
Abstract
Accurate assessment of distal radioulnar joint (DRUJ) stability is increasingly recognized as an important part of clinical examination of the wrist. The ability of 30 specialist UK hand surgeons to clinically determine the stability of four volunteers’ wrists was assessed. Volunteers’ wrist stability had previously been confirmed with a validated measurement rig. Use of the wrist ballottement test as the primary examination technique yielded a positive predictive value of 81%, a negative predictive value of 55%, a specificity of 94% and a sensitivity of only 24%, for the detection of DRUJ instability. No correlation between background speciality (orthopaedic versus plastic surgery), nor years of clinical experience was found. Clinical assessment of DRUJ instability among experienced clinicians appears unreliable and instability is typically under recognized. Previous research to date using this clinical assessment method as a parameter of success is therefore brought into question.
Introduction
The distal radioulnar joint (DRUJ) is anatomically and biomechanically complex (Nagata et al., 2013; Stuart et al., 2000). Studies suggest that approximately 20% of DRUJ stability is bony in origin (Stuart et al., 2000), while the vast majority of soft tissue stability originates from the triangular fibrocartilage complex (TFCC) (Ward et al., 2000). Other structures contributory to dynamic stability include the pronator quadratus (Stuart, 1996), the interosseous membrane (Malone et al., 2015; Watanabe et al., 2005), the joint capsule (Watanabe et al., 2004) and the extensor carpi ulnaris tendon (Spinner and Kaplan, 1970).
DRUJ motion can occur in three planes; translational, longitudinal and rotational (Tolat et al., 1996). This combined with the complex biomechanics, makes assessment of DRUJ stability difficult. There are a number of recognized methods of clinical assessment (Zimmerman et al., 2012), and it is widely agreed that critical to DRUJ testing is comparison of the two lateral sides in the same patient. The most commonly used bedside test is that of the ‘ballottement’ or ‘shuck’ test (Gofton et al., 2004). This test is typically deemed positive with initiation of pain or ‘excessive’ movement/translation compared with the contralateral side. Several authors have simulated clinical assessment of DRUJ instability on patients and cadavers and felt it to be reliable (Kim and Park, 2008; Lindau and Aspenberg, 2002; Lindau et al., 2002; Moriya et al., 2009; Onishi et al. 2017). In addition, previous authors (Iida et al., 2014) have reported that ulnar deviation of the wrist makes the DRUJ more lax on clinical testing, whereas it makes the DRUJ more stable in unstable wrists. Our experience of assessment of DRUJ clinically (Pickering et al., 2016) and in particular in assessing DRUJ instability in conjunction with a distal radius fracture (Giddins and Pickering, 2022) indicates that clinical assessment of DRUJ instability is unreliable.
Our hypothesis was therefore that clinical assessment of DRUJ instability is unreliable.
The aim of the study was to assess the reliability of clinical assessment of DRUJ instability among experienced clinicians in comparison with a proven mechanical assessment of DRUJ instability.
Methods
We selected four volunteers (all authors of the study) who had a range of normal and unstable DRUJs. Thirty experienced clinicians (Tang and Giddins Grade 4 or 5, (Tang and Giddins, 2016)) were asked to assess the wrists of all four volunteers using any clinical assessment they wished, namely they could examine the DRUJ’s in the ways they thought best for as long as they needed. No clinical information was provided although the general age and gender of the volunteers was clear. Each examination was performed in a warm quiet room. No examiner watched the examinations of any other examiner. Each examiner was briefed in advance of the purpose of the study, namely to see whether clinical examination was reliable in detected abnormal ranges of DRUJ shear. The examiners recorded whether each DRUJ they assessed was stable or unstable. As all examiners were asked to assess both wrists of each volunteer and all examiners used a comparative approach to their assessments (performing a test or range of tests on one side before repeating in an identical manner on the other side), it was anticipated that where a volunteer had asymmetrical wrists (i.e. one stable and the contralateral unstable) identification of the unstable side would have been more obvious.
Each examiner utilized an individual approach to assess the DRUJ. All examiners performed the shuck test as the primary method of assessment. All examiners performed the shuck test with the forearm and hand in neutral, and the majority repeated the test with varying degrees of forearm pronosupination and wrist deviation. Assessment of elbow range of movement, comparative achievable forearm pronosupination, visual assessment of distal ulna prominence and observation of discomfort in the volunteers’ faces were all common features of the clinical examination techniques used.
Each volunteer had been assessed in advance using a proven rig (Pickering et al., 2016) to reliably measure their DRUJ shear and determine their stabilities.
Results
We assessed 30 examiners, 25 men and five women, with a combined total of 468 years of consultant level practice (mean duration 15, range 1–35). Of these individuals, 25 were of an orthopaedic surgery training background and five of a plastic surgery background. All had a current sole, or at least primary, practice in the speciality of hand surgery and reported themselves as a specialist in this field.
Volunteers' demographics and wrist stabilities.
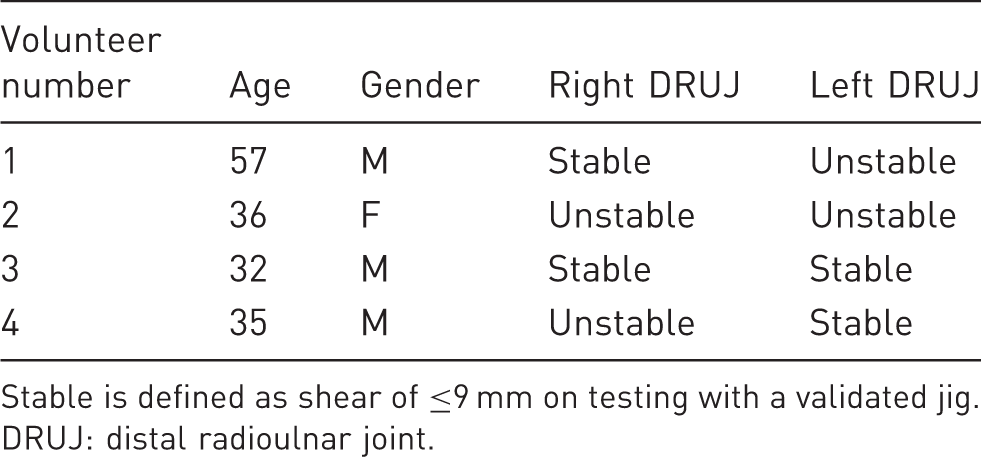
Stable is defined as shear of ≤9 mm on testing with a validated jig.
DRUJ: distal radioulnar joint.
Examiner findings for each of the eight wrists are shown in supplementary online Table S1, including incorrect assessments. No examiner correctly identified the stability of all eight wrists, with the best result being seven of the eight wrists correctly identified (achieved by one individual) and the worst result being only three of the eight wrists correctly identified, which occurred with three examiners.
While anticipated that instability would have been easier to detect in individuals with asymmetrical wrist stability, it was in fact only identified correctly 11 times in the 60 assessments of volunteers with asymmetrical wrists (18%). Instability was correctly identified most often in the volunteer with bilateral wrist instability, although this only occurred 18 times during the 60 wrist examinations performed on this individual (30%).
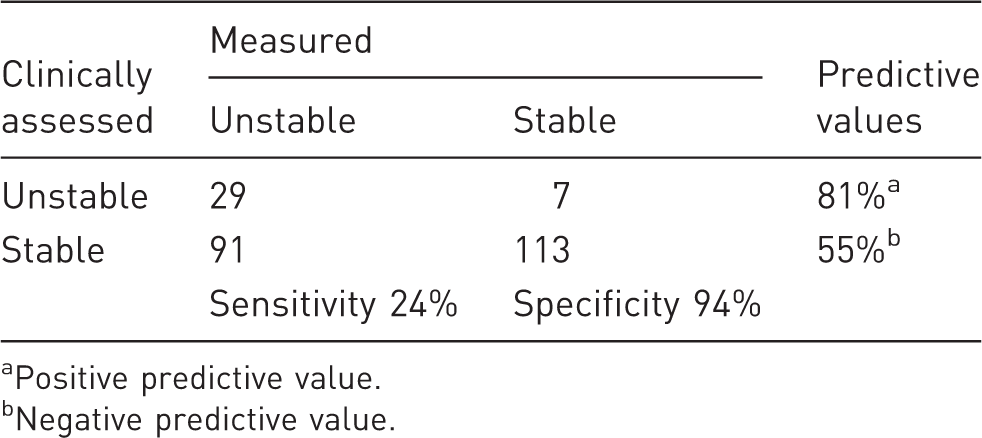
Overall, the stable wrists were correctly noted to be stable in 87–100% (mean 94%) of cases, while unstable wrists were identified correctly as unstable in only 17–33% (mean 24%) of cases. The calculated sensitivity of the examiners’ assessments was 24% (95% confidence interval (CI) 17–33%), but calculated specificity was 94% (95% CI 88–97%). The examiners demonstrated that clinical assessment of a wrist being unstable had a positive predictive value of 81% (95% CI 61–90%), but that an assessment of a wrist being stable had a negative predictive value of only 55% (95% CI 53–58%) (Table 2). There was no correlation between years of experience, nor background speciality training, and accuracy of assessment (Figure 1).
Scatter plot of years of clinical experience against correctly assessed wrists. Circular dots represent surgeons with an orthopaedics background, while triangles represent a plastic surgery background. Summary of results. Positive predictive value. Negative predictive value.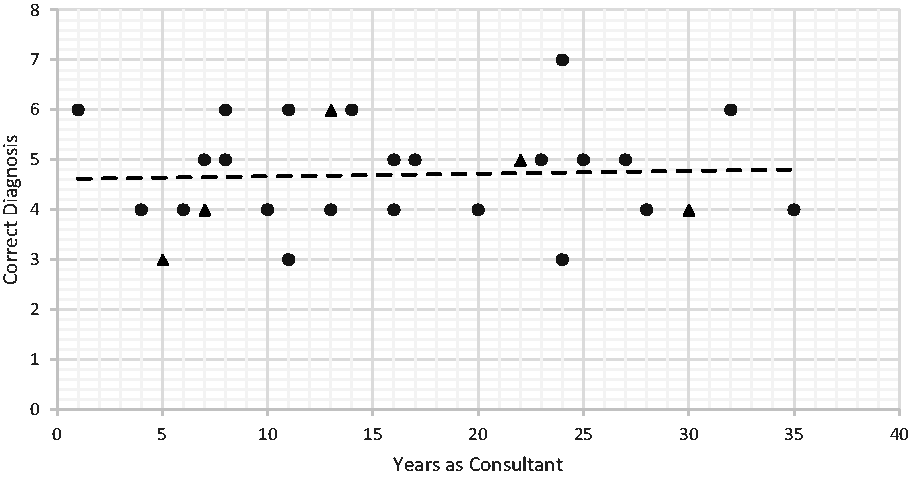
Discussion
This study shows that clinical assessment of instability is very unreliable with a sensitivity of only 24%. These data would fit with our clinical experience and, in particular, our study of DRUJ instability associated with wrist fractures where we showed that 100% are unstable to measurement (Giddins and Pickering, 2022). This contradicts previous studies where isolated, ballottement test-based clinical assessment of instability post-distal radius have shown instability in only 2% to 37% of cases (Geissler et al., 1996, Lindau and Aspenberg, 2002).
Each examiners’ test was not recorded, and it is not possible to truly know how each examiner came to their final decisions. It is also not possible to know from this study which physical examination tests, and their individual variations, of DRUJ instability are more and which less reliable in clinical assessment. Our experience suggests that, in general, the most sensitive clinical test of DRUJ instability is assessment of DRUJ instability performed in maximal pronation and compared with the contra-lateral side.
This study of clinical testing of volunteers with proven DRUJ instability shows that most clinicians are unable reliably to detect DRUJ instability. By implication clinical reports of instability should be considered unreliable. We recommend use of a proven mechanical system like a rig, or imaging such as CT or ultrasound scans (Kim and Park, 2008, Thiellemann et al., 2020). In our experience, use of a validated objective device or technique, providing feedback and ‘calibration’ to an individual’s personal clinical assessment, makes clinical application of tests for DRUJ instability more reliable (Giddins, 2016).
There are limitations of this study: only four volunteers were tested, but there were an equal number of stable and unstable wrists; and an examination of the DRUJ would normally be part of a whole clinical assessment, including taking a history.
In conclusion, this study of 30 experienced clinicians clearly shows that clinical assessment of DRUJ instability is unreliable and that instability is typically under recognized. Previous research to date using this clinical assessment method as a parameter of success is therefore also brought into question.
Supplemental Material
sj-pdf-1-jhs-10.1177_17531934211054282 - Supplemental material for The reliability of clinical assessment of distal radioulnar joint instability
Supplemental material, sj-pdf-1-jhs-10.1177_17531934211054282 for The reliability of clinical assessment of distal radioulnar joint instability by Greg Thomas Pickering, Nicola Francesca Fine, Thomas David Knapper and Grey Edward Bence Giddins in Journal of Hand Surgery (European Volume)
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.