
Abstract

Dear Editor,
Dorsal dimelia is a rare congenital hand difference, a result of a developmental error in the dorsoventral axis during digit formation. In this condition, there is evidence of nail structures on both the dorsal and palmar aspect of the digit. Reconstructive options available are limited. We present a case of dorsal dimelia in a thumb tip with the use of a free great toe wraparound flap.
A 14-year-old girl presented to our department with a congenital hypoplastic left thumb. The nail complex appeared to cover both the dorsal and volar aspect of the tip, forming a cap over the distal phalanx (Figure 1(a)–(b)). In particular, there was evidence of ectopic nail on the volar aspect of the thumb pulp and a diagnosis of dorsal dimelia was made. The range of motion of the metacarpophalangeal (MCP) and interphalangeal joints were extremely limited, and there was a tendency for her thumb to go into ulnar deviation at the MCP joint whenever flexion was attempted. Opposition was restricted only to a pinch prehension with the index finger, but not the rest of the digits. Radiographs revealed a hypoplastic distal phalanx with a conical appearance (Figure 1(c)). The patient was very keen for surgical correction of her left thumb, mainly for cosmetic improvement. A plan was made to reconstruct the distal thumb deformity with a great toe wraparound flap.
(a, b) The thumb manifests as a ‘chicken claw’ deformity. (c) X-ray shows the distal phalanx of the thumb was conical. (d, e) At 2 years postoperatively, the reconstructed thumb in different views. The reconstructed thumb can complete the action of thumb to fingers. (f) The great toe wounds healed well with good appearance.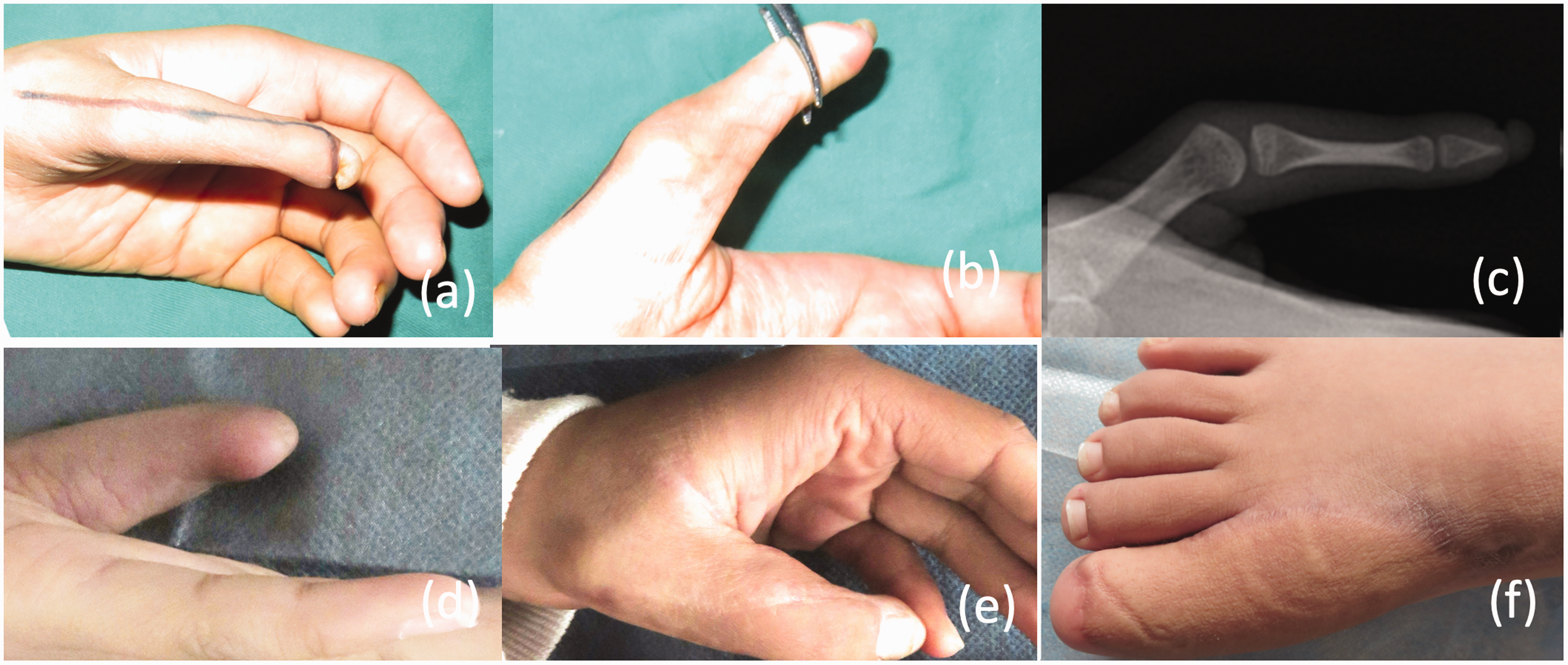
An incision was made on the dorsal ulnar aspect of the thumb (Figure 1(a)). Intraoperatively, the flexor pollicis longus (FPL) tendon was found to be hypoplastic and shifted to the dorsal and ulnar side and the radial collateral ligament was found to be extremely lax; this would explain why there was a tendency for the MCP joint to ulnarly deviate whenever she flexed her thumb. The FPL tendon was centralized and a strip of fascia lata graft was harvested to reconstruct the flexor pulley. The radial collateral ligament of the MCP joint was also reinforced with fascia lata graft. The nail complex was removed in its entirety with its germinal matrix, and a free great toe wraparound flap, as described by Morrison et al. (1980), was used to replace the defect. The first dorsal metatarsal artery of the toe flap was anastomosed to the dorsal radial artery in the anatomical snuff box, and the dorsal cutaneous nerve of the first toe was sutured to a branch of the superficial radial nerve.
A perforator flap based on the descending branch of the lateral circumflex femoral artery on the patient's contralateral thigh was simultaneously harvested to reconstruct the donor defect. Both the great toe wraparound flap and perforator flap for the donor site survived uneventfully (Figure 1(d)–(f)). At 2 years follow-up, both the thumb and the great toe have healed well. Sensation was adequate in the reconstructed thumb tip and the thumb MCP joint remained stable with an improved flexion range of 0°–30°. As a result, the reconstructed thumb could now oppose to the rest of the digits (Figure 1(e)).
Dorsal dimelia classically manifest with nail deformities, flexion abnormalities and a tapered or hypoplastic phalanx (Al-Qattan, 2013). These deformities remain extremely uncommon with an unknown aetiology. In 1977, Egawa reported the first dorsal dimelia (Egawa, 1977) and recent genetic and animal studies have linked dorsal dimelia to abnormal apical ectodermal ridge boundary formation (Habenicht et al., 2019). This would suggest that both the proximal distal axis as well as the dorsal ventral axis are involved in its pathogenesis. Intraoperatively, both the flexor and extensor tendons in our patient were abnormal, suggesting a more global developmental error. To improve the appearance of the thumb deformity, we performed a double free flap procedure, to reconstruct her thumb with a great toe wraparound flap and a perforator flap to reduce her donor site morbidity. Postoperatively, the patient was delighted with the appearance of her thumb and also the improved function as a result of improved MCP joint flexion. In conclusion, we present our experience with reconstruction in a patient with dorsal dimelia who went on to achieve satisfactory cosmetic and functional results.
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.