
Abstract

Dear Editor,
The high nonunion incidence (15%) observed after appropriate scaphoid fracture treatment is caused by its vascular supply, micro-movement at the fracture site and absence of callus formation due to its 80% cartilage coverage (Yeo and Kim, 2018). Treatment strategies based on the characteristics of the nonunion were developed to reduce this high incidence of failure. Slade and Dodds (2006) recommended a cancellous bone graft bridging the two fragments for a stable nonunion with a bone loss of more than 2 mm but less than 10 mm. We retrospectively reviewed the results of our minimal incision technique for management of stable scaphoid nonunions with this degree of bone loss. These were treated with local reaming, bone grafting and screw fixation through a palmar approach.
Between 2014 and 2020, we saw 20 patients with scaphoid nonunions without prior surgeries. Nine presented with Grade IV nonunion according to Slade and Dodds’ (2006) classification. All nine were non-smoking males with an average age of 25 years. The mean time between trauma and surgery was 24 weeks (range 20–33). Outpatient surgery was carried out under brachial plexus block. Through a 1-cm volar incision, a K-wire was placed along the longest central axis followed by a 2.5-mm cannulated drill bit until reaching the nonunion site to debride the devitalized bone. Cancellous bone graft plugs of 2.3 mm (11 gauge) were harvested percutaneously from the ipsilateral Lister’s tubercle with a bone biopsy needle. These were pressed onto the K-wire and gently pushed into the scaphoid with the cannulated drill bit (Figure 1). Once the graft was inserted in the nonunion site, drilling was continued to within 2 mm of the proximal pole (Slade and Dodds, 2006). This also allowed impaction of the cancellous bone along the inner portion of the nonunion site. Thereafter, a headless compression screw was inserted for stabilization. Three months postoperatively a CT scan was obtained to evaluate bone healing. We obtained preoperative and 3-month postoperative ranges of motion and visual analogue scale scores, along with grip strength, which was measured with a dynamometer (JAMAR, Sammons Preston, Bolingbrook, IL, USA).
(a) K-wire is inserted into the plug after harvesting. (b) K-wire with the mounted graft is inserted into the scaphoid. (c) The graft is gently impacted with the drill bit into the nonunion site.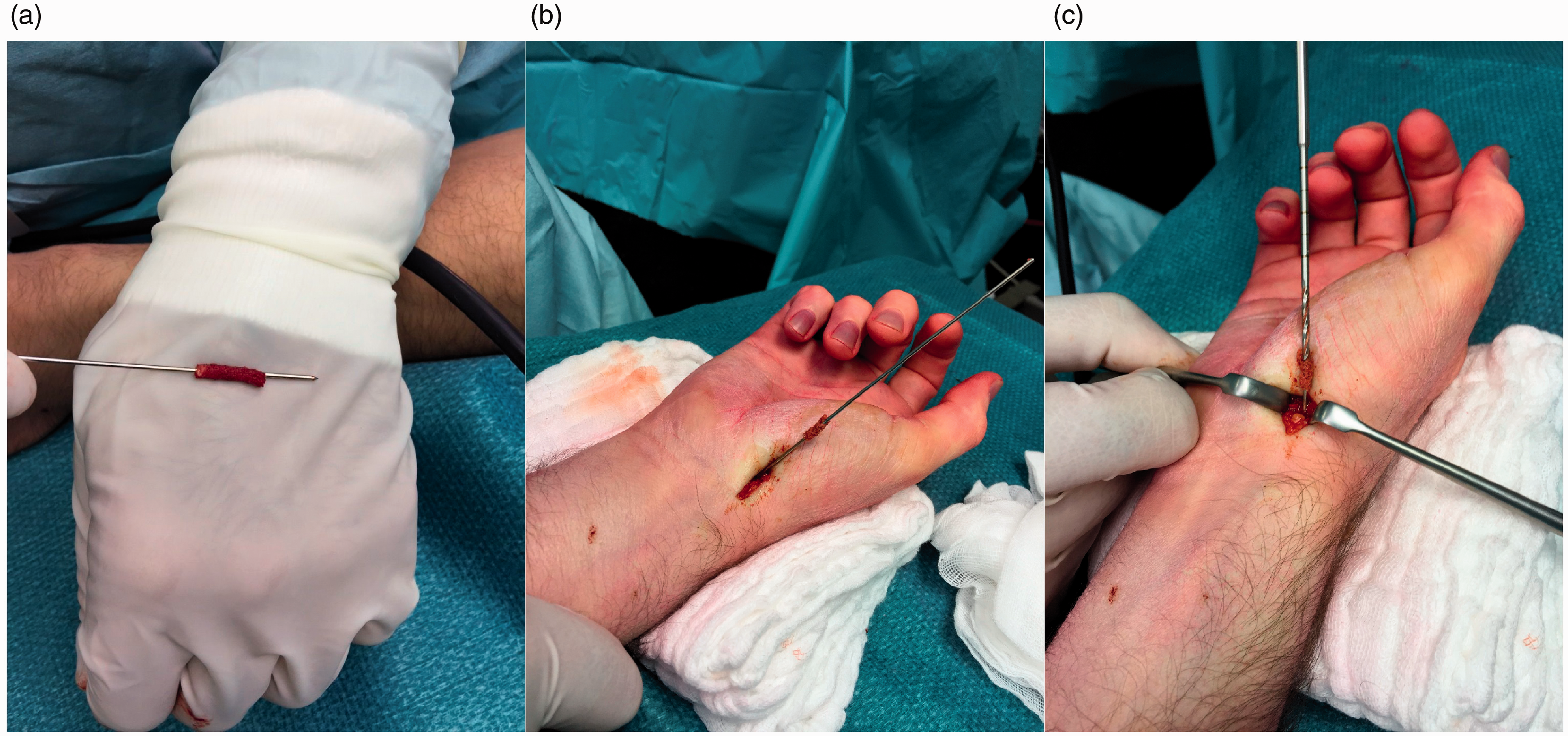
All scaphoid nonunions were consolidated 3 months postoperatively, as confirmed by CT scan. The mean follow-up was 30 weeks (range 17–44). No complications were noted. Out of the nine patients, all six working patients returned to their previous work 3 months after surgery, and six of seven avocational athletes resumed contact sports without complaints. The remaining patient decided to postpone returning to sports until the next season, 10 months later. Six screw removals took place due to deep tissue irritation. The visual analogue scale scores improved from a median of six (IQR 1) to one (IQR 1). The median range of motion of the operated wrists was 123° (IQR 19) for flexion and extension, which is similar to values described in the literature; the preoperative value was 92° (IQR 5). The median postoperative grip strength for the operated wrists was 29 kg (IQR 2), the contralateral side was 34 kg (IQR 2).
Percutaneous reaming debrides devitalized bone at the nonunion site. Slow reaming does not destroy the peripheral fibrous connections that act as a barrier to synovial fluid, thus preventing the dilution of local osteogenic stimulants that may lead to faster and more predictable healing (Slade and Dodds, 2006). The bone graft impacted through the minimal incision adequately replaces the loss of cancellous bone and bridges the fragments. Using the minimal incision technique, the scar does not preclude further procedures. The harvest site involves the same wrist and can be carried out without additional anaesthesia (Pinder et al., 2015).
Arthroscopy has a role in scaphoid reduction, assessment and treatment of concomitant ligamentous injuries. Arthroscopic scaphoid nonunion management has been described. However, it requires more skill, materials and time. If surgeons are not familiar with this form of management, they can begin by selecting patients who have no degenerative changes of the wrist and whose scaphoid is well aligned (Wong and Ho, 2019). The high incidence of screw removal is due to screw protrusion and soft tissue irritation. This error is due to the compression effect and the percutaneous technique, as the ruler measures the screw length plus the thickness of the cartilage, and eventually some connective tissue. We advise to deduct at least 2 mm from the actual measure to avoid this complication. A limitation is that the study is non-comparative and that all patients were non-smokers. This minimally invasive technique seems to be a valuable option addressing stable scaphoid nonunion with substantial bone loss but without the presence of a humpback deformity.
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Obtained from CUB Erasme’s ethics committee (P2020/318) and Hopital d’Ixelles’ ethics committee (CEHIS/2020-18).