
Abstract

Dear Editor,
Spontaneous posterior interosseous nerve (PIN) palsy may be associated with neuralgic amyotrophy or fascicular constriction (Ochi et al., 2011). Since both conditions mostly have good functional outcome after conservative treatment in young patients, nonsurgical treatment of spontaneous PIN palsy in children is usually advised (Al-Ghamdi and Ghosh, 2018; Ochi et al., 2011). We present two cases with no sign of recovery after more than 8 years.
Case 1. A 16-year-old boy presented at our hospital with impaired finger extension in his right hand. He had been diagnosed with a spontaneous PIN palsy when he was 7 years and treated conservatively. Until recently, he managed his daily life without active extension of his fingers, therefore he had not undergone any treatment. His parents first realized his finger disability when he started swimming, and this disability progressed for months without pain. His strengths were as follows: extensor carpi radialis longus five, extensor carpi radialis brevis (ECRB) zero, extensor pollicis longus (EPL) and extensor indicis proprius (EIP) one, and extensor digitorum communis (EDC) and extensor digiti minimi (EDM) zero according to the British Medical Research Council grading system. Neither space occupying lesions nor malformations were seen on radiological or MRI examinations. However, MRI suggested denervation of the extensor muscles. Electrophysiological examination confirmed the diagnosis of a PIN palsy. Needle electromyography showed spontaneous fibrillation potentials and positive sharp waves in the extensor carpi ulnaris and no electrical activity in the other muscles innervated by the PIN. Considering that incomplete spontaneous PIN palsy may partially recover by simple interfascicular neurolysis even 17 years after the onset (Ochi et al., 2015), interfascicular neurolysis was performed. No pathological feature, such as compression of the nerve, entrapment, fascicular constriction or hourglass-like deformity, was seen (Figure 1). The patient and his family refused tendon transfer procedures. Fourteen months later, fibrillation potentials were seen in the EIP but there were no clinical signs of recovery.
Interoperative photograph of posterior interosseous nerve in case 1. (a) Macroscopic view. (b) Microscopic view. Interfascicular neurolysis was performed. No pathological feature like compression of the nerve, entrapment, fascicular constriction, or hourglass like deformity is present.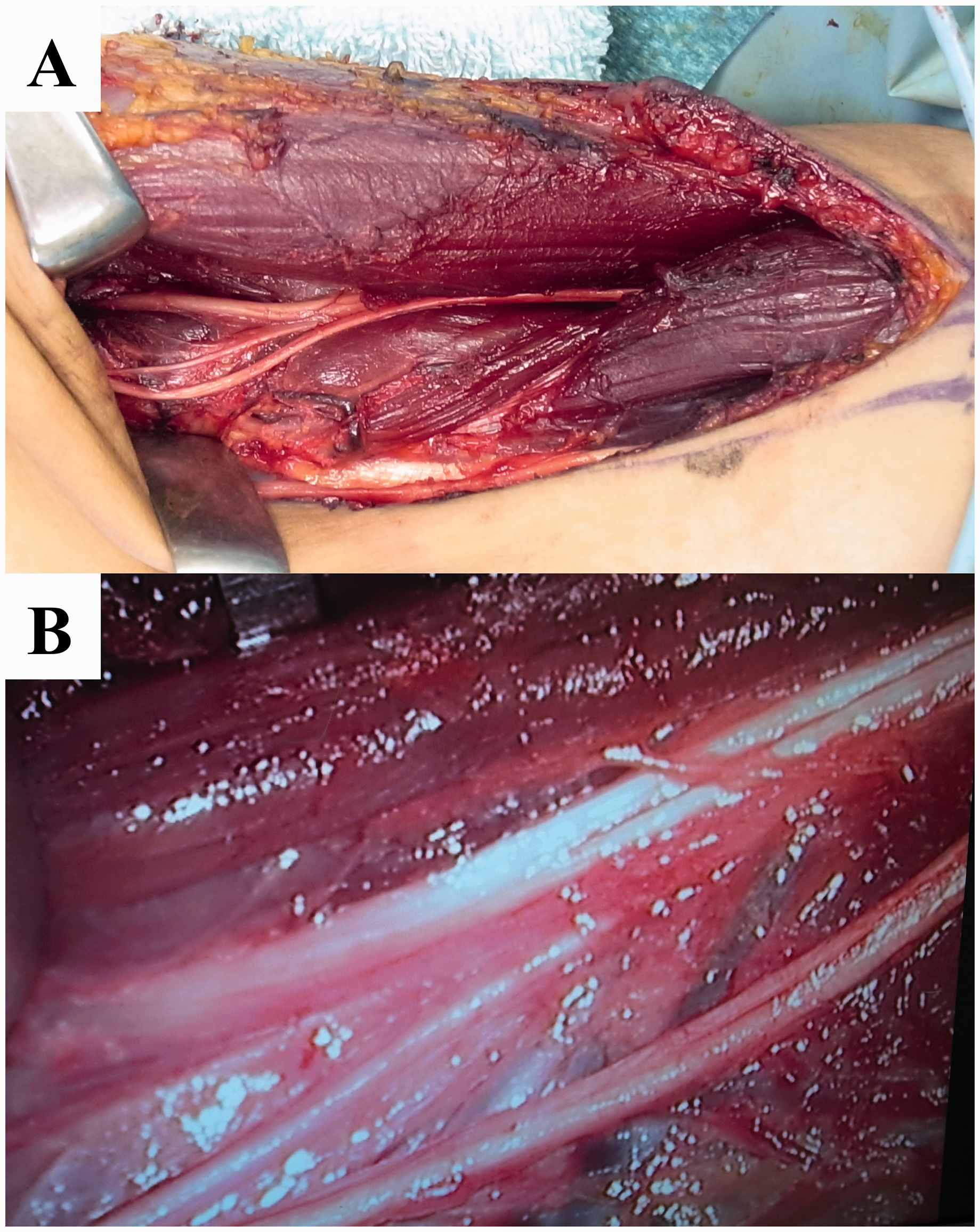
Case 2. A 13-year-old girl was referred to our hospital because of difficulty in extending her ulnar-sided fingers. Her parents had noticed the finger dysfunction when she had difficulties putting on gloves at the age of 5 years. The finger extension problems progressed for months without pain. Muscle strength was as follows: ECRB five, EPL and EIP five, EDC zero and EDM one. The brachial plexus image was highly intense on T2 weighted MRI. No space occupying lesion or malformation was seen on radiological or MRI studies. Thus, we diagnosed a spontaneous PIN palsy. Since there were no signs of recovery, we reconstructed finger extension with tendon transfers when the patient was 14 years. Her family declined the recommendation of performing a neurolysis.
Spontaneous PIN palsy in childhood is rare, and natural recovery is reported to be favourable in teenagers (Ochi et al., 2011). Both those who believe the condition is due to neuralgic amyotrophy and those who believe it is caused by fascicular constriction favour conservative treatment in children. However, in adults, slow progression of the palsy for more than a month is one of the poor prognostic factors associated with conservative treatment (Ochi et al., 2013), which also was the case in our two paediatric cases. We therefore conclude that surgical treatment should be considered, not only in adult-onset spontaneous PIN palsy, but also in children if there is no spontaneous recovery or even slow worsening of the palsy during conservative treatment.
Footnotes
Acknowledgements
We thank all the members of the Department of Exploratory Medicine on Nature, Life, and Man at Toho University Medical School, the Department of Orthopaedic Surgery, National Center for Child Health and Development, the Department of Orthopedic Surgery, Tokyo Dental College Ichikawa General Hospital, and the Department of Orthopedic Surgery, Keio University School of Medicine for their support.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported in part by the grants-in-aid for scientific research from the Japan Society for the Promotion of Science to KO [grant number 19K09612]; and the Nukada Foundation Grant to KO [grant number 2018-A].
Ethical approval
The study protocol was approved by the Institutional Review Boards of our institutes, study numbers 20120430 (case 1) and 2021-045 (case 2).
Informed consent
Written informed consents were obtained from the patients before enrolling to this study.