
Abstract
This retrospective study reviewed 28 patients, aged 10 to 17 years, who underwent corrective osteotomy for malunion of the proximal phalangeal distal condyles at a mean of 9 weeks (range 2–52) from injury. There were 19 patients treated with K-wire and nine patients with locking plates. The two groups were comparable for trauma mechanism, fracture type, time delay from injury and the type of initial treatment. The K-wire group had a shorter duration of operation and shorter time to union than the plating group. For both groups, postoperative radiographs showed significant correction, which remained unchanged until the final follow-up (minimum 12 months), although greater residual coronal angulation was found in the K-wire group. The outcomes in 17 of the 28 patients were graded as excellent or good according to the Al-Qattan classification, with no difference between the groups. The complication rate was also similar between the groups, while the locking plate group had a higher rate of secondary surgery.
Introduction
Fractures of the distal condyles of the phalanges include extra-articular phalangeal neck fractures and intra-articular phalangeal head fractures. Surgical fixation is typically indicated for displaced distal condylar fractures in children (Al-Qattan and Al-Qattan, 2015; Leonard and Dubravcik, 1970). Conservative measures may not be appropriate for treating displaced distal condylar fractures due to their inherent instability and the relatively poor remodelling potential. It is not uncommon to see patients referred with malunion, deformity and functional impairment of the digits, resulting from previous inadequate non-operative treatment (Puckett et al., 2012; Tada et al., 2010).
Studies have reported the remodelling potential of phalangeal neck fractures in young patients (typically younger than 12 years) in the sagittal plane with acceptable functional restoration in neglected cases (Cornwall and Waters, 2004; Puckett et al., 2012; Tada et al., 2010). However, remodelling potential is limited in the coronal plane and in older children. Rotational deformities and malunion resulting from intra-articular fractures do not remodel. Corrective osteotomy is indicated for adolescents where deformities induce significant scissoring of fingers, functional disability or disturbance in tendon balance (Matzon and Cornwall, 2014). Fixation techniques for the corrective osteotomy typically include K-wires or plate and screw systems (Potenza et al., 2012; Ring, 2006). However, there is limited literature regarding corrective osteotomy for distal condylar malunion of the phalanx in adolescents.
In this study, we aimed to report the outcomes of corrective osteotomy in adolescent distal condylar malunion of the proximal phalanx and to compare the use of fixation with K-wires and plates.
Methods
This retrospective study was approved by the relevant institutional review board, which waived the requirement of informed consent as it is a retrospective study. We reviewed patients between 10 to 17 years who were treated surgically for distal condylar malunion of the proximal phalanx (defined by an interval longer than 2 weeks from the initial trauma event) between January 2009 and June 2020 in a single medical centre. Patients who had multiple fractures, who had been surgically treated previously, and those with deformities caused by bone tumours were excluded. Patients with inadequate follow-up of less than 1 year were also excluded. Distal condylar malunion of the thumb was not included in this study.
The indication for surgery was deformity with greater than 15° of angulation in the coronal plane, rotational deformity, 25% translation in either the coronal or sagittal plane, or an incongruent articular gap or step-off more than 2 mm in unicondylar or bicondylar fractures. All patients presented clinically with scissoring of digits, or intolerable limited motion or stiffness after injury.
The patients were divided by the method of fixation into a K-wire group and a locking plate group. The type of fixation was chosen by the treating surgeon and not randomized. Patients must have had a closed or near-closing physis on radiographs of the injured phalanx, to be considered candidates for plate fixation.
Surgical techniques
Surgery was performed by two hand specialists with Level IV experience (Tang and Giddins, 2016) under general anaesthesia for both groups of patients.
Percutaneous osteoclasis using an intrafocal 1.0-mm K-wire was attempted for patients in early stages of healing with unmatured callus, as described by Waters et al. (2004). Open osteotomy with a mid-axial approach under pneumatic tourniquet was performed in patients with maturing hard callus or an established union. When capsulotomy was required to expose the site of malunion, the collateral ligaments were carefully identified and preserved. The direction of osteotomy was determined by the previous fracture line. In cases where fracture lines could no longer be determined, a dome osteotomy in the metaphyseal region was performed by connecting multiple K-wire drill holes with a small osteotome.
In the K-wire group, the antegrade intramedullary pinning technique was utilized to minimize tethering of soft tissues in the affected joints (Chen et al., 2019) (Figure 1). Retrograde or interfragment pin techniques were used or added to the antegrade construct in the unicondylar and bicondylar malunions, depending on the fracture pattern.
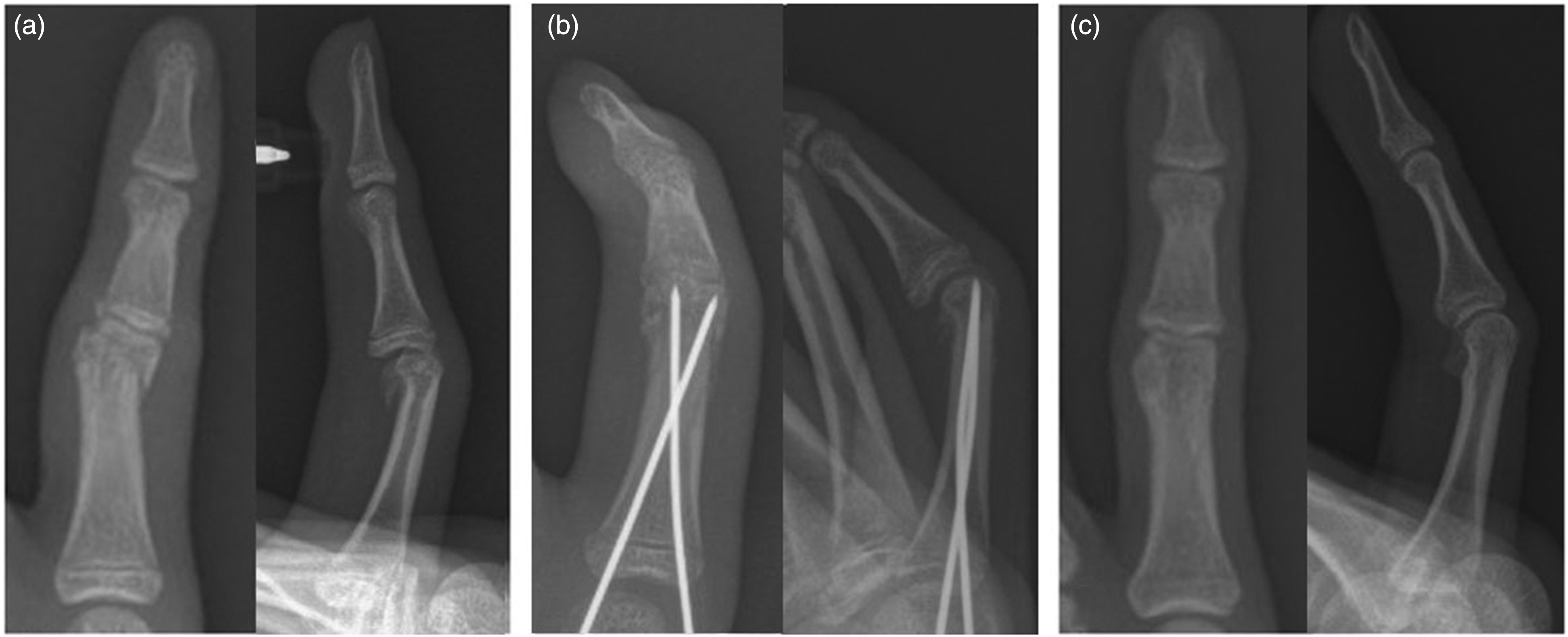
A Type IIb proximal phalangeal neck fracture in a 12-year-old boy presented 3 weeks after injury. (a) Preoperative radiographs show the fracture was in early union status, with displacement on both coronal and sagittal planes. (b) Immediate postoperative radiographs following percutaneous reduction and K-wire fixation show correction of the displacement and (c) Radiographs at follow-up 132 weeks after operation show anatomic sagittal alignment and 5° of residual coronal angulation.
In the locking plate group, the 1.7 mm VariAx Hand Plating System (Stryker GmbH; Bohnackerweg, Switzerland) or OsteoMed Hand Plating System (Osteomed Corporation, Addison, TX, USA) were used, placing the plate on the side of the main osteomized fragment (Figure 2). None of the primary procedures involved any kind of bone grafting.
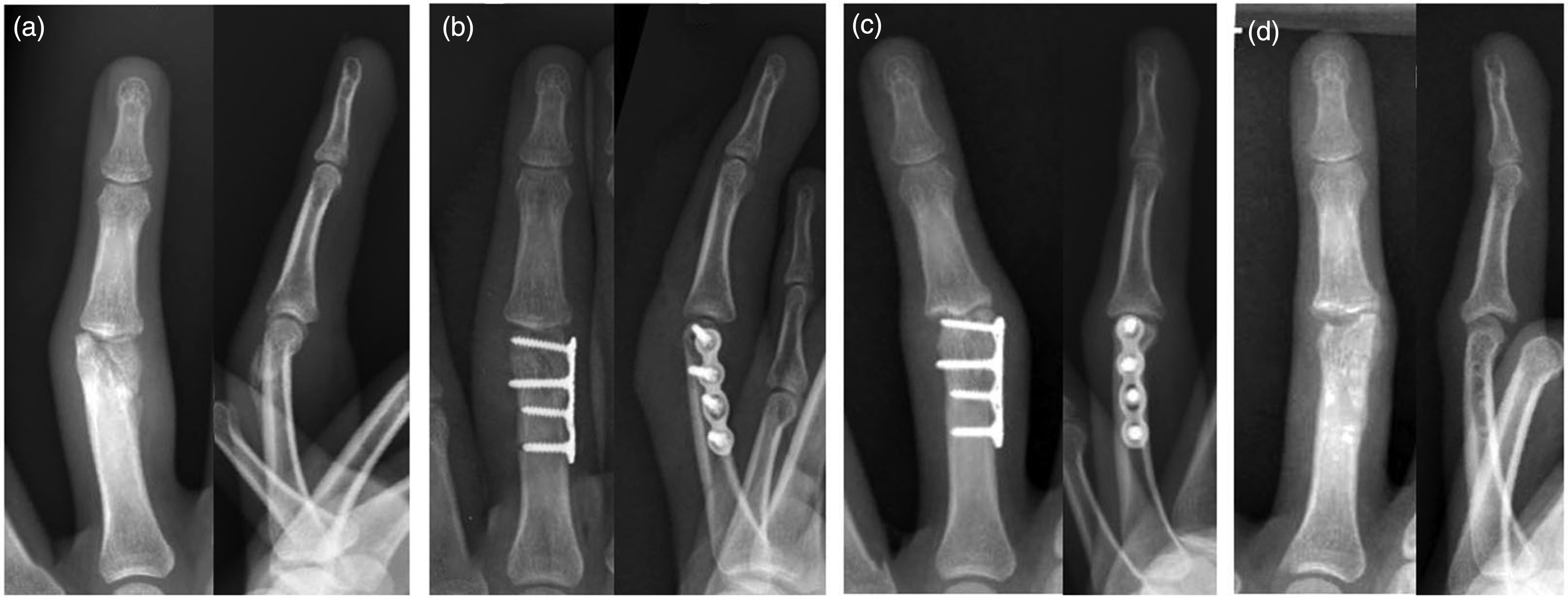
Unicondylar fracture of the proximal phalangeal head in a 15-year-old girl presented 12 weeks after the injury with limited range of movement (ROM) of the digit. (a) Preoperative radiographs indicate that the fracture healed with malalignment and a 2 mm intra-articular gap. (b) The alignment was restored after corrective osteotomy and fixation with a lateral locking plate. (c) Avascular necrosis of the opposite phalangeal condyle was noted 1 year after the surgery, causing pain and deformity and (d) After a second operation of volar plate arthroplasty and implant removal, she had a full ROM and normal hand function despite mild residual deformity, and was graded as fair on the Al-Qattan classification at final follow-up.
Postoperative care
After operation, a short arm splint was applied with the wrist in a functional position, metacarpophalangeal joints in 90° flexion, and interphalangeal joints in full extension. Immediately after the surgery, the patients with antegrade intramedullary K-wires and locked plating were encouraged to remove the splint by themselves and mobilize the fingers at least four times a day, passively through a full range of movement (ROM) of metacarpophalangeal and interphalangeal joints, followed by active ROM as tolerated.
The patients were followed-up in the outpatient clinic with radiographs taken every 2 weeks until union of the osteotomy. Union was judged radiographically with diminished gap of osteotomy, or clinically with reduced pain. The K-wires and splints were removed 4 to 6 weeks after surgery, when diminishing pain was reported along with radiographic signs of union. Subsequent follow-ups were arranged every 3 months for clinical assessments. The help of a hand therapist was rarely used.
Outcome assessment
Baseline demographics, including age, sex, trauma mechanism, delay time from injury to surgery and initial treatment, were collected from the medical records. Intra-articular phalangeal head fractures were classified as unicondylar or bicondylar, while extra-articular phalangeal neck fractures were classified using the Al-Qattan classification (Al-Qattan, 2001) (Figure 3). The operative time and time to union were recorded.
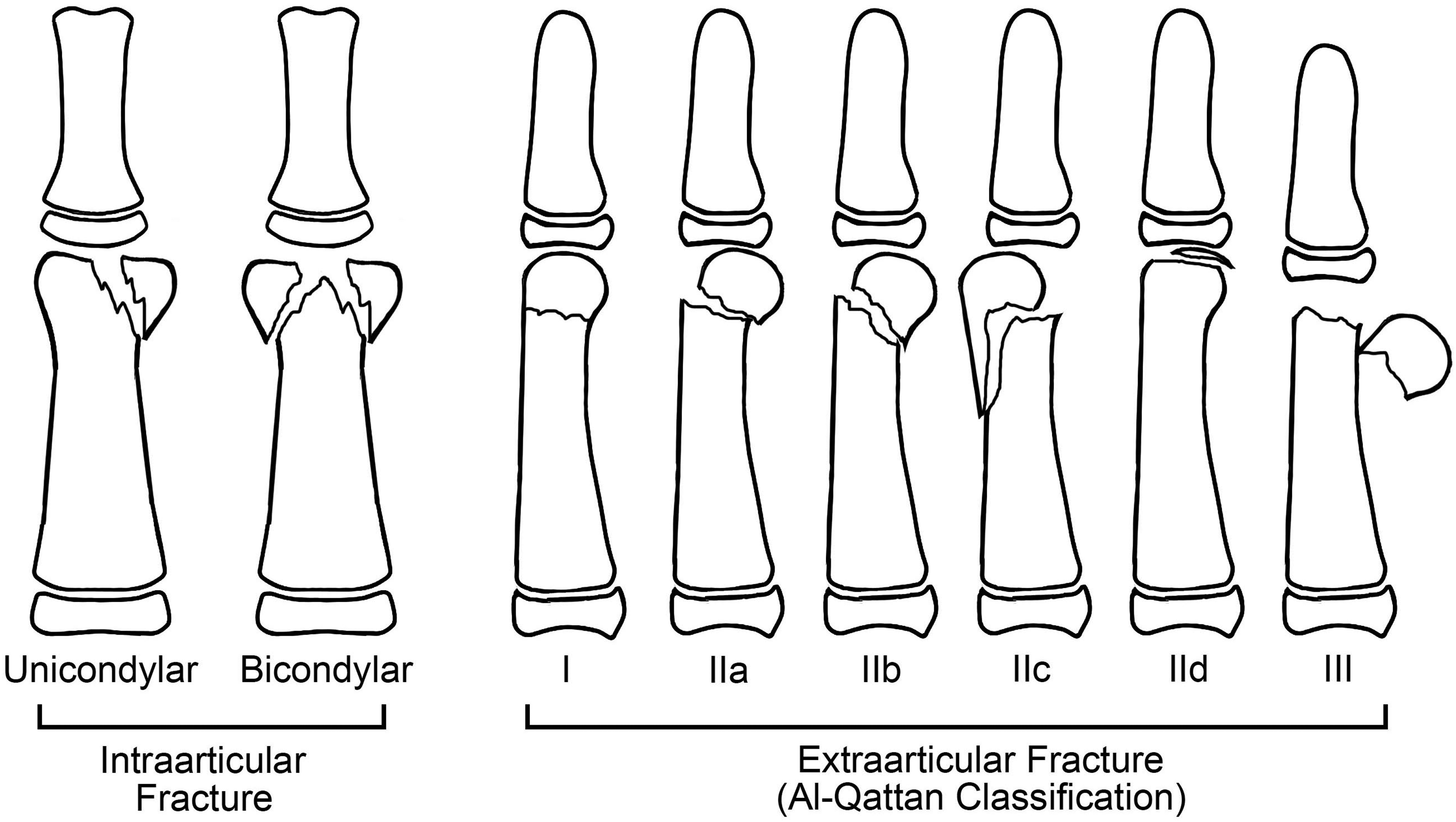
The classification of distal condylar fracture. Intra-articular fractures were classified as unicondylar or bicondylar. Extra-articular fractures were classified with the Al-Qattan classification (Al-Qattan, 2001): Type I are non-displaced fractures; Type II are displaced fractures, with bone-to-bone contact between distal and proximal fragment. The four subtypes of Type II fracture include: Type IIa, transverse fracture; Type IIb, oblique fracture; Type IIc, fractures with a dorso-lateral bony flange; Type IId, a small distal flake. Type III are displaced fractures with loss of bone-to-bone contact.
The preoperative, immediate postoperative and final radiographs were measured on the picture archiving and communication system (PACS) system. The head-shaft angulation and translation were assessed on both coronal and sagittal views (Tan et al., 2020) (Figure 4). In unicondylar fractures, parameters were measured on the displaced fragment. In bicondylar fractures, parameters were measured individually for both fragments; angulation was recorded from the more displaced fragment, while translation was recorded as the summation of both fragments. All parameters were measured by two independent orthopaedic specialists, and the mean of their measurement was recorded for each parameter.
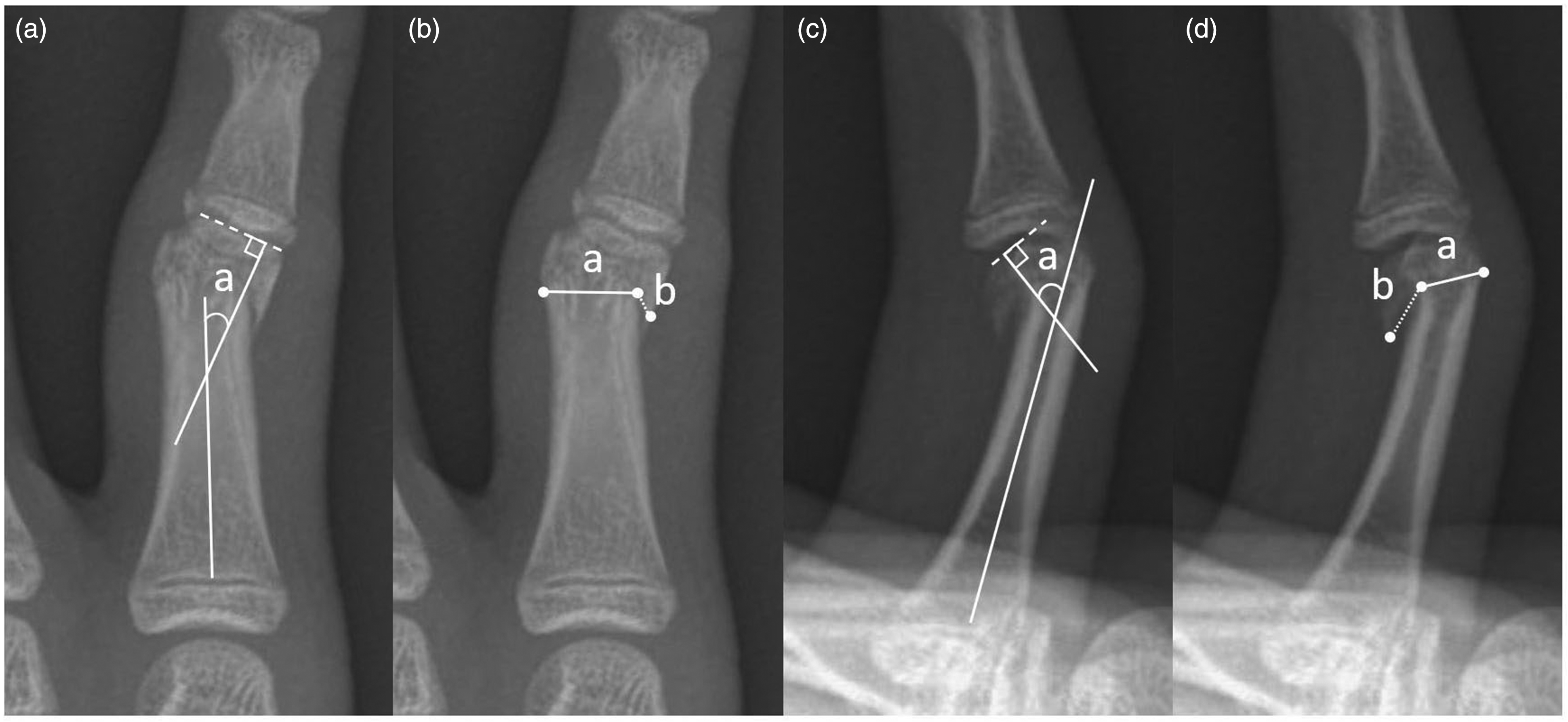
Diagrams showing the measurements of the alignment parameters on radiographs of a Type IIb phalangeal neck fracture. Angulation was measured as the angle (‘a’) between the line perpendicular to the articular surface and the centreline along the intramedullary axis; (a) coronal angulation, (c) sagittal angulation. Translation was measured as the percentage of displacement (‘b’) divided by the width of the fracture site (‘a’), namely translation = b/a × 100%; (b) coronal translation and (d) sagittal translation.
Clinical outcomes including ROM, union, residual deformity and function of the involved digit, were graded by Al-Qattan outcomes classification, and sorted into excellent, good, fair and poor results (Table 1) (Al-Qattan and Al-Qattan, 2015). Complications and causes of secondary surgery were recorded from the medical notes.
Al-Qattan outcomes classification of paediatric phalangeal neck fractures.
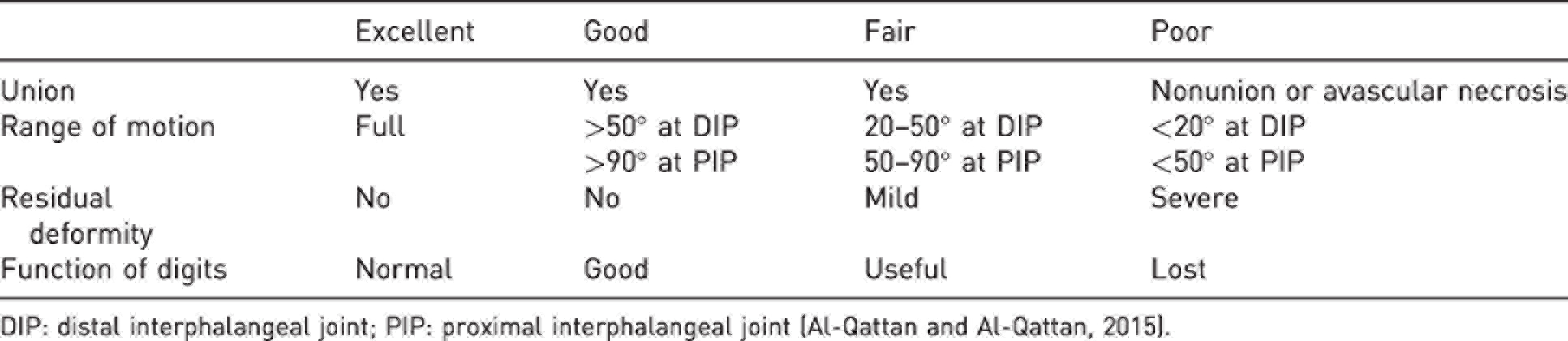
DIP: distal interphalangeal joint; PIP: proximal interphalangeal joint (Al-Qattan and Al-Qattan, 2015).
Statistics
Normality of the data was assessed using the Shapiro–Wilk test. Values are presented as median and interquartile range (IQR) if not otherwise specified. The Wilcoxon–Mann–Whitney test was used to compare numeric variables between groups, whereas the Wilcoxon signed-rank test was used to compare radiographic parameters of alignment between preoperative and postoperative radiographs, and between postoperative and final radiographs. Fisher’s exact test was used to compare categorical variables. A p-value <0.05 was considered statistically significant. The intra- and inter-observer reliabilities were verified using Cohen's kappa coefficients.
Results
Thirty-seven adolescent patients underwent corrective osteotomy for distal condylar malunion from January 2009 to December 2020. Nine patients were excluded at the outcome assessment: three patients with follow-up less than a year, three with delayed treatments due to multiple fractures, two who had had previous surgery and one with deformity caused by pathologic fracture of an enchondroma.
Twenty-eight patients with a complete dataset followed-up for more than a year were finally enrolled in the study including 20 males and eight females. The mean age was 12.8 years (range 10–17). The mean delay from initial injury was 9 weeks (range 2–52). There were eight intra-articular and 20 extra-articular fractures. Nineteen had received finger splinting in other institutes prior to our treatment. There were 19 patients in the K-wire group and nine in the locking plate group. The groups were comparable for sex, mechanism of trauma, fracture type and classification, mean delay time from injury, initial treatment and follow-up time, except for the age (Table 2), with the mean age of the K-wire fixation group being younger (11.9 years, range 10–17) than the plate fixation group (14.7 years, range 14–17; p = 0.01).
Patient demographics and fracture characteristics.
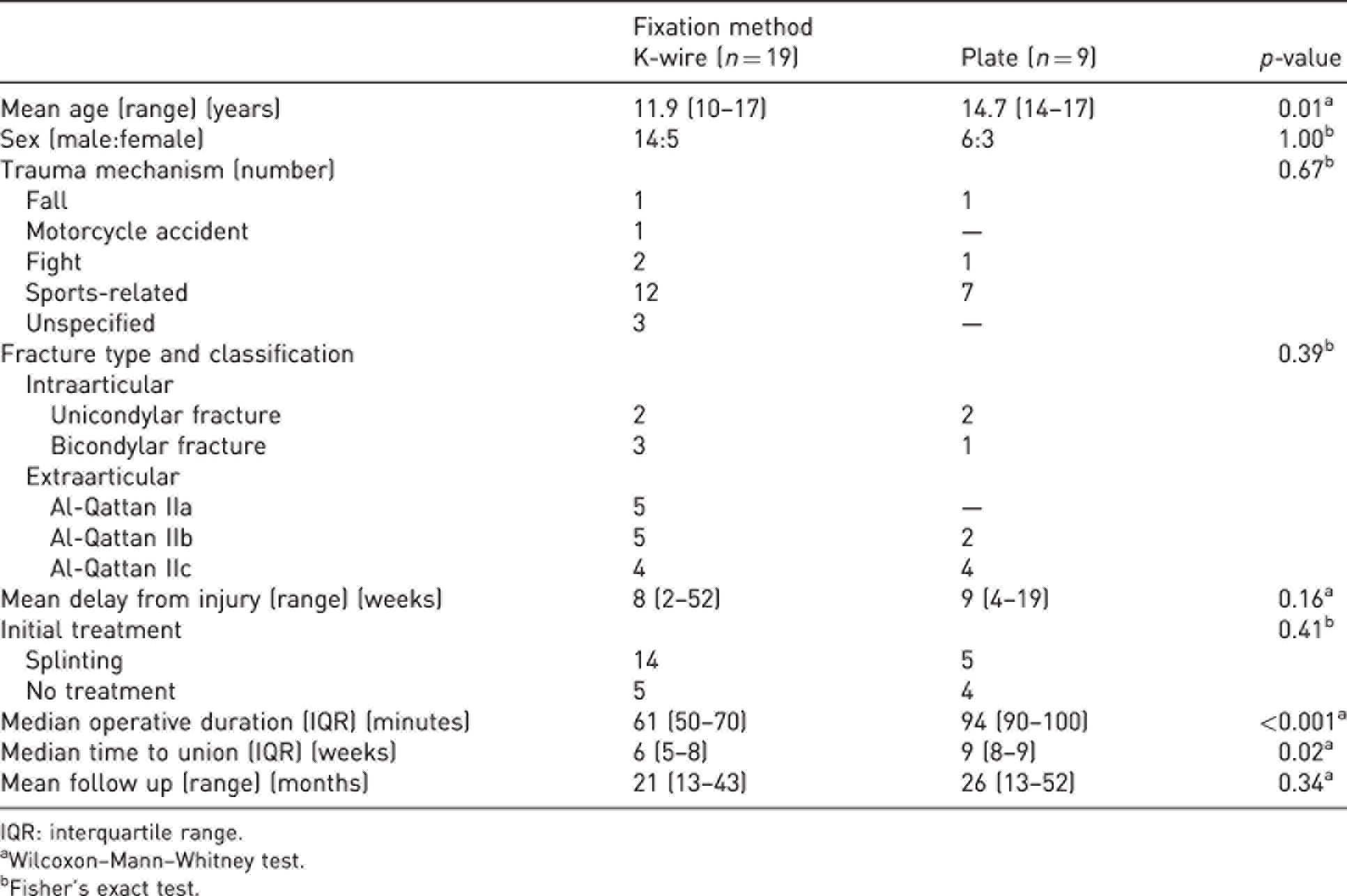
IQR: interquartile range.
aWilcoxon–Mann–Whitney test.
bFisher’s exact test.
In the K-wire group, four patients with 2 to 5 weeks of delay to surgery received percutaneous osteotomy with the Waters’ technique (Waters et al., 2004). All other patients with 4 to 52 weeks of delay underwent an open osteotomy using a mid-axial approach. Corrective dome osteotomy was performed on two patients in the K-wire group and one patient in the locking plate group, while corrective osteotomy was performed through the fracture line all other patients. Two or three wires were used in each patient in the K-wire group. The K-wire group took not only shorter operative duration (median 61 minutes, IQR 50–70; plate group, 94 minutes, IQR 90–100; p < 0.001), but also had shorter time to union (6 weeks, IQR 5–8; plate group, 9 weeks, IQR 8–9; p = 0.02).
Radiographic outcomes
Comparison of the translation and angular deformities measured on radiographs before and after operation are shown in Table 3. Good intra- and inter-observer reliabilities were demonstrated by Cohen's kappa coefficients of 0.77 and 0.68, respectively. Preoperative radiographic evaluation indicated that the deformities were similar between two groups, except for coronal translation, which was larger in the locking plate group. After the corrective osteotomy, the parameters were considerably improved in both groups, leading to no differences between treatment groups. At final follow-up, the parameters remained unchanged compared with postoperative radiographs, albeit a larger coronal angulation was found in the K-wire group (6°, IQR 4–9; plate 3°, IQR 1–4; p = 0.01).
Radiographic outcomes.
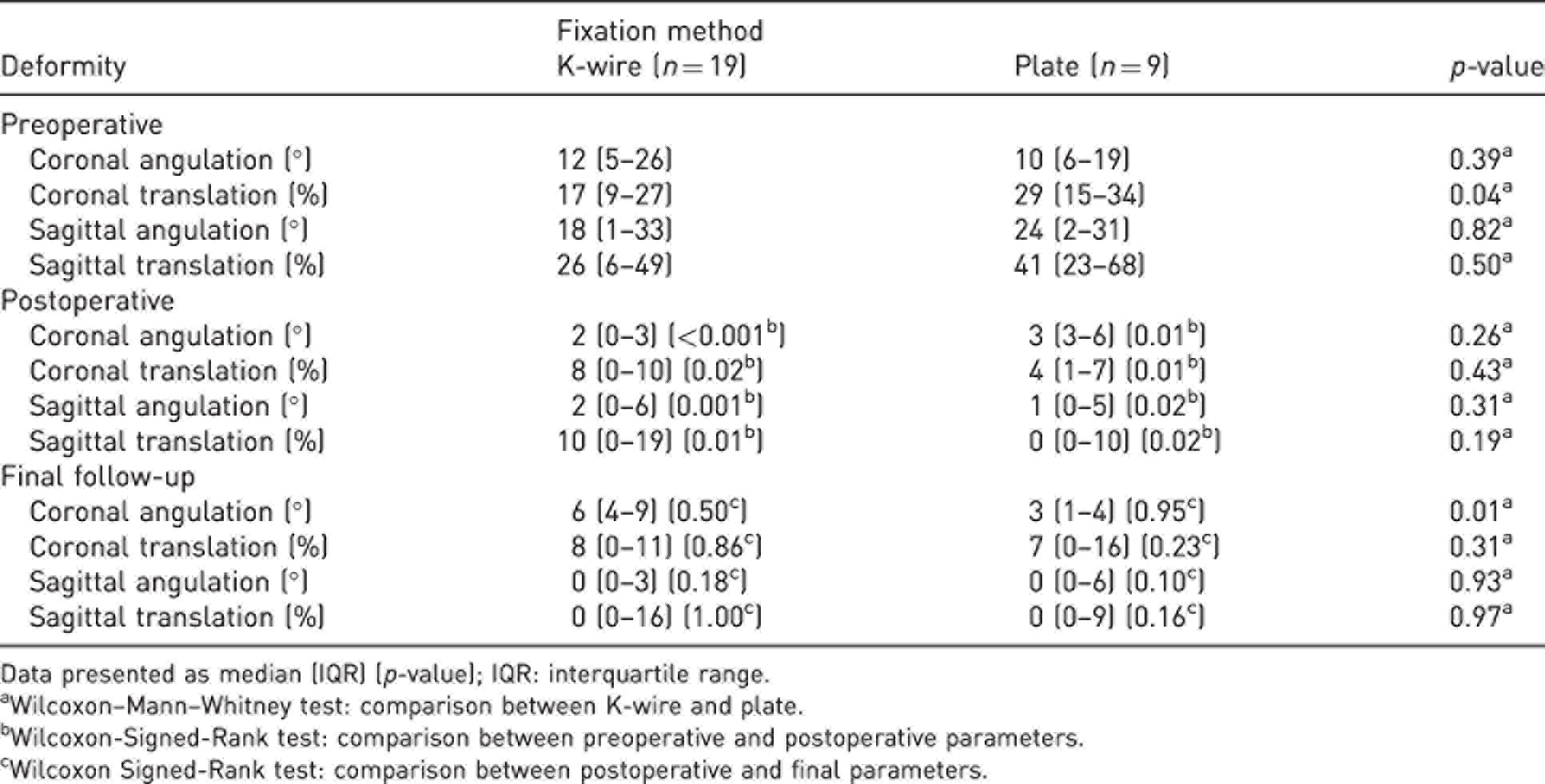
Data presented as median (IQR) (p-value); IQR: interquartile range.
aWilcoxon–Mann–Whitney test: comparison between K-wire and plate.
bWilcoxon-Signed-Rank test: comparison between preoperative and postoperative parameters.
cWilcoxon Signed-Rank test: comparison between postoperative and final parameters.
Clinical outcomes
At the final follow-up, clinical outcome for 13 patients was graded as excellent, four as good, eight as fair and three as poor, according to the Al-Qattan outcome classification (Table 4). The median ROM of involved PIP joints was 92° (IQR 77°–102°); there was no significant difference between the K-wire and locking plate group.
Clinical outcomes.
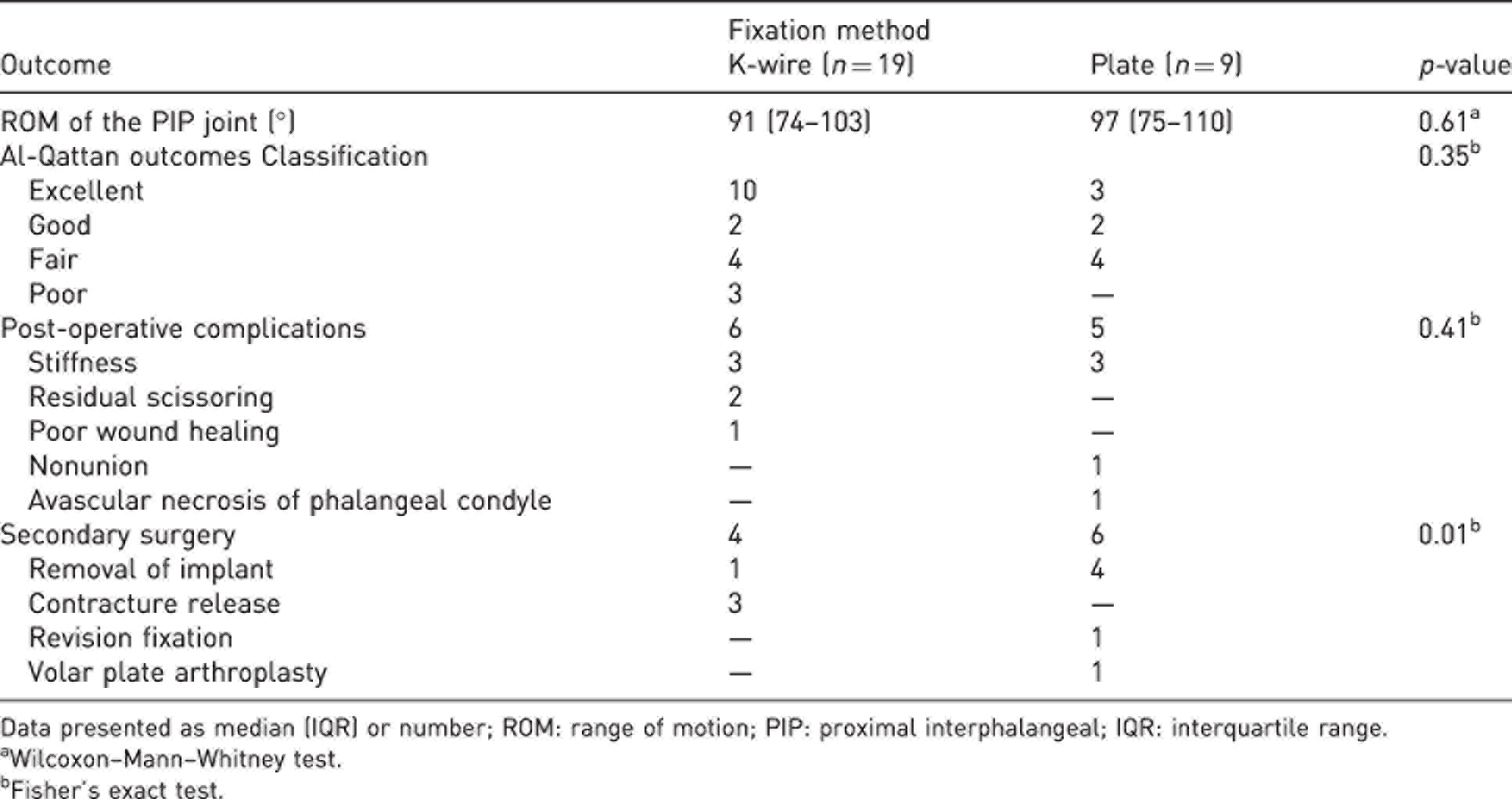
Data presented as median (IQR) or number; ROM: range of motion; PIP: proximal interphalangeal; IQR: interquartile range.
aWilcoxon–Mann–Whitney test.
bFisher’s exact test.
The rate of complications was similar between groups (6/19 versus 5/9, p = 0.41). The most common complication found in both groups was stiffness of the affected joints (Table 4). In the K-wire group, two patients had residual scissoring of digits. In the locking plate group, one patient developed nonunion requiring bone grafting and revision fixation and one patient developed avascular necrosis of a phalangeal condyle and required volar plate arthroplasty. Overall, the locking plate group had a higher rate of secondary surgery, (4/19 versus 6/9 (p = 0.01)), the majority of which being for removal of the implant (4/9).
Discussion
In this study of corrective osteotomy for adolescent distal condylar malunion, 19 patients underwent K-wire fixation and nine patients underwent plate fixation. Seventeen of the 28 patients had an excellent or good outcome, with no differences between the type of fixations. Both groups maintained the postoperative radiologic correction at the final follow-up, although a larger coronal angulation and more residual scissoring were found in the K-wire group. The K-wire group had shorter operative times and time to union, and a lower chance of requiring secondary surgery.
A few recent studies have proposed non-operative treatment alternatives for management of some cases of Type II, and even Type III fractures (Park et al., 2016; Tan et al., 2020). We do not know the exact rate of deformity progression with inadequate non-operative treatment, as our institute generally follows the principles proposed by Al-Qattan and Al-Qattan (2015).
Matzon and Cornwall (2014) reported a treatment algorithm for displaced paediatric phalangeal neck fractures with varying delays in presentation. In patients with fractures in the acute phase or early healing stages, they suggested first an attempt at closed reduction. If inadequate, the patients should undergo Waters' percutaneous reduction technique (Waters et al., 2004). Open reduction should be performed in cases where percutaneous reduction fails. In patients with healed fracture but mal-alignment and poor remodelling potential, salvage procedures such as an osteotomy should be performed. The algorithm is followed by our study. In the series of Matzon and Cornwall (2014), closed reduction succeeded in cases with delayed presentation up to 13 days, while percutaneous reductions led to 89% excellent and good outcomes on patients with delayed presentation for up to 36 days. In our study here, Waters' technique was performed in four patients with 2 to 5 weeks of delay from injury, while open osteotomy was required in 24 patients with 4 to 52 weeks delay from injury.
Regarding fixation after the corrective osteotomy, an obvious advantage of K-wire is the shorter surgical time required. On the other hand, common concerns with regard to the use of K-wires are suboptimal fixation strength, tethering of soft tissues and risks of pin track infection (Zhang et al., 2016). We utilized antegrade intramedullary pinning technique to minimize tethering of soft tissues in the affected joints (Chen et al., 2019). However, additional retrograde or interfragmentary pins should be inserted in cases where dual pin fixation is deemed inadequate to maintain stability. The K-wire group had more coronal angular displacement, although the mean difference of 3° might not be clinically important. The K-wire group also had more cases of residual scissoring of digits at final follow-up. Nevertheless, 12/19 excellent or good outcomes were achieved in patients of the K-wire group.
The advantages of locking plate systems include enhanced angular stability and better fixation strength, allowing early mobilization. Since many of the patients with distal condylar malunion initially presented with stiff joints, it is reasonable to encourage the patients to mobilize the joints as early as possible after the surgery. However, in a comparative study of K-wire and plating in the treatment of acute metacarpal and phalangeal fractures, the ROM of injured digits in the plating group were inferior 3 months after surgery, and not different after 6 months (Zhang et al., 2016). In our study, we did not demonstrate a difference in ROM of digits between groups. Unfavourable mobility of fingers after plating is often attributed to the requirement for a larger extent of tissue dissection. Although we were treating a series of delayed fractures, 24 of 28 patients required a mid-axial approach to perform osteotomy and reduction, the effect may still be prominent. Overall, a complication rate of five out of nine was recorded in the plating group, of which one avascular necrosis of phalangeal condyle and one nonunion may be attributable to the tissue dissection of plating.
The limitations of this study include its retrospective design and the small number of patients in the plating group. Consequently, the study may have been insufficiently powered to detect differences in outcomes between the groups. Second, the fixation method was chosen by the surgeon rather than by randomization. Plating was only used in adolescents whose physis were closed or near closing. Therefore, an older age was found in the plating group. Lastly, we did not analyse outcomes of using a patient-reported scoring system.
Both K-wire and plate fixation achieved a high rate of excellent or good clinical outcome in corrective osteotomy of phalangeal distal condylar malunion in adolescents. The K-wire group showed shorter operative time, faster union and a smaller chance of secondary surgery than the locking plate group.
Footnotes
Acknowledgements
The authors thank OFC Chang for editing the manuscript.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was not obtained because of the retrospective nature of this study, and therefore waived by the institutional review board.
Ethical approval
Ethical approval for this study was obtained from the institutional review board of Taipei Veteran General Hospital (IRB/REC number 2021-07-024CC).