site if we found gapping at the repair site during the test (Figure 1). Finally, any divided digital nerves were repaired. The A1 or A2 pulley should be vented in the thumb FPL repairs, and a similar digital extension–flexion test was performed. The 6-strand repair may not need any peripheral suture if the repair was well tensioned and the test reveal no gapping (Figure 2).
A 32-year-old woman with a glass laceration of the FDP tendon in Zone 2 A underwent tendon repair 8 days later under wide-awake condition. (a) The entire A4 pulley and distal half of the A2 pulley were vented, and the A3 was retained. The proximal FDP stump was immobilized with a 25-gauge needle. (b) The FDP tendon was repaired with a 4-0 looped suture with a 6-strand M-Tang core suture without a peripheral suture. (c) and (d) When we performed extension–flexion testing, gapping occurred at the A3 pulley. Therefore, we added two figure-of-eight stitches on the lateral aspects of the tendon as shown in the photo. No gapping occurred when the repair glided under the A3 pulley when we performed the extension–flexion test again. (e) Finger flexion 2 months after surgery. (f) Finger extension 2 months after surgery. Videos of this patient are shown in online supplementary materials. A 32-year-old man with a complete Zone 1 FPL tendon laceration of the left thumb was treated within hours. (a) Venting the A2 pulley exposed the distal tendon stump. The proximal stump was pulled distally and was immobilized with a 25-gauge needle. (b) The FPL tendon was repaired using a 6-strand M-Tang core suture. (c) The thumb was passively flexed and confirmed smooth gliding of the repair site. (d) The interphalangeal joint of the thumb was hyper-extended without gapping of the repair. No peripheral sutures were used. (e) and (f) The active flexion and extension motion of the left thumb was normal 10 weeks after operation. The red arrow indicates the repaired thumb.

After surgery, the hand was protected in a short forearm-based dorsal splint, from 6–8 cm above the wrist to the tip of the fingers, with the wrist in 20°–30° of flexion, the metacarpophalangeal joints in 30°–50° of flexion and the interphalangeal joints fully extended. We have not used a splint distal to the wrist as described by Wong and Peck (2014).
The mobilization protocol used was a combined passive-active motion protocol (Giesen et al., 2009; Lalonde, 2019; Tang 2007, 2014, 2018b). Mobilization was started 4 days after surgery. The fingers rested in extension against the splint between exercise sessions, which were undertaken 5 to 6 times per day. A full range of passive digital motion (repetitions) was carried out 10 to 30 times before initiation of active digital flexion at each session. During the first and second weeks after surgery, active finger flexion was restricted to one-third of the total range of finger flexion from the fully extended position. The range of active flexion was increased to two-thirds in Week 3 and full flexion was achieved in Week 4. Each session included 20 to 30 repetitions of active motion. The splint was removed 6 weeks after surgery. Passive then active exercises were continued for about 10 to 12 weeks after surgery.
Among Zone 2 flexor tendon repair in 111 fingers, two fingers in two patients had ruptures. One patient ruptured his repaired FDP tendon in the index finger at Week 2 after surgical repair; another patient ruptured his repaired little finger FDP tendon at Week 4. Both patients did not follow the instruction of rehabilitation and started to actively use the fingers for work in the first 4 weeks. Both patients with repair ruptures had surgical re-repair of the FDP tendon using double U-shaped repair, an 8-strand repair consisting of two groups of U-shaped repair (Cao and Tang, 2006), a few days after the ruptures. The outcomes were rated good for both fingers.
Assessment of results of flexor tendon repairs (Tang, 2013).
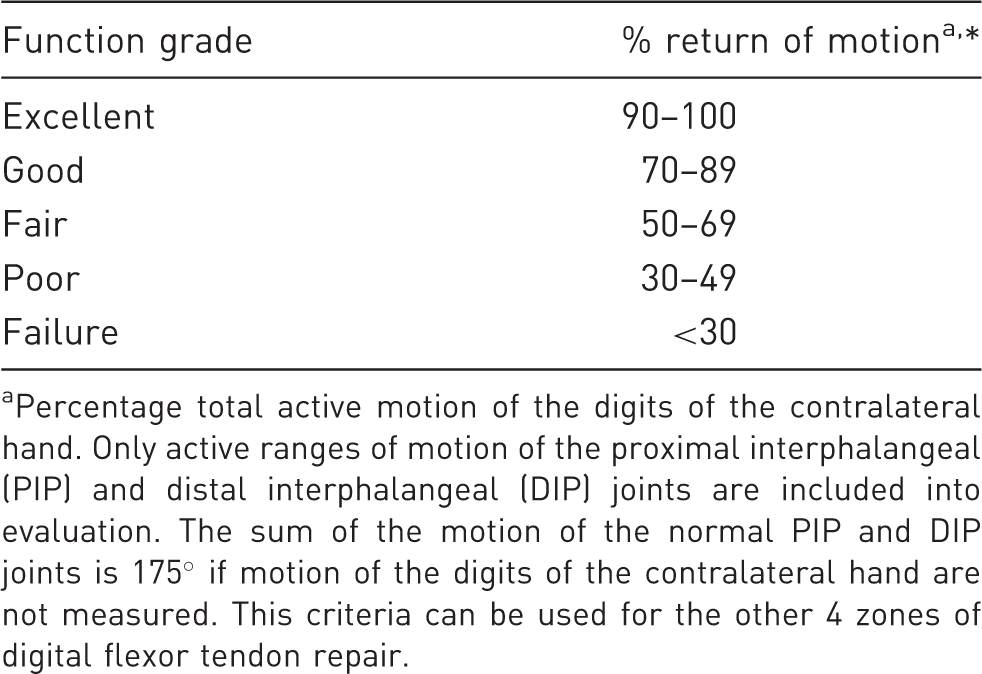
Percentage total active motion of the digits of the contralateral hand. Only active ranges of motion of the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints are included into evaluation. The sum of the motion of the normal PIP and DIP joints is 175° if motion of the digits of the contralateral hand are not measured. This criteria can be used for the other 4 zones of digital flexor tendon repair.
Outcomes of Zone 2 and Zone 1 FDP tendon repair in fingers.
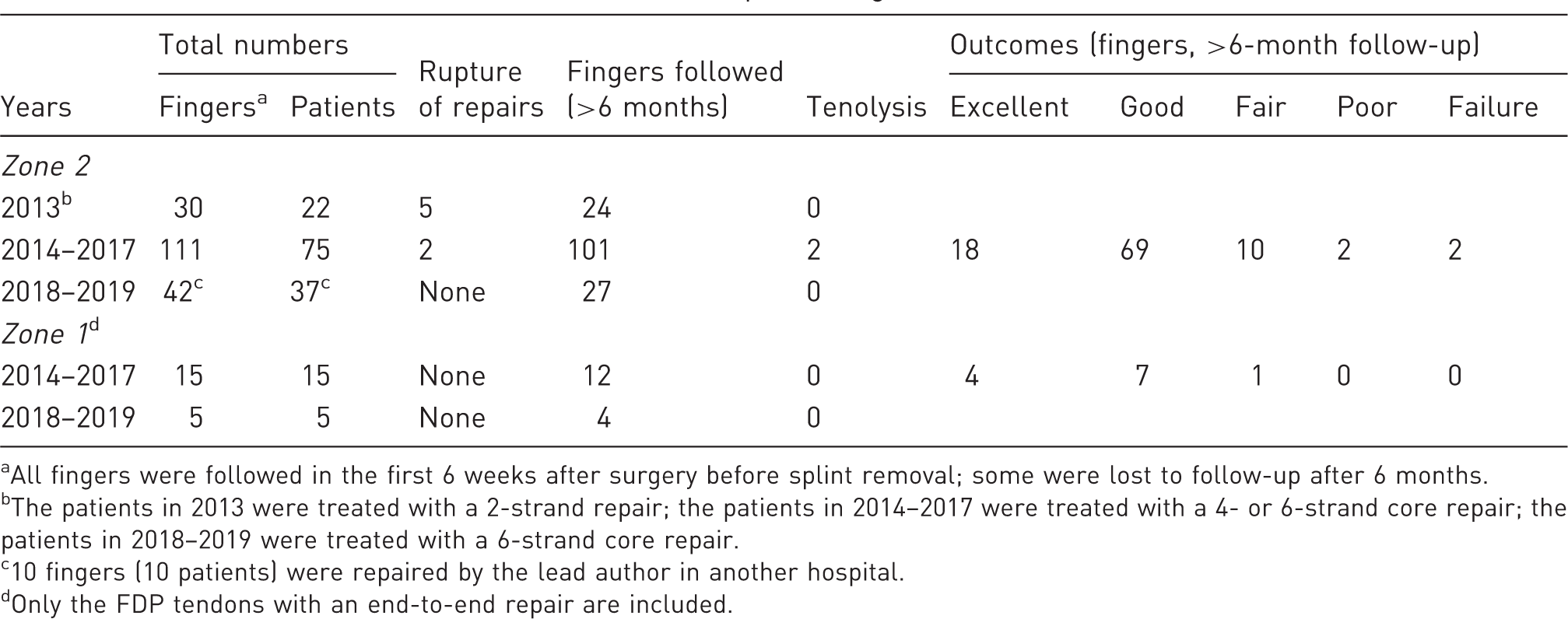
All fingers were followed in the first 6 weeks after surgery before splint removal; some were lost to follow-up after 6 months.
The patients in 2013 were treated with a 2-strand repair; the patients in 2014–2017 were treated with a 4- or 6-strand core repair; the patients in 2018–2019 were treated with a 6-strand core repair.
10 fingers (10 patients) were repaired by the lead author in another hospital.
Only the FDP tendons with an end-to-end repair are included.
Zone 1 repairs and outcomes
The repair of the Zone 1 flexor tendon was the same as in Zone 2. FDP tendons of the 15 fingers (15 patients) were repaired with 4-strand repair in 10 tendons, 6-strand repair in five tendons. For Zone 1 FDP repair, 12 out of 15 fingers with clinical follow-up over 6 months had good or excellent results (Table 2).
Zone 1 or 2 FPL repairs and outcomes
Outcomes of Zone 1 and 2 FPL repair in thumbs.

All thumbs were followed in the first 6 weeks before splint removal; some were lost to follow-up after 6 months.
Treated with a 6-strand core repair, except one thumb with a 4-strand repair in 2014–2017.
Protocols and outcomes from 2018 to 2019
The protocols from 2018 to 2019 used were the same as they were used from 2014 to 2017, with two changes: all FDP or FPL tendons were repaired with a 6-strand M-Tang repair, and almost all patients started out-of-splint motion after surgery (Tang 2018a, 2018b), except two patients who we deemed to be noncompliant.
There were no repair ruptures in this period, with 42 fingers (37 patients) and six thumbs (six patients) (Tables 2 and 3) in 37 patients. The final grading of the outcomes was still too early to report, as minimal of 6 months follow-up is necessary. No tenolysis has been necessary so far. We expect the functional recovery to be similar to that obtained from 2014 to 2017. Out-of-splint motion in 48 fingers or thumbs has been safe, with no repair ruptures.
Discussion
Remarkable changes in the surgical methods and postoperative motion regimes of flexor tendons in the hands have occurred in the past two decades (Caulfield et al., 2008; Giesen et al., 2009, 2018; Hoffmann et al., 2008; Lalonde et al., 2013, 2017, in press; Moriya et al., 2016, 2019; Orkar et al., 2012; Rigó et al., 2017; Reissner et al., 2018; Tang, 2007, 2014, 2018a, 2018b), which led to our use of updated protocols over the past 7 years. The protocol and outcomes used for the initial series patients between 2014 and 2016 were presented in our previous reports on outcomes of Zone 2 repair (Pan et al., 2019) and FPL tendon repair (Pan et al., 2017). The low incidence of tenolysis is consistent with that reported by Moriya et al. (2019).
Though this was not a comparative study, the results in three periods over 7 years shows differences in outcomes. One concern is that the surgeons’ expertise had definitely improved over the 7-year period, though we had new surgeons added to our team who had only entry level expertise as attending surgeons in this period. This can influence outcomes, but a rupture rate of 26% in 2013, compared with a rupture rate of 1.5% (from 2014 to 2019) in fingers is remarkably different.
The 1.5% rupture rate in two out of 153 fingers with Zone 2 repair from 2014 to 2019 and good and excellent results in 87% of the fingers from 2014 to 2017 are in sharp contrast to the rupture rate of five out of 30 Zone 2 repairs in 2013. Using an earlier protocol, which included 2-strand core repair and passive mobilization, no pulley venting, and no extension–flexion testing, rupture occurred in five out of the repairs in 24 fingers which had followup. These results show that a multi-strand core repair, adequate pulley venting, and intraoperative extension–flexion testing for gapping and free gliding of the repair, in association with early active motion significantly improves outcomes over a conventional 2-strand repair with early passive motion for Zone 2 injuries. Because four changes occurred between the earlier and the updated protocol, we do not know whether any one of these changes is particularly important. However, it is clear with all four changes, the outcomes improved with almost no repair ruptures.
Two ruptures that we encountered were in two patients who did not follow instructions and started to use their hand normally soon after repair, and one started heavy labour at Week 4. In the patients who followed our instruction, even with some light use of the hand, we have not found rupture. We consider venting the major pulleys to be as important as a strong core repair in reducing the incidence of rupture. We consider venting the pulley and a tensioned repair the most important keys in making a repair.
An additional observation is that the knots of core sutures in the methods that we have used since 2014 are exposed on the tendon surface rather than being placed between two tendons ends. This had no adverse influence on the outcomes. We agree with the findings and considerations from recent biomechanical studies of Chang et al. (2018) that placement of suture knots between the tendon ends do not favour gap resistance and propose that knots should not be placed between the tendon ends (Chen et al., 2018). We currently use the 6-strand M-Tang method in all patients with few or no peripheral stitches. Whether to add a few sparse peripheral stitches is decided by observation on gapping and roughness of the repair site during the digital extension–flexion test. In the 6-strand M-Tang method, no suture knots are between two tendon ends, eliminating the need of peripheral sutures, or at least, standard peripheral stitches, if tension over core sutures is ensured.
Performing the digital extension–flexion test is extremely helpful. In our series, only a small percentage of the patients had wide-awake surgery. Therefore, only a small percentage of the patients had an active test. Passive digital extension–flexion test worked very well in the remaining patients. Other keys in our series include not repairing the FDS tendon and starting true active motion with or without splint protection at the time of motion as proposed recently (Tang, 2007, 2018a, 2018b). The factors that are not important include peripheral suture, frequency of motion exercises, and timing of tendon repair. We did not observe effects of these factors on the outcomes and deem these to be of low importance. We did not repair the FDS in our series, which may contribute to good outcomes by eliminating the risk of adhesions between the FDP and FDS tendons and decreases the resistance of tendon gliding after repair surgery. In the past three decades, many laboratory studies also support these considerations.
We found some patients, though not many, had fair or poor results. We consider the degree of injury and individual variation and health condition contribute to these unsatisfactory outcomes. Because patients with less than good recovery were few, we were unable to analyse whether there was definite correlation, but we noted these conditions might have contributed to the poor or fair outcomes. We also cannot rule out unsatisfactory surgeries in these patients, because surgeons’ factors could not be entirely controlled over a lengthy period. We consider patients’ non-compliance to be a key cause of repair rupture. Patients should be warned to avoid heavy labour in the first 8–10 weeks after repair. Strong surgical repairs can allow for early active motion and may afford some light manual activity, but are not suited for early return of heavy or even routine activities.
Footnotes
Acknowledgements
The clinical protocols used in the patients from 2014 to 2019 are provided by Department of Hand Surgery, Affiliated Hospital of Nantong University, Jiangsu, China.
Dr Jing Chen, Nantong University, independently reviewed and evaluated outcomes of the patients treated from 2014 to 2017 through clinical pictures of the patients with 6-month or longer clinical observation.
Drs Lei Pan and Yun Fei Xu in our team participated in the surgeries in this study.
Jiangsu Clinical Medical Research Center provided the sutures used in this report.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.