
Abstract

Dear Editor,
Communications between the median and ulnar nerves are well described (Smith et al., 2019). Of the four most common variations, the Martin-Gruber interconnection is the most proximal, occurring in the forearm with a prevalence of 20% (Roy et al., 2016). We report an unusual case of a median to ulnar nerve interconnection in the upper arm.
A healthy 9-year-old girl sustained a closed Type 3 Gartland supracondylar fracture of the left humerus (Figure 1(a)). She complained of pain and tingling in all the digits of the left hand and diminished touch sensation in the ring and little fingers. A closed reduction with medial and lateral pinning was performed and achieved an acceptable reduction (Figure 1(b)).
Supracondylar fracture of left humerus before reduction (a), and after pinning (b).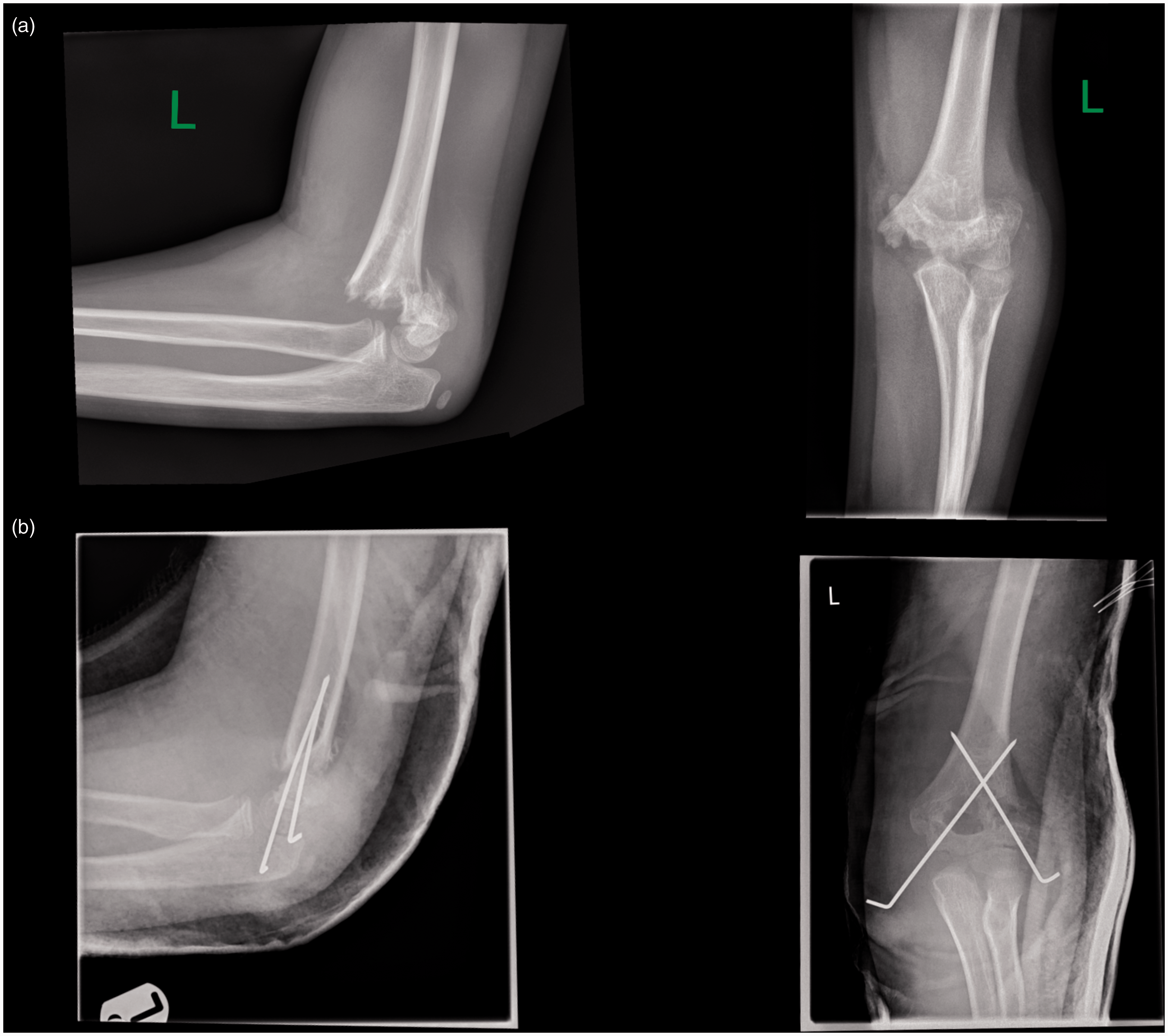
At 5 weeks, the patient had persistent neuropathic pain and allodynia across all digits, worst in the ring and little fingers. Clinical examination revealed mild clawing of the left hand and altered sensation in all digits with a dense sensory deficit in the ulnar two fingers. The function of the flexor pollicis longus, the flexor digitorum profundus of the index and middle fingers, and forearm pronation, were weak, suggesting injury to the anterior interosseous nerve (AIN). Clinical examination of motor function of the intrinsic muscles was limited by pain. Sonography demonstrated continuity of ulnar and median nerves and a normally appearing brachial artery around the humeral metaphyseal region, but these structures could not be visualized distally due to fixed flexion of the elbow.
Under general anaesthesia and tourniquet control, the K-wires were removed, and the median and ulnar nerves were explored. The ulnar nerve was found directly adjacent to the K-wire but without division. A cubital tunnel decompression and neurolysis was performed. The median nerve was approached through an anterior incision. It was encased in thick scar. Dissected under a microscope, it divided into three branches at the distal third of the humerus: one branch contributing to the ulnar nerve proximal to the cubital tunnel and two branches with distal interconnections at the level of the elbow (Figure 2). The more medial of the latter two branches, presumed to be the AIN, was 100% divided. This was repaired using interrupted 9-0 Ethilon sutures and fibrin sealant.
The median nerve trunk in the distal upper arm divided into three branches: (a) contribution to ulnar nerve, (b) main sensory branch and (c) anterior interosseous nerve with 100% laceration.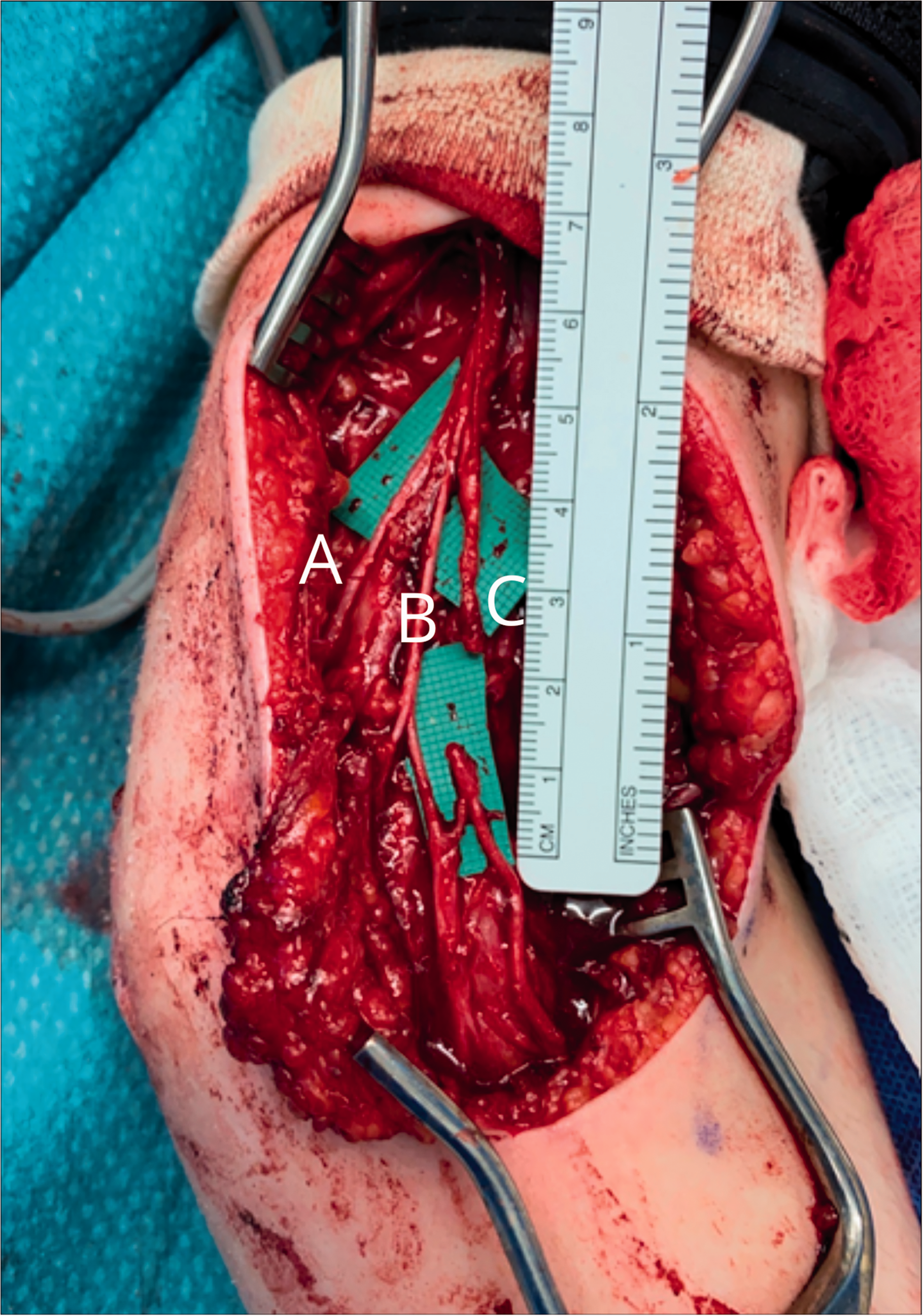
The severe pain resolved immediately postoperatively, which we surmised was due to neurolysis of the ulnar and median nerves. Over 7 months, the patient reported gradual recovery. The AIN-innervated muscles regained full power at 3 months, followed by ulnar and median-innervated intrinsic muscles, which achieved Medical Research Council Grade 4 to 5 by 7 months. Froment’s test was positive at 3 months and negative at 7 months. Sensation improved in all digits and was near normal in the ulnar digits at 7 months.
The described nerve pattern may complicate the diagnosis of brachial plexus injuries or more peripheral lesions. According to the meta-analysis of Babal et al. (2010), supracondylar fractures are associated with primary nerve injuries in 11%, most commonly the AIN. Nerve injury induced by lateral-only pinning occurred at a weighted event incidence of 3%, while the introduction of a medial pin elicited neurapraxia at a weighted event incidence of 4%. Also, arthroscopic interventions and surgical treatment of peripheral nerve compression syndromes around the elbow may cause iatrogenic nerve injury.
From our case, we conclude that nerve exploration is important in the absence of clinical improvement and that anatomical variants should be considered, particularly when the clinical assessment is not definitive.
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from a legally authorized representative (parent) for their anonymized information to be published in this article.