
Abstract

Dear Editor,
Radial polydactyly with a floating-type thumb duplicate is usually treated with simple excision of the pedunculated digit. More recent reports have suggested that interphalangeal (IP) joint deviations can occur in conjunction with these types of radial polydactyly, a deformity that can persist or worsen after excision surgery (Lourie et al., 1995; Saito et al., 2018). Most recently, Hanaka et al. (2021) investigated the clinical features of 12 patients with floating type radial polydactyly and found that two of the 12 thumbs showed a deviation at the IP joint preoperatively, which did not improve postoperatively. In addition, two of 10 patients with no deformity preoperatively developed IP joint deviation postoperatively. The authors did not explore the anatomical structures responsible for the IP joint deviation, as they mentioned this would cause unnecessary extension of the surgical procedure. The cause of the deviation has thus remained unclear.
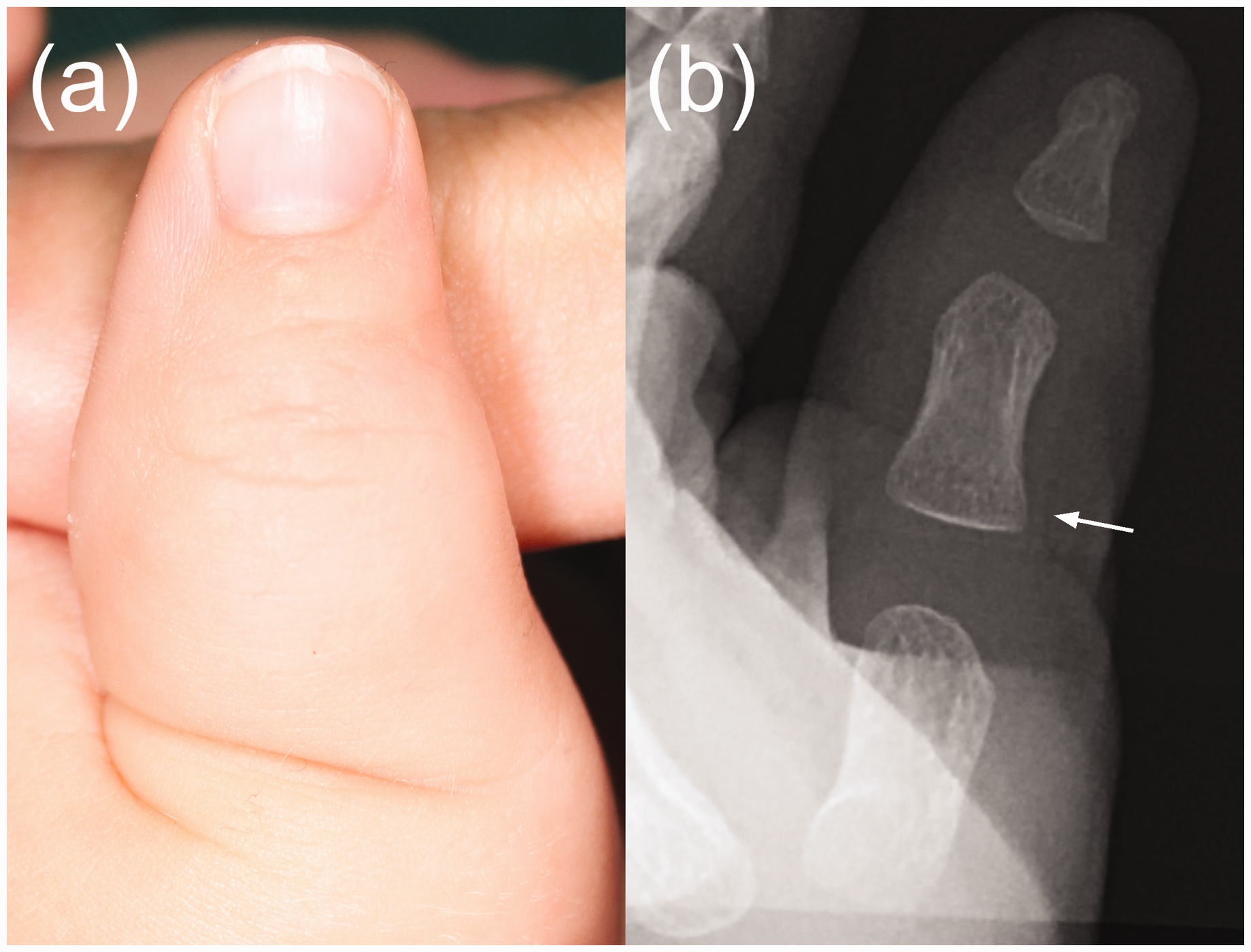
A 3-month-old boy presented to our department with a floating type radial polydactyly at the level of the distal proximal phalanx (Figure 1(a)). The rudimentary radial thumb duplicate contained a nail and small bony fragment and was connected to the ulnar thumb with a narrow pedicle measuring about 3 mm. The IP joint of the ulnar thumb was radially deviated at 25° (Figure 1(b)). Surgery was performed at 6 months to remove the radial duplicate. The pedicle was dissected and contained a nerve, vessels and tendon-like cords. We decided to perform extensive exploration of the volar aspect of the ulnar duplicate, revealing a malalignment of the flexor pollicis longus (FPL) tendon, which was located radial to the central longitudinal axis of the thumb (Figure 1(c)). FPL centralization was achieved by releasing the distal part of the ulnar sheath of the A2 pulley, detaching the radial part of the distal attachment of the tendon and suturing it to the more central position (Figure 1(d)). No osteotomy was performed and the reconstructed thumb was protected with a cast for about 3 weeks, followed by taping for an additional 3 weeks. The IP joint radial deviation improved to 10° at 1 year after surgery (Figure 2).
Preoperative photograph (a) and radiograph (b) show a floating-type radial polydactyly with radial deviation at the interphalangeal joint. Note the asymmetrical configuration of the proximal phalanx (arrow) with radial broadening of the base. Intraoperative photograph (c) showing malalignment of the flexor pollicis longus tendon, located radial to the central longitudinal axis of the thumb (purple lines). (d) After centralization of the flexor pollicis longus tendon. Photograph (a) and radiograph (b) taken 1 year after surgery show a decrease in the radial deviation of the retained thumb. Note the improved morphology of the proximal phalanx with less radial broadening at the base (arrow).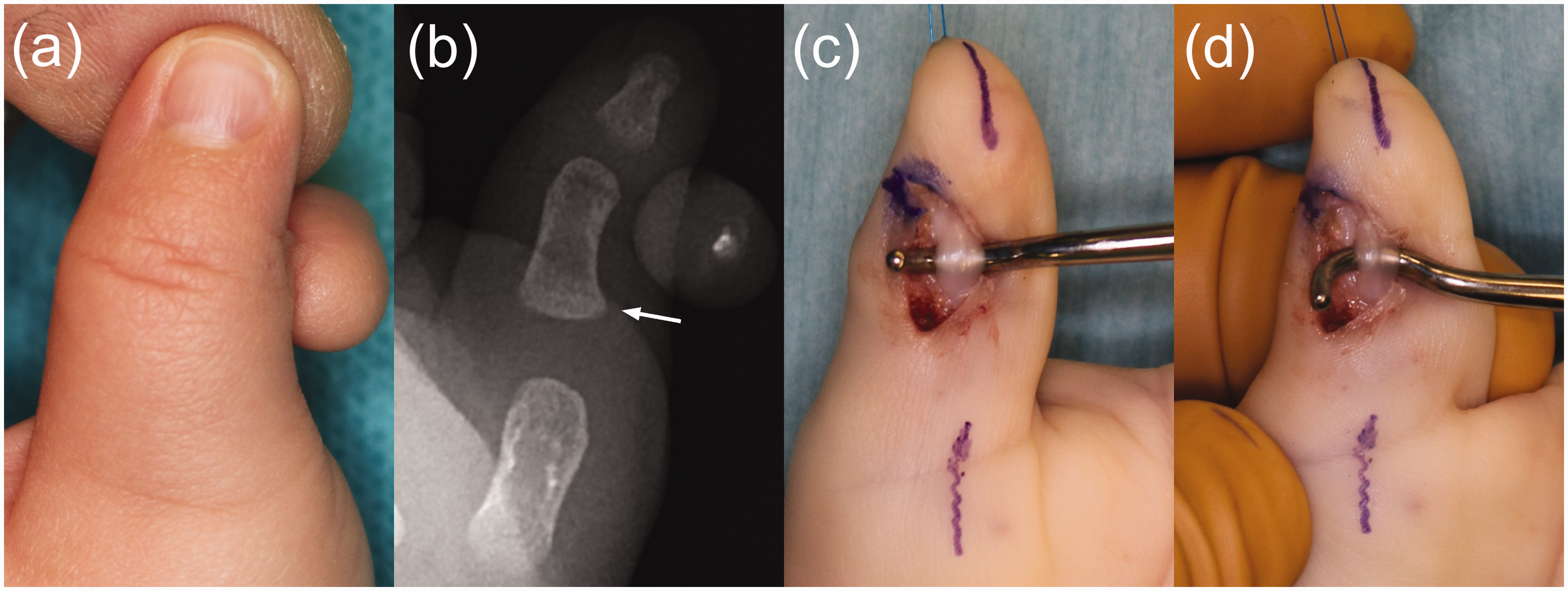
Deformities such as joint angulation or deviation are commonplace in radial polydactyly. It is currently accepted that these deformities associated have a biomechanical basis; for example, the zigzag morphology of a Wassel Type IV duplicated thumbs can be associated with the aberrant location of the FPL in combination with the lack of the normal A1 pulley system (He et al., 2017). Lourie et al. (1995) reported a case of marked IP joint radial deviation after suture ligature of a soft tissue tag at birth. They suggested that there might be a similarity in the causative mechanisms between the floating type radial polydactyly with the zigzag deformity found in Type IV duplicated thumbs, because the duplication was at the metacarpophalangeal joint level as evidenced by a widened metacarpal head. In our case, there was found to be a malalignment of the FPL, despite the level of bifurcation being distal to the metacarpophalangeal joint with a normal metacarpal head. Radiographs of our patient, however, demonstrated a radial broadening at the base of the proximal phalanx (Figure 1(b)).
It would perhaps have been the accepted norm to simply excise the radial duplicate in our patient, but we decided to explore the FPL tendon and centralize it during the initial surgery. A decreased IP joint deviation after FPL centralization would suggest that the tendon was the main deforming force responsible for the deformity. Interestingly, there was decreased broadening of the radial aspect of the proximal phalanx, which may also indicate that a deforming force had been removed (Figure 2(b)). There remains some degree of deviation at 1-year follow-up, which may indicate either that there are other residual soft tissue abnormalities or that the deviation would eventually correct itself with more growth time. In conclusion, we recommend surgical exploration of radial polydactyly even in floating-type cases, which may initially appear inconspicuous. This is especially relevant when there is a degree of joint deviation preoperatively.
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.