
Abstract

Dear Editor,
An 8-month-old baby boy presented to our department with bilateral congenital hand differences. On the right, he had a five-fingered hand with three phalanges in the most radial digit (Figure 1(a) and (b)). On the left, the most radial digit was duplicated although there were also three phalanges in the ulnar duplicate. Both first web spaces were narrowed and the thenar muscles were hypoplastic (Figure 1(c) and (d)).
(a) and (b) Preoperative picture and corresponding radiograph of the right hand showing a five-fingered hand. (c) and (d) Preoperative picture and corresponding radiograph of the left hand showing a five-fingered hand with duplicate thumb.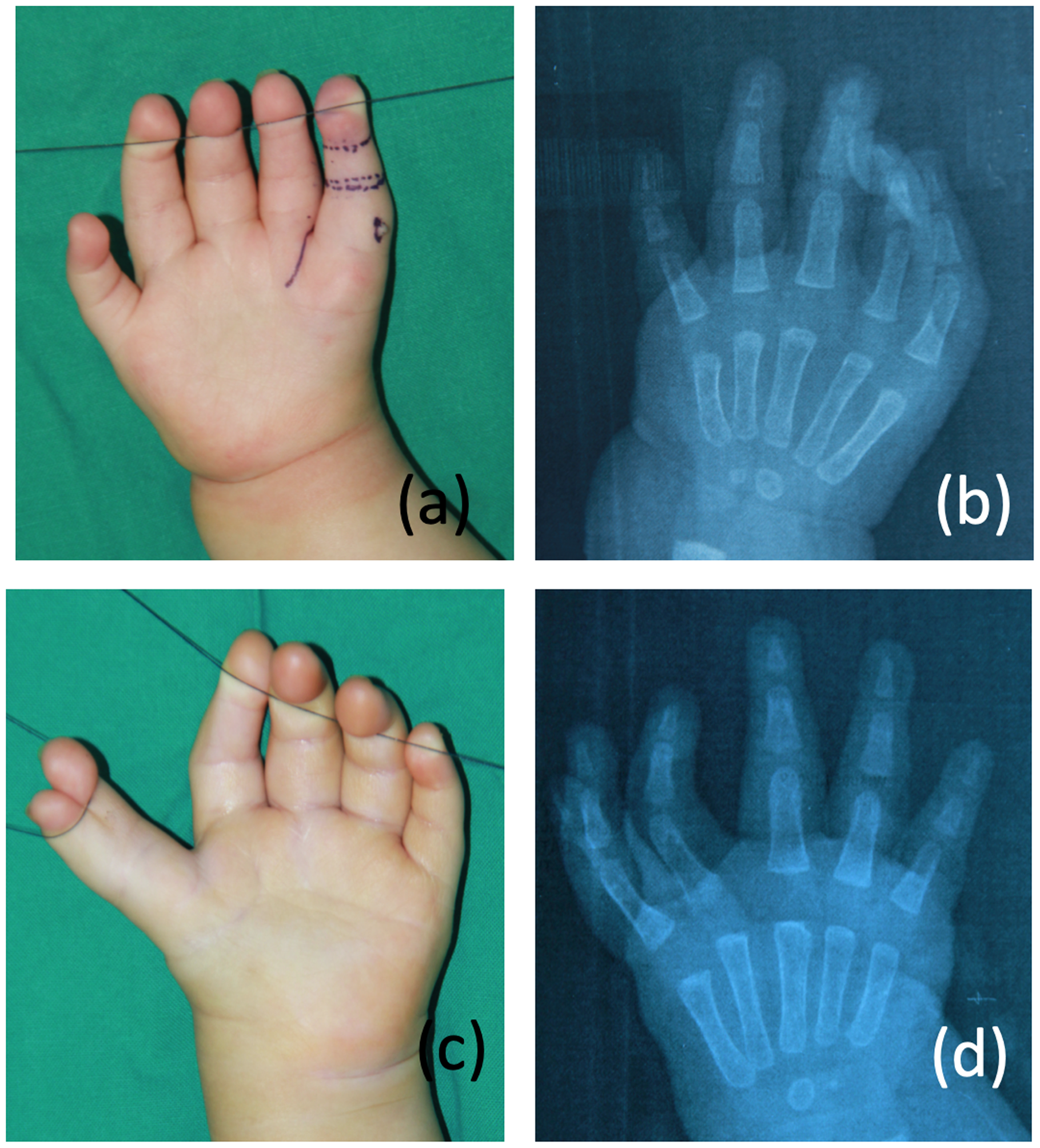
The surgical plan consisted of correcting the duplicate thumb on the left and removing the triphalangeal thumb element bilaterally. At the same time, tightness in both first web spaces were addressed. On the right thumb, a longitudinal incision was made on the ulnar side of the middle phalanx and an intersegmental flap was harvested, based on the neurovascular bundle of the radial proper digital artery and corresponding nerve. The pedicled flap was then transferred through a subcutaneous tunnel to widen the first web space (Figure 2(a)–(c)). The ulnar neurovascular bundle was meticulously preserved as well as dorsal veins of the remnant thumb to ensure that there would be no vascular compromise to the distal phalanx. The middle phalanx was removed and a new interphalangeal (IP) joint created by transfixing the distal phalanx to the proximal phalanx. The extensor tendon was shortened with plication sutures and a longitudinal syringe needle inserted across the IP joint and kept in place for 4 weeks while the soft tissues healed. On the left hand, a similar procedure was performed; the middle phalanx was ablated, and an intersegmental flap harvested to reconstruct the first web space. The radial thumb duplicate was removed at the same time and the soft tissues used to widen the intersegmental flap that was inserted into the first web space (Figure 2(d)–(f)). Both flaps and distal thumb digits survived uneventfully, and at the last follow-up (16 months postoperatively) the child demonstrated a good first web space and a functional hand bilaterally. Range of active/passive flexion of the IP joint was 0 °–75 ° on his left thumb and 0 °–70 ° on the right thumb.
(a) and (b) Intersegmental skin flap from the middle phalanx of the right thumb harvested and inserted into the first web space pedicled on the radial digital artery (white arrow). (c) Results at 16 weeks postoperatively. (d) Intersegmental skin flap from the middle phalanx of the left thumb harvested and inserted into the first web space, again pedicled on the radial digital artery. (d) and (e) Two small triangles were designed from the skin of the excised radial duplicate to widen the flap (white arrow). (f) Results at 16 weeks postoperatively.
Triphalangism of the thumb is uncommon, as characterized by an extra middle phalanx that can be of various shapes and configurations (Hovius et al., 2019). The deformity can co-exist with thumb duplication; a complex arrangement that has been further described and classified by the Rotterdam classification (Zuidam et al., 2008). When the middle phalanx is rectangular, as in the case of our patient, the hand is typically known as a five-fingered hand. Hovius et al. (2019) favoured preservation of the original carpometacarpal (CMC) joint instead of a pollicization procedure as they found that this led to more strong and stable thumbs. Deficiency of the first web space, without pollicization, were treated with local flap procedures, such as Z-plasty and/or rotational flaps from the dorsum of the hand or the index finger. In this patient, we decided to use skin that would otherwise be discarded from the ablation of the middle phalanx. The height, as well as the circumferential diameter of the middle phalanx, allows a flap design that is wide enough to address the tightness of the first web and extend sufficiently from the dorsum to the volar aspect of the hand. Moreover, the use of tissues that would otherwise be discarded avoided the need for more scars from other local flap options. The important steps in the surgery are the meticulous dissections of the neurovascular bundles that would ensure reliable viability of the pedicled flap and preservation of blood supply to the distal phalanx of the remnant thumb.
Radiologically, the ratio of the length of the second metacarpal to that of the first metacarpal for this patient was calculated as 1.1 (right hand) and 1.2 (left hand). These were significantly lower than the normal values for a 2-year-old Asian child, which is usually in the region of 1.6 (Matsuura and Kajii, 1989), implying that the first metacarpals in our patient were longer. This phenomenon is common in triphalangeal thumbs and a standard treatment may therefore involve reduction (and rotational) osteotomy of the first metacarpal in addition to the removal of the extra middle phalanx (Hovius et al., 2019). If there are growth plates on both ends of the metacarpal, epiphysiodesis should be considered to prevent extra growth in the future. In our patient, we have decided to keep the first metacarpal intact because we believe that excision of the extra phalanx was sufficient to reduce length. Further observation would be required to decide whether reduction osteotomy, epiphysiodesis or an opposition plasty is necessary in the future.
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was funded in part by the National Natural Science Foundation of China [81472104].