
Abstract
Current guidelines from the British Orthopaedic Association state that if fractures of the distal radius are operated on then this should take place within 3 days of injury for intra-articular fractures, 7 days for extra-articular fractures and 3 days when a trial of conservative management has failed. This retrospective cohort study aimed to assess whether there was any difference in outcome between patients receiving timely or delayed surgery, using the Patient-Rated Wrist Evaluation score at >12 months after injury as the primary outcome measure. Data from 380 patients treated at two district general hospitals over a 5-year period were obtained using electronic databases to capture the demographics and treatment details and postal questionnaires to assess current function. The study showed no statistical or clinical differences in outcome measures between the timely or delayed cohorts in any of the three treatment groups.
Introduction
Fractures of the distal radius make up a large proportion of orthopaedic attendances, with an estimated 70,000 sustained in the UK each year (O’Neill et al., 2001). Although there has been a trend towards non-operative management in recent years (Song et al., 2015), a significant proportion of patients still have operative fixation of these injuries. Current advice from the British Orthopaedic Association (BOAST, 2017) and the British Society for Surgery of the Hand (2018) (the ‘Blue Book’) reflects guidance from the National Institute for Health and Care Excellence (NICE) (2016) that if distal radial fractures are to be operated on then this should be done within 3 days from injury for intra-articular fractures, within 7 days for extra-articular fractures and within 3 days from a decision being made to operate on fractures that have failed a trial of conservative management (FCM).
The full NICE document states that there is no concrete evidence behind these timings and there is limited information on the effect that the length of time between injury and operation has on patient outcomes after closed distal radial fractures in adults (Ashdown et al., 2020). It appears that this is a significant gap in knowledge given the frequency of these injuries and current pressures on operating lists. This study aimed to partially address this, starting with the null hypothesis that there is no significant difference in outcomes between patients treated within the NICE guidelines and those receiving delayed surgery, using the Patient-Rated Wrist Evaluation (PRWE) score at >12 months after injury as the primary outcome measure.
Methods
This was a retrospective cohort study. Trauma databases from two adjacent district general hospitals were used to retrospectively identify all distal radial fracture fixations over a 5-year period (September 2013 to September 2018 inclusive). ‘Fixation’ included open reduction with plate fixation and closed reduction with Kirschner (K)-wire fixation. Patients aged 16 years or less, fractures more than 3 cm proximal to the distal radioulnar joint, open and bilateral injuries were then excluded (Figure 1).
Flowchart showing recruitment of study participants.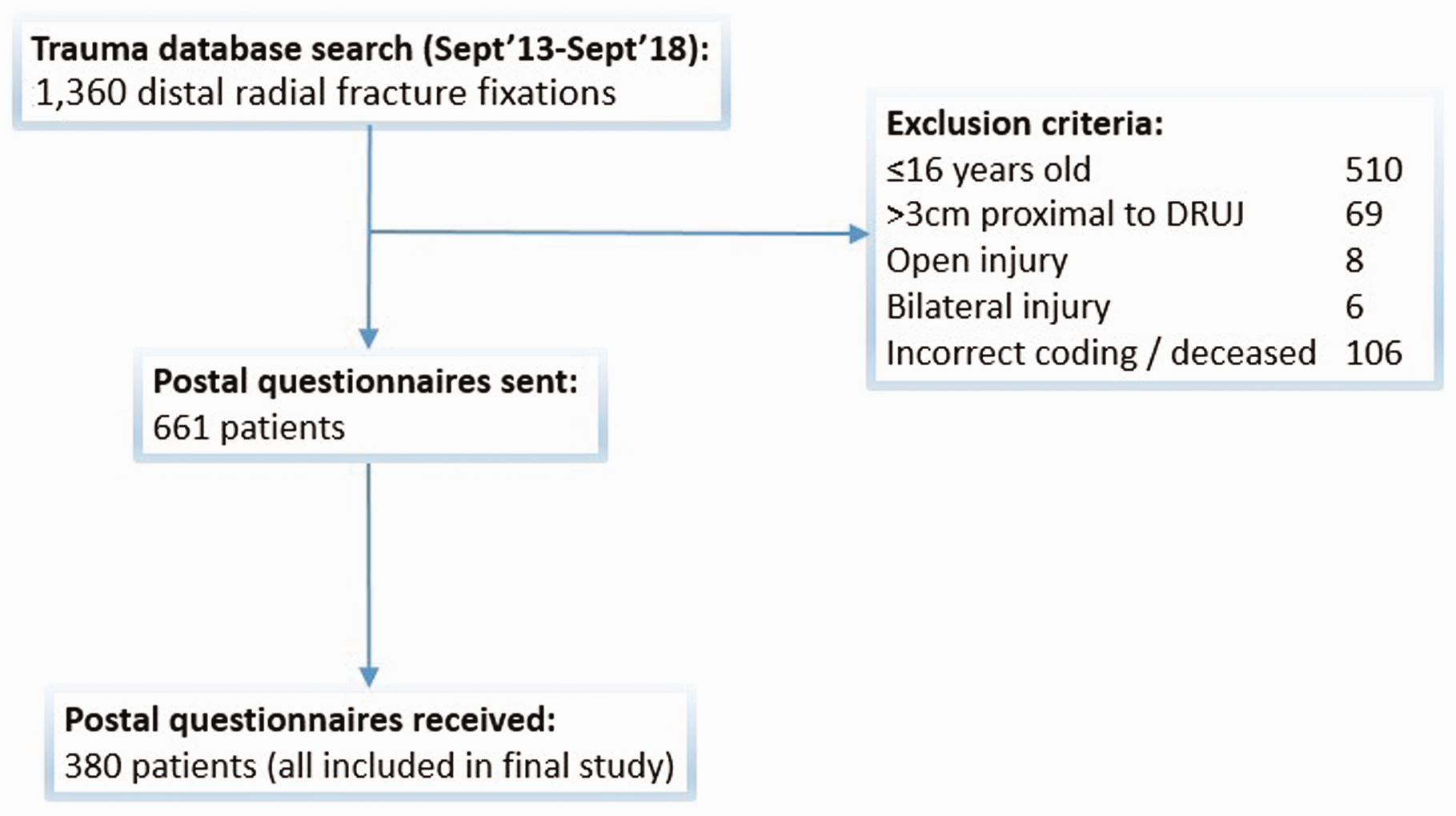
The hospitals’ radiography systems were used to recover patient demographics, injury characteristics and treatment information (including time to theatre). Electronic notes were accessed to identify whether patients required repeat operation at any point after the initial fixation.
Questionnaires were then sent to each patient by post, to complete and return. These contained questions on smoking and diabetic status, hand dominance and a PRWE questionnaire to assess current level of function of the wrist that had been operated on.
The PRWE is a reliable and validated patient-reported outcome measure (PROM), comprising of a 15-item questionnaire designed to assess a patient’s level of wrist pain and function; scores range from 0 (no disability) to 100 (severe disability) (MacDermid et al., 1998). It has been recognized as the most appropriate PROM to assess patients after distal radial fracture (Gupta et al., 2014). The minimum clinically important difference (MCID) specifically in the context of distal radial fractures has been stated to be 11.5 (Walenkamp et al., 2015), which is the value that we have used in this study.
Each patient category (intra-articular, extra-articular, FCM) was split into two cohorts: those operated within current timeline guidance, and those who had delayed surgery, with subsequent comparison of outcome measures between the two. The primary outcome measure was the PRWE score at >12 months from initial surgery; the secondary outcome measure was a need for re-operation at any point after initial fixation.
After this initial analysis, the study population as a whole was then re-arranged into a further two cohorts: patients undergoing surgery within 2 weeks from the time of injury, and those undergoing surgery after 2 weeks, again with the primary and secondary outcomes measured. This secondary re-grouping was done to answer the specific question posed in the British Society for Surgery of the Hand Blue Book as to whether a delay to surgery of more than 2 weeks had an effect on outcome.
Statistical analysis
Statistical analysis was done using MedCalc Statistical Software version 19.2.1. Binary categorical data were analysed using Fisher’s exact test, and numerical continuous data with a normal distribution pattern were analysed using Student’s unpaired t-test. Numerical data that did not have a normal distribution were analysed using the Mann–Whitney U test. Differences with a p-value of <0.05 were deemed to be statistically significant.
Previous studies have reported mean PRWE scores at 12 months after distal radial fixation of approximately 30, with a standard deviation (SD) of 20 (Costa et al., 2015; Hull et al., 2011; MacDermid et al., 2003). An appropriate sample size for detecting an 11.5-point difference (the MCID) between two cohort groups at 5% level with 80% power was therefore established to be a minimum of 47 patients in each cohort group (assuming equal group numbers).
Results
Comparison of baseline and injury characteristics between cohorts, with primary and secondary outcome measures.
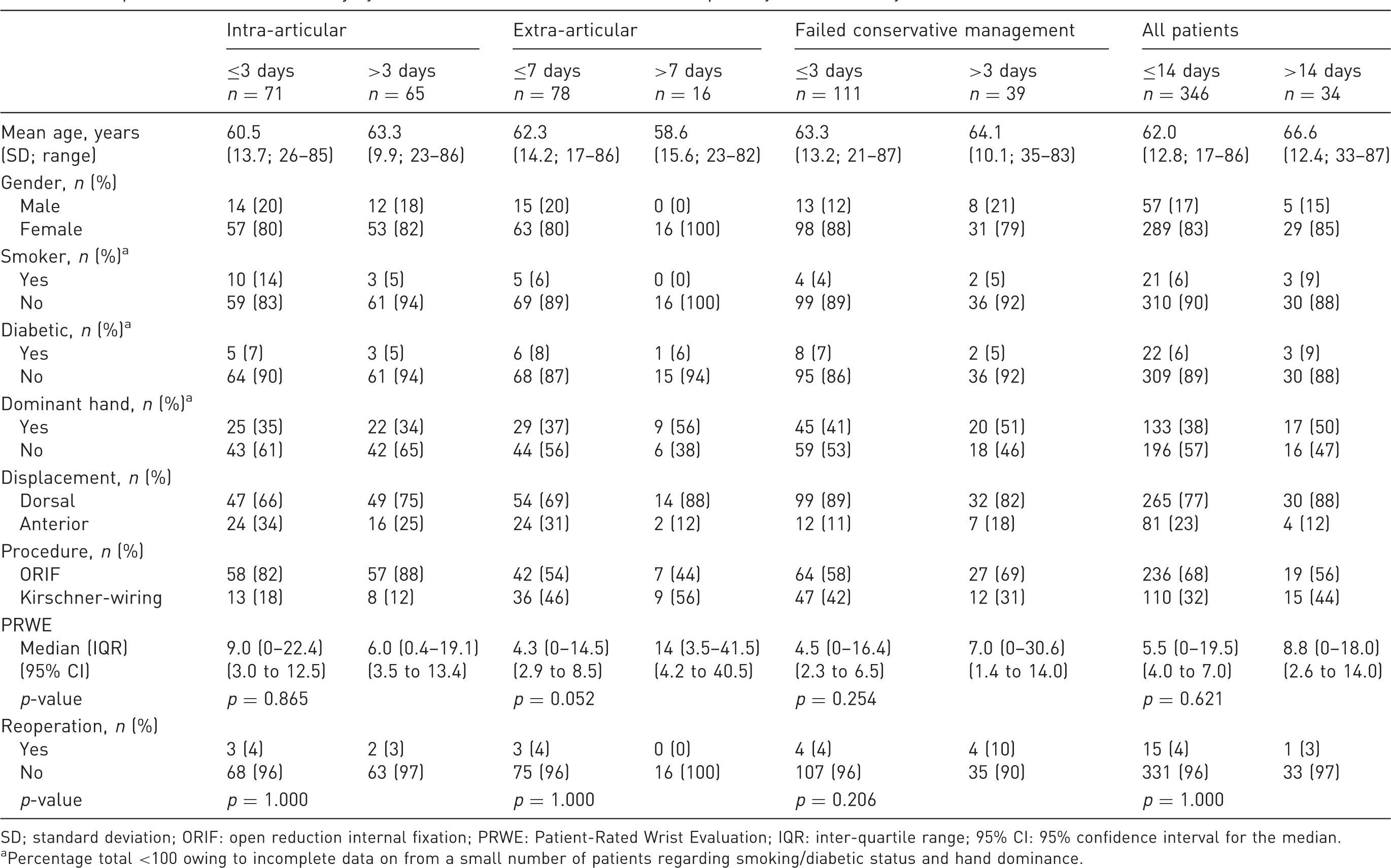
SD; standard deviation; ORIF: open reduction internal fixation; PRWE: Patient-Rated Wrist Evaluation; IQR: inter-quartile range; 95% CI: 95% confidence interval for the median.
Percentage total <100 owing to incomplete data on from a small number of patients regarding smoking/diabetic status and hand dominance.
PRWE scores did not follow a normal distribution curve, so the difference in median scores between cohorts was used rather than the mean. None of the three treatment groups showed differences in median PRWE between the timely and delayed fixation cohorts that exceeded the MCID value of 11.5, or that were statistically significant. The extra-articular group showed the largest difference between the two cohorts, of 9.7 (median PRWE scores of 4.3 (timely) vs 14.0 (delayed)), although this difference still fell outside the thresholds for both clinical and statistical significance (Table 1; Figure 2).
Scatter diagrams of relationship between the follow-up Patient-Rated Wrist Evaluation (PRWE) and time to operation in (a) intra-articular fractures, (b) extra-articular fractures and (c) fractures that have failed conservative management. The vertical lines show the cut-off times for surgery under the current national guidelines for each treatment group.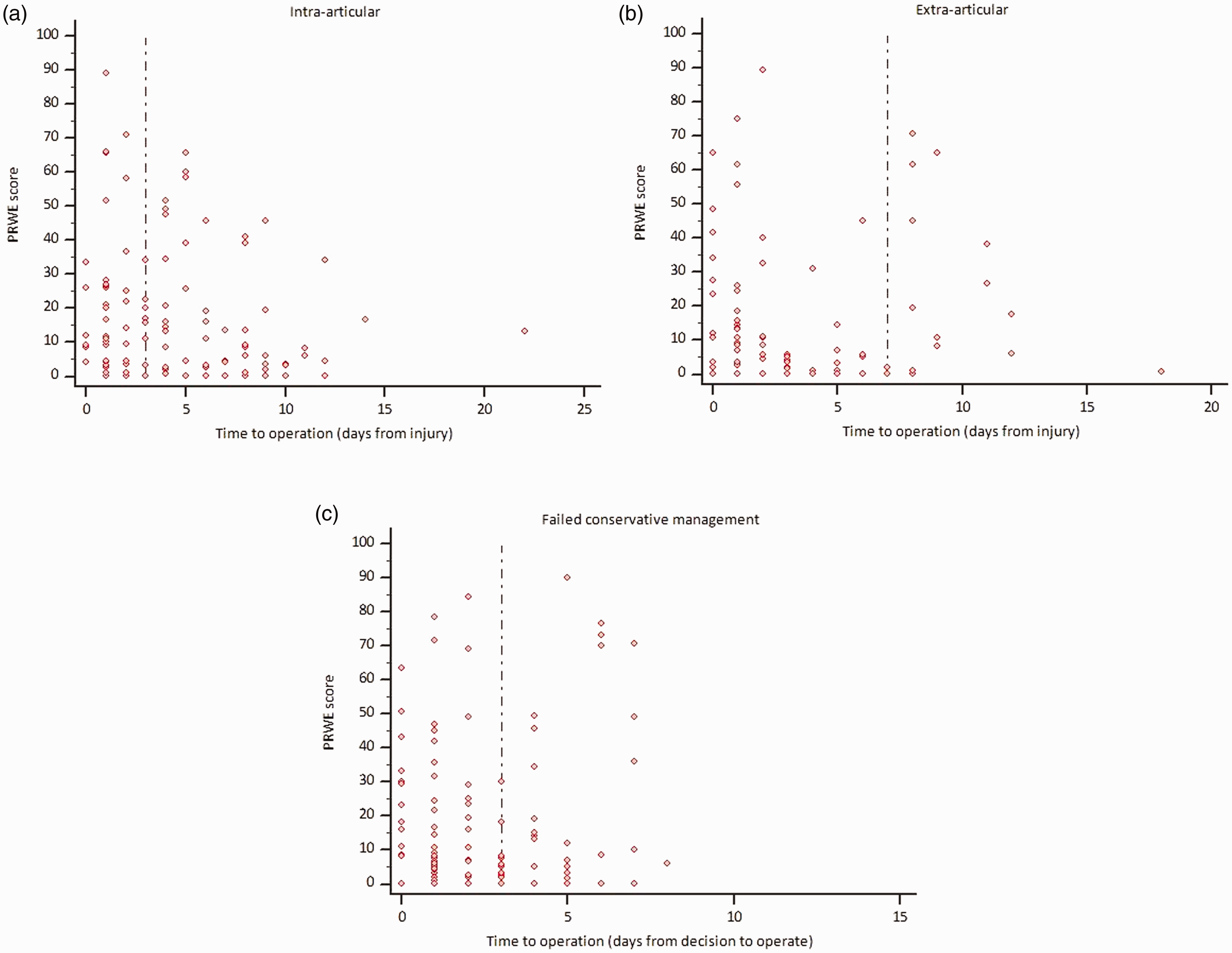
None of the treatment groups showed significant differences in reoperation rate between the timely and delayed fixation cohorts (Table 1). Of the 16 patients requiring reoperation, 12 underwent removal of implants with the remaining four cases requiring revision of fixation.
When the study population was rearranged into a further two cohorts comprising of those operated within 2 weeks and those operated on after 2 weeks, there was again no significant difference in primary or secondary outcome measures (Table 1).
When patient demographics and injury characteristics were analysed individually against PRWE scores for the whole study population, patients aged under 65 had a statistically significant higher median PRWE (8.0 vs 4.0; p = 0.008), although again this difference did not meet the threshold for the MCID. Patients aged under 65 also had a significantly higher reoperation rate (6.5% vs 2.1%; p = 0.040).
Discussion
This study has shown no significant differences in PRWE scores or re-operation rates between patient cohorts undergoing timely versus delayed fixation. The study contained a large number of patients across two separate institutions covering a 5-year time period, with a lengthy follow-up time, meaning results are likely to be generalizable to a wider population. Baseline characteristics were comparable between cohorts in each of the treatment groups, meaning that these known confounders were unlikely to have had an effect.
When the whole study population was examined against baseline characteristics, only an age of under 65 was associated with a statistically significant difference in either primary or secondary outcome measures. This is probably because younger patients have higher functional demands and so are more likely to perceive a decrease in function after injury and are more likely to be considered for reoperation if a poor outcome is encountered.
Operative management may be delayed for many reasons. In many cases the fracture is viewed as a relatively minor injury in a patient who is ambulant and can cope at home while waiting for operation, meaning that the patient is often pushed to the ends of busy trauma lists. It may also be the case that the more complex fractures are delayed to allow for further imaging (of the 13 patients in the study who underwent CT scanning, ten were in the intra-articular delayed surgery cohort), or to wait for a specialist upper limb surgeon to become available to do the operation. Whatever the decision-making processes involved, it would certainly be helpful for clinicians to have an awareness of whether or not a delay may significantly affect an individual patient’s long-term outcome.
The rationale for the current guidelines is the concept that after these respective timeframes, intra-articular fragments become more difficult to reduce, and extra-articular fractures become more difficult to reduce in a closed manner (National Institute for Health and Care Excellence, 2016). The concern is that a delay therefore leads to more difficult or invasive surgery, and a potentially poorer long-term outcome. In future studies it would be interesting to see whether patients receiving delayed surgery had sub-optimal fracture reduction, a longer operating time or increased complications. It would be useful to obtain data on the grade and sub-speciality of the operating surgeon, as more complex cases (predisposed to a poorer outcome) waiting for an experienced or specialist surgeon may be more likely to fall into the delayed surgery cohort. It is also worth noting that the timings for the FCM group are taken from the time of the decision to operate rather than from the initial injury, potentially leading to some heterogeneity within the cohorts for this group.
There are inherent weaknesses because of the retrospective nature of the study and unequal sample sizes. We did not have access to baseline PROM scores, which may have been helpful for comparison, and follow-up was at a variable rather than fixed time period. Using postal questionnaires to gauge current function is susceptible to selection bias, with patients who have experienced poor outcomes possibly more likely to be disproportionately represented in responses. However, well over half of patients responded and PRWE scores were generally lower across our population than in previously published studies looking specifically at distal radial fractures (Costa et al., 2015; Hull et al., 2011; MacDermid et al., 2003), meaning this is unlikely to have been an issue. When adjusted for unequal sample sizes, the cohorts were sufficiently powered, with the single exception of the extra-articular delayed treatment group.
The data from this study have not provided sufficient evidence to reject the null hypothesis, with no evidence that delayed surgery (using current national guidelines) for distal radial fractures has an effect on long-term functional outcome or reoperation rates. With current ever-increasing pressures on operating lists, and difficult decisions being made about prioritizing cases, this raises the question whether the guidelines may need reconsidering. Further studies with large prospective cohorts of patients, and with baseline PROMs for comparison, would be beneficial to help provide more information.
Footnotes
Acknowledgements
Thanks to C. Christie, R. Dunbar, F. Chiwah, K. Davoudi, A. Cavenagh, O. Catton and T. Clarke for their assistance with data collection.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Patients were informed in a covering letter attached to postal questionnaires that if they responded then their anonymized data would be included in the study.
Ethical approval
This study was approved by the Research & Development departments at participating institutions, with formal ethical approval not required due to its retrospective observational nature.