
Abstract

Dear Editor,
In 2018, we reported 30 explanted NeuFlex® implants with fractures at various sites. Subsequently, we have encountered two more cases of early catastrophic failures of NeuFlex® metacarpophalangeal (MCP) joint implants at the hinge.
A 45-year-old man with painful thumb MCP joint arthritis received a NeuFlex® MCP joint arthroplasty in another hospital. Initially, he reported good pain relief and movement, but within 4 months, he experienced significant thumb pain, with reduced strength and movement. On examination at 1 year postoperatively, there was mild MCP joint instability with lateral stressing, opening to 20° ulnarly and radially. Radiographs showed a NeuFlex® implant in situ with no adverse features. Following failed non-operative treatment, the implant was removed and was found to be fractured at the hinge. The bone implant interfaces looked normal with a thin shiny lining membrane, with no obvious inflammation and no bone spikes to explain the failure. The arthroplasty was converted to an arthrodesis with good pain relief and thumb function.
The second and third cases occurred in a 55-year-old lady with rheumatoid arthritis who presented with bilateral index finger MCP joint pain. In 2013, she had a right index finger NeuFlex® size 30 arthroplasty with a very good outcome, achieving a range of motion from 0°–50° and good pain relief. Upon request, she underwent the same procedure for her left index finger in 2016, with a NeuFlex® size 30 implant MCP joint arthroplasty for her left index finger. The surgery and postoperative rehabilitation were performed in exactly the same manner as her right side. She initially reported good relief of her preoperative symptoms but by 3 months postoperatively had developed recurrent pain. No cause was found, and the joint was re-explored at 6 months postoperatively. The implant was again found to be fractured at the hinge, with no evidence of bone spikes or infection.
As the patient had done well on the right hand, the arthroplasty was revised with another size 30 NeuFlex® implant. The postoperative regimen was more conservative, with restricted mobilization and prolonged splintage to beyond 6 weeks postoperatively. Initially, she reported good pain relief, but within 4 months of the operation she developed recurrent pain, stiffness and weakness. Her radiographs were again unremarkable (Figure 1(a) and (b)). The left index finger MCP joint was re-explored after a year (delayed due to other medical causes) and the implant was found to be fractured at the hinge (Figure 1(c)) for no obvious reason. The implant was changed to a size 7 Swanson implant with the stems trimmed to fit the bone tunnels. She achieved good pain relief and mobility with no evidence of implant failure after 2 years.
(a) and (b) Radiographs showing the fractured index finger NeuFlex® implant in situ. (c) Explanted NeuFlex® implant fractured at the hinge.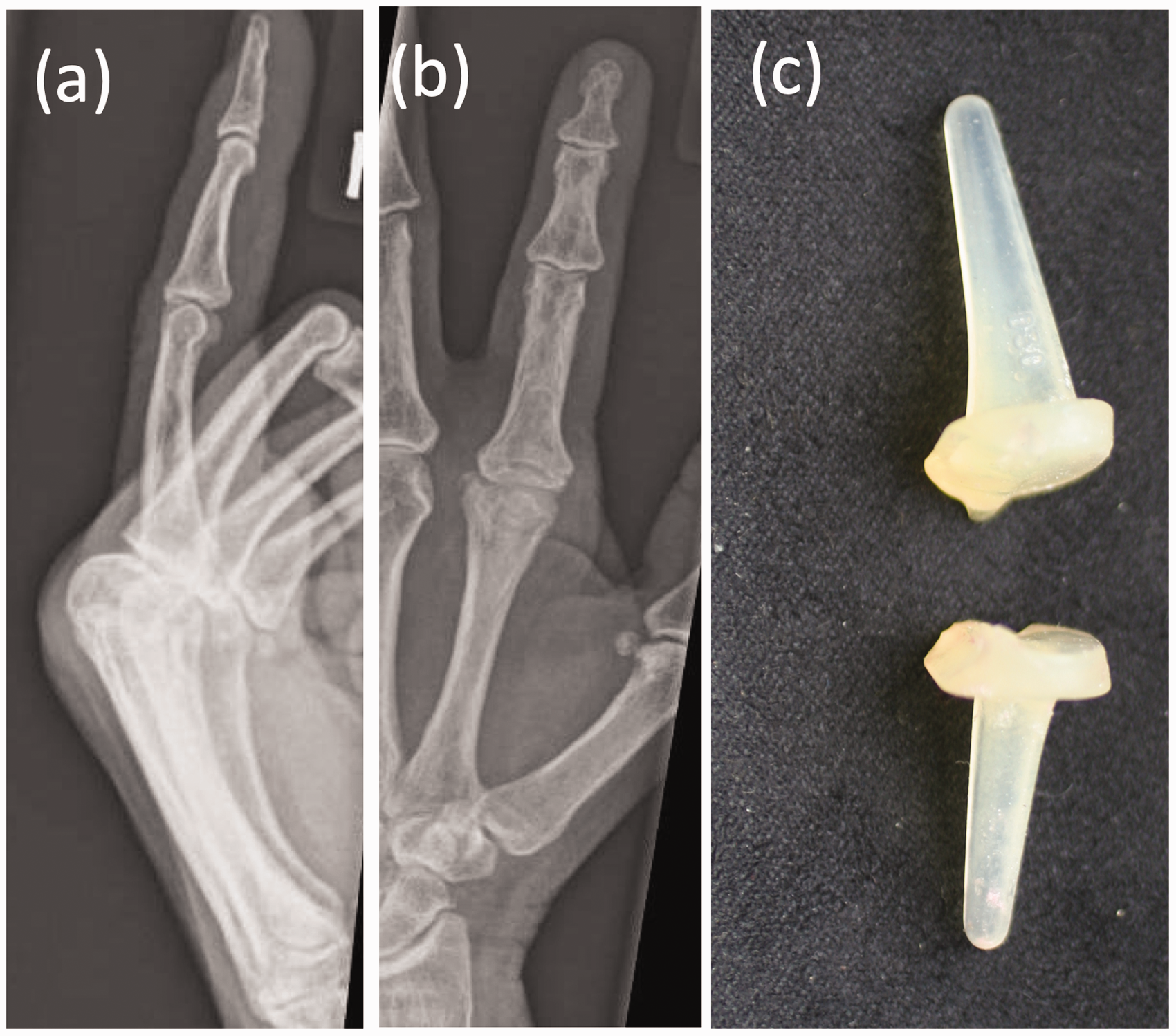
The failure of NeuFlex® implants at the hinge has only recently been identified (Joyce and Giddins, 2018). We reported on 30 NeuFlex® explants: seven were intact; nine had fractured at the junction of the body and distal stem; 11 at the hinge; and three at both the distal stem and hinge. These further cases have identified a risk of catastrophic early failure of NeuFlex® implants at their hinge. No other silastic finger joint implant has been shown to fail so quickly, although some patients have had early revision of silastic arthroplasties (Trail et al., 2004) for dislocation. Although an implant could fail due to fatigue fracture, similar to other silicone rubber implants, these typically fail at the junction of the body and distal stem and not the hinge.
The explanted implant from the second patient was included in the earlier study, where the focus had been on the sites of ruptures, whereas in this report we elaborated on patient details to demonstrate the lack of any explanation when implants fail. There were no patient factors that could have helped predict the failures; in each case, the individuals were reasonably healthy with good neighbouring joints. Both achieved very good early thumb or index finger MCP joint movement where there was not only flexion and extension loading, but appreciable lateral loading with pinch.
From our observations, a flexible hinge appears to be an area of weakness and manufacturers may need to consider thickening this area to make it more resistant to tear propagation. Finally, as lateral loading increases rotational stresses, which could potentially increase the chance of implant failure, perhaps a more suitable implant for single joint replacement in high demand patients may be one without a hinge, such as with the Swanson design.
There are limitations to our hypotheses as this is only a small series of three cases and indeed, good results can be achieved, as shown by the longevity of the implant in the right index finger of the second patient. Overall, surgeons need to be aware of the vulnerability of this implant and the mode of failure, especially when searching for the cause of unexplained early symptoms after an initial good result following NeuFlex® MP joint arthroplasty.
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.