
Abstract
To compare the outcomes of non-operative versus operative treatment for distal radius fractures in patients aged from 18 to 64 years, we performed a retrospective analysis using the OptumLabs® Data Warehouse using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis codes of distal radius fracture. Of the 34,184 distal radius fractures analysed, 11,731 (34%) underwent operative management. Short-term complications within 90 days of fracture identified an overall complication rate of 16.6 per 1000 fractures and the 1-year upper extremity-specific complication rate was 287 per 1000 fractures. Overall, post-injury stiffness was the most common 1-year upper extremity-specific complication and was associated with operative management (202.8 vs. 123.4 per 1000 fractures, operative vs. non-operative, p < 0.01). Secondary procedures were significantly more common following non-operative management (8.7% vs. 43%, operative vs. non-operative, p < 0.01) with carpal tunnel release representing the most common secondary procedure. Operative management of distal radius fractures resulted in significantly fewer secondary procedures at the expense of increased overall 1-year complication rates, specifically stiffness.
Keywords
Introduction
Distal radius fractures (DRFs) are common, with a rising incidence in paediatric, adult and older adult age cohorts. Given this, their management costs continues to escalate (Nandyala et al., 2018; Nellans et al., 2012). One of the main driving factors is the cost of care associated with open reduction and internal fixation (Huetteman et al., 2018; Kazmers et al., 2018; Nandyala et al., 2018; Swart et al., 2017).
Fractures of the distal radius in young, active adults are often related to higher energy mechanisms in comparison with older adults (Gauci et al., 2016; Nellans et al., 2012).
Displaced DRFs are less well tolerated in young patients than in patients over 65 years of age, particularly in terms of palmar tilt, ulnar variance and loss of radial height (Beumer et al., 2013; Grewal and MacDermid, 2007; MacIntyre and Dewan, 2016; Perugia et al., 2014).
Given this, there is an increasing tendency for surgical intervention within this younger cohort to restore anatomy and try and improve clinical outcomes (Azad et al. 2019); however these effects appear to be mitigated with advancing age (Gliatis et al., 2000; Grewal and MacDermid, 2007; Hollevoet et al., 2003).
Consequently, the present study is designed to identify trends in the modality of management for DRFs with a focus on the relative utilization of non-operative treatment with closed reduction and plaster casting versus operative intervention with closed reduction and percutaneous pinning (CRPP) with Kirschner-wires, external fixation (EF) and open reduction internal fixation (ORIF) in patients ranging from 18 to 64 years using the OptumLabs® Data Warehouse (OLDW). This is akin to what we had previously reported on a separate cohort of patients aged 65 years and older (DeGeorge et al., 2020).
Less robust evidence exists to guide the management of DRFs in patients between 18 and 64 years of age, compared with that for the elderly patient population, with a general consensus that instability and residual deformity are better tolerated with advancing age (Azad et al., 2019; Kong et al., 2019; Perugia et al., 2014; Synn et al., 2009). The primary aim of this study was to assess the patient-specific demographic factors and co-morbidities associated with both operative and non-operative management of DRFs for the patients under 65 years of age. The secondary aim of the study was to investigate the rates of 90-day and 1-year medical complications, postoperative complications and the need for secondary operative procedures associated with each mode of management in the age cohort.
Methods
Data source
The OLDW includes claims data for over 100 million privately insured and Medicare Advantage enrolees throughout the United States (US). The OLDW is a proprietary, de-identified administrative claims database, containing medical and pharmacy claims, laboratory results and enrolment records for Medicare Advantage and commercial enrolees as well as longitudinal health data on patients, representing a varied mixture of demographic cohorts across the US (Wallace et al., 2014). The approach is similar to that previously described to assess the outcomes and complications following DRF in patients aged 65 years and older (DeGeorge et al., 2020). These data are compliant with the privacy rules of the Health Information Portability and Accountability Act and were therefore exempted from review by the institutional review board at our institution.
Study population
The database was queried for all DRF claims in patients aged 18 through 64 years of age from 1 January 2009 to 31 August 2014, including primary or secondary diagnosis codes, to control for the potential of pre-existing or historical conditions (Appendix S1). The DRF codes included DRFs with and without fractures of the distal ulna. Patients were required to have medical coverage for 1 year prior to and 1 year after injury to prevent the potential of inaccuracies due to patient loss (online supplementary figure). The presence of a treatment code with an associated inpatient or outpatient encounter was required. Fractures associated with ICD-9-CM codes for E810.0–E891.9 (motor vehicle collision) were specifically excluded. We classified treatments as non-operative or operative. If both treatments were included in the same encounter, the encounter was recorded as operative. Furthermore, if multiple encounters were separated by less than 90 days, we classified them as the same encounter/same fracture. Non-operative initial management was classified as the absence of a same side operative treatment within 90 days of the initial diagnosis of DRF. Additionally, patients treated with an operative procedure between 91 days and 1 year following initial classification as non-operative initial management were classified as having received secondary operative treatments. Operative fracture management was then subdivided as ORIF, CRPP or EF.
Independent variables
Demographic information, geographical distribution, occurrence of fracture, the Charlson/Deyo Index (CCI) and individual component comorbidities were recorded. The CCI index was calculated using primary and secondary diagnoses to identify 17 conditions during the 1-year prior to fracture (baseline period) (Charlson et al., 1987). CCI was utilized to assess the comorbidity weight at baseline and was stratified into three categories for data analysis (0, 1, 2+).
Outcomes
Ninety-day medical- and wound-related complications were assessed (Table 4 and Appendix S2). One-year upper-extremity-specific complications were also recorded (Table 4 and Appendix S2). One-year, same laterality secondary (revision/subsequent) procedures were defined by the presence of a same side current procedural terminology (CPT) code disparate from the primary encounter within 1 year of the fracture (Appendix S2). In order to ensure a ‘same side’ secondary procedure, only cases with a laterality modifier on the index procedure and subsequent procedure were included. Complications present prior to DRF were excluded as a pre-existent condition. Complications were analysed overall and secondarily divided by treatment type.
Statistical analysis
Patient characteristics were described using percentages, counts for categorical and ordinal data, means and standard error for continuous data. Continuous variables were assessed with the Kruskal–Wallis test and categorical data was assessed with the chi-square test. Ninety-day and 1-year complication rates were expressed as the number per 1000 fractures for overall analysis and by treatment modality. Multivariable logistic regression models were used to account for differences in patient characteristics. Models were run for overall 90-day and 1-year complications as well as individual complications with a covariate indicating surgery type (operative vs. non-operative) and adjusting patient characteristics. To comply with OptumLabs® policy, data with a cell size less than 11 observations were not disclosed to protect patient confidentiality. Values of p < 0.05 were considered statistically significant.
Results
Demographic factors and co-morbidities
Patient demographics classified by two management methods.
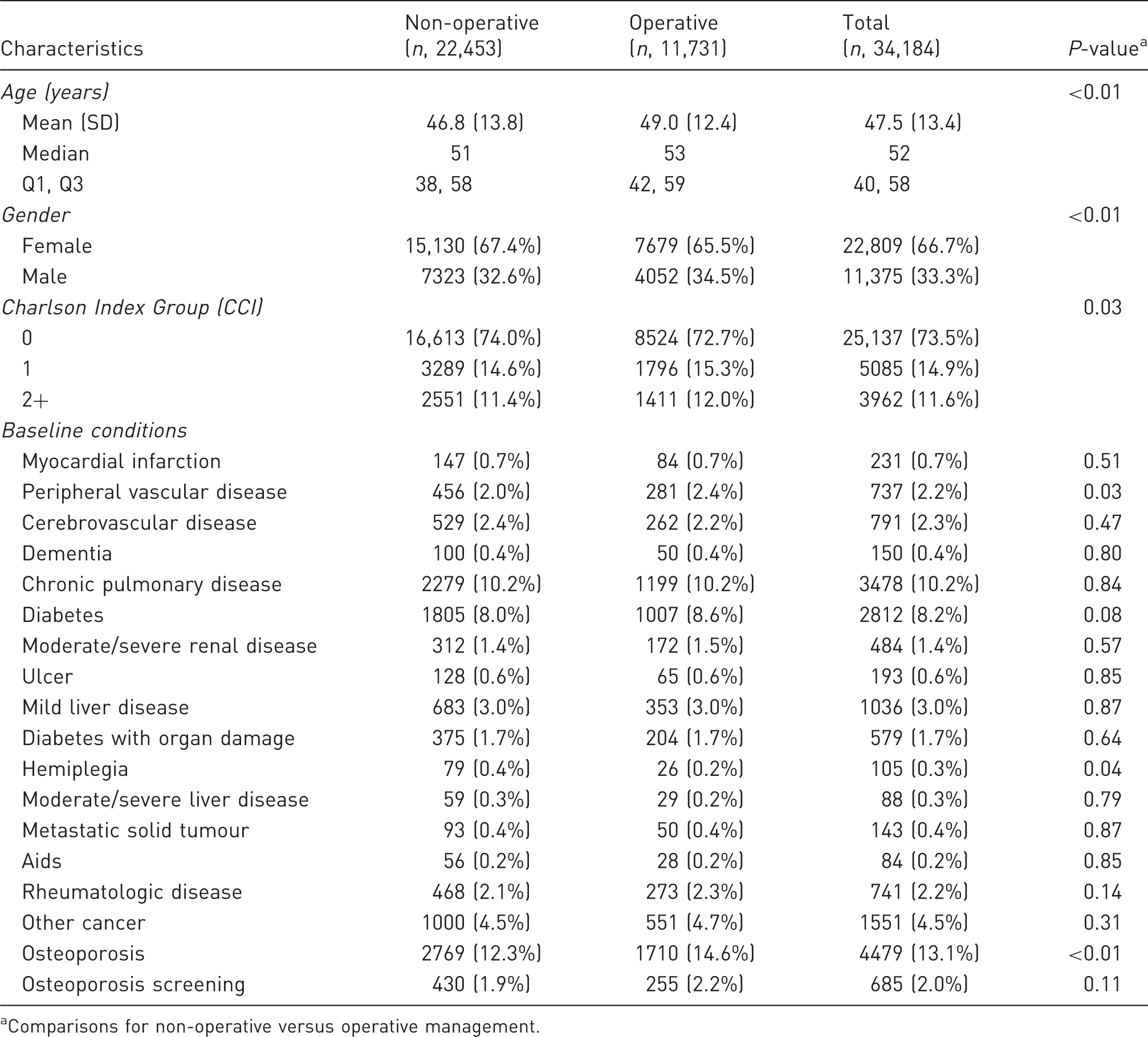
Comparisons for non-operative versus operative management.
Complication rates per 1,000 fractures subdivided by methods of management.

Comparisons among patients with non-operative versus operative (ORIF, EF, and CRPP) as well as non-operative versus each operative method.
ORIF: open reduction internal fixation; EF: external fixation; CRPP: closed reduction and percutaneous pinning.
Ninety-day and 1-year post-injury medical complications
Multivariable logistic regression of 90-day complications associated with operative versus non-operative treatment.
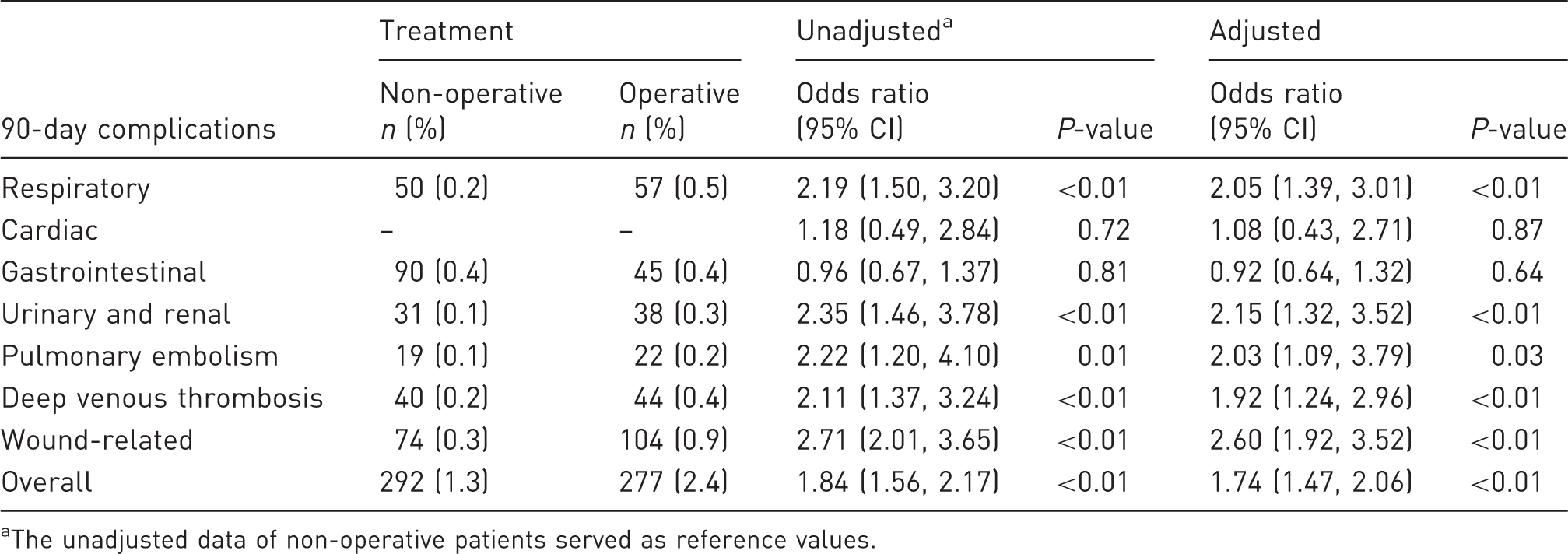
The unadjusted data of non-operative patients served as reference values.
Stiffness was the most common 1-year post-injury complication across all modes of treatment with a rate of 150.6 cases per 1000 fractures (Table 2), and the incidence of stiffness was significantly more common following operative management (p < 0.01). Fracture malunion was more common following non-operative management with an odds ratio of 0.83 (95% CI of 0.7–0.98) (Table 4).
The need of secondary procedures
Multivariable logistic regression of 1-year complications associated with operative versus non-operative treatment.
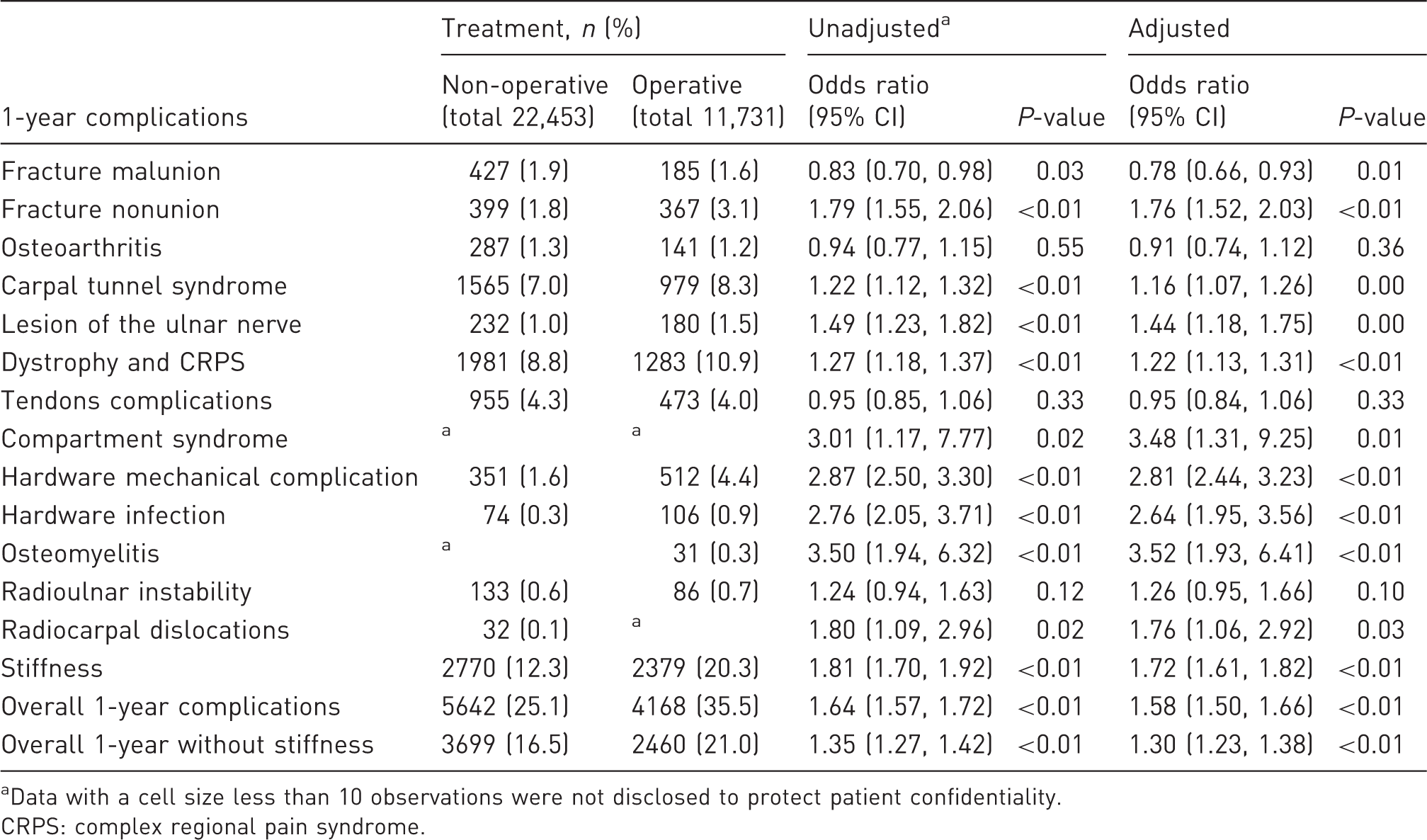
Data with a cell size less than 10 observations were not disclosed to protect patient confidentiality.
CRPS: complex regional pain syndrome.
Multivariable logistic regression of 1-year overall secondary procedures (same laterality) and carpal tunnel release.

Unadjusted data served as the references.
Regarding secondary operative procedures, increasing age per year (odds ratio 1.02, 95% CI of 1.01–1.02), male sex (odds ratio 1.20, 95% CI of 1.04–1.38) and history of osteoporosis screening (odds ratio 1.79, 95% CI of 1.18–2.71) were significantly associated with an increased rate of secondary operative procedures (p < 0.05).
Discussion
This large study with more than 34,184 DRFs over a 6-year period from all over the US provides comprehensive determination of secular trends in fracture management in the patients under 65 years of age. The results show that operative management of DRF results in significantly lower fracture malunion rates and secondary procedures, however both overall 90 medical complication rates and 1-year extremity-specific complication rates, specifically stiffness, are increased. These data provide relevant incidences for complications and secondary procedures, which are critical to reviewing the risks, benefits, alternatives and complications of the existing treatment options and providing anticipatory guidance to inform the decision making in patients between 18 and 64 years.
In this study, we found that the risk of 90-day medical complications was 16.6 cases per 1000 fractures in the patients under 65 years of age, and it was significantly higher in patients undergoing operative treatment. Among operative patients, medical complication rates were greatest with EF and least with closed reduction and ORIF. This reflects a greater degree of critically ill or multiply injured patients (with a higher CCI) in the operatively managed cohort.
We also found that 1-year extremity-specific complications were significantly greater following operative management, and among operative modalities, were highest following EF followed by ORIF and CRPP. Among these complications, stiffness was the most frequent. Stiffness was identified in 20% of patients managed operatively versus 12% of patients managed non-operatively, which is a rate consistent with previous reports identifying stiffness as a complication of DRF management (Heyer et al., 2019; Ikpeze et al., 2016; Synn et al., 2009; Teunis et al., 2015). The incidence of chronic regional pain syndrome was more frequent with operative management, and the overall rate of 9.5% in this patient age cohort is in line with previous reports ranging from less than 1% to 25% (Cowell et al., 2018; Crijns et al., 2018; Farzad et al., 2018).
Despite the increased incidence of complications with operative treatment of DRF, operative treatment was associated with a reduction in fracture malunion. An inverse age-dependent tolerability for residual anatomic deformity has been proposed, and is supported by the increased incidence of secondary procedures in the non-operatively managed cohort (Kong et al., 2019; Perugia et al., 2014; Synn et al., 2009).
From the present dataset, we were not able to discern the specific indications for secondary procedures, except for carpal tunnel release, or the time frame of occurrence within the first postoperative year; and as such future prospective studies will be required to assess whether operative management of DRFs has the potential to mitigate the need for secondary or revision procedures. Advanced age has also been shown to be an important factor associated with revision or reoperation following operative treatment of DRFs (Alter et al., 2019; Hollevoet et al., 2013; Li et al., 2019). Within this patient cohort, however, a significant proportion of patients with non-operatively managed DRFs elected to proceed with a secondary procedure.
Previously, our group investigated the outcomes and complications of DRF management in the elderly patients (DeGeorge et al., 2020). In the analysis of 13,713 DRFs in patients over the age of 65 years, non-operative management was more commonly performed (34.3%) than in the present series (27.3%); however the rates of ORIF, CRPP and EF were comparable. In both series, stiffness was the most common 1-year post-injury complication, however, this was more common in the younger population (115.0 vs. 150.6 cases per 1000 fractures). Taken together, regardless of patient age, operative management is associated with reduced secondary procedures at the expense of higher overall complications.
The limitations of this study are inherent to studies using large administrative databases. Not with-standing, we have tried to make the data relevant for practising physicians, where applicable. Large administrative databases are also subject to errors associated with inaccurate documentation through the use of ICD-9-CM or CPT coding. To address these limitations, we combined both diagnostic and procedural codes of DRF in an effort to improve the accuracy of reporting. The OLDW database contains only data points for commercially insured and Medicare Advantage enrolees; and therefore, the data presented herein may not be generalizable to all populations across Medicare categories or uninsured populations. Additionally, direct causal relationships are not possible using administrative claims data, and only relative trends and associations can be reported. Complications were identified based on the use of ICD-9 coding, however we did not specifically exclude patients with a history of that complication (i.e. stiffness 719.54, 719.53, 718.44 or 718.43). Therefore, it is possible that antecedent conditions could have been improperly recorded as complications. In addition, the mechanism of injury was not evaluated, and although motor vehicle accidents were excluded, this is dependent on the precision of billing information. Fracture patterns or fracture classifications were also not reliably reported and could not be included for analysis. Functional parameters were not recorded in the present study, and therefore no statements on the functional implications of the intergroup differences can be made.
An additional limitation was the inability to report on individual study cohorts with a sample size of less than 11, which is designed to protect patient confidentiality; however, many of the complications were observed in relatively few patients and therefore could not be independently reported. To address this issue, we included rank order lists for complications, including percentages for all sample sizes greater than 11 to allow the reader to draw conclusions on the frequency of these occurrences. Despite these limitations, this study with more than 34,184 DRFs over a 6-year period drawn nationwide provides comprehensive determination of, trends in fracture management in the younger than 65 years of age cohort, which is not available in previously published similar studies.
Supplemental Material
sj-pdf-1-jhs-10.1177_1753193420941310 - Supplemental material for Outcomes and complications of operative versus non-operative management of distal radius fractures in adults under 65 years of age
Supplemental material, sj-pdf-1-jhs-10.1177_1753193420941310 for Outcomes and complications of operative versus non-operative management of distal radius fractures in adults under 65 years of age by Brent R. DeGeorge Holly K. Van Houten, Raphael Mwangi, Lindsey R Sangaralingham and Sanjeev Kakar in Journal of Hand Surgery (European Volume)
Footnotes
Acknowledgements
We would like to thank Lindsey R Sangaralingham with Mayo Clinic Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery for statistical review of the manuscript.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Kakar is a consultant for Arthrex. The other authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this publication was made possible by funding from the Mayo Clinic Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.