
Abstract
This integrative review investigated reports of psychological impact and sequelae of traumatic hand injuries. A systematic search using Medline, PsychINFO, PubMed, EMBASE, CINAHL and hand-searching methods was conducted from 2008 to 2020. Nine included articles with a total of 503 participants were reported in prospective cross-sectional or longitudinal cohort studies. Depression and anxiety were common, affecting between 7% and 71% and between 23% and 71% of patients, respectively. Post-traumatic stress disorder affected between 3% and 95% of patients. Factors reported predicting psychological sequelae of hand injuries included injury severity, pain, limb dysfunction, negative perceptions of injured limbs, suboptimal coping mechanisms and limited social support. Symptoms persisted for protracted periods of follow-up but broadly attenuated after 3 months. We conclude that the high prevalence and enduring nature of psychological symptoms demonstrate an urgent need for further research to optimize treatment.
Introduction
Trauma is recognized as a physical injury that frequently requires hospitalization (Baecher et al., 2018). Hand injuries vary widely in severity and result in a range of reactions. Bates and Mason (2014) described major hand injury as a permanent alteration in the function of the hand through sudden or accidental actions. Physical effects could be accompanied by psychological impacts; the consequences of hand injury include pain (Haese, 1985; Koestler, 2010), loss of function but also frustration (Grunert et al., 1988a, 1988b, 1992), fear and anger (Hennigar et al., 2001; Ladds et al., 2017; Meyer, 2003), altered body image (Moor, 1999), anxiety, depression, and post-traumatic stress disorder (PTSD) (Gilbert, 1996; Gustafsson and Ahlström, 2004, 2006; Gustafsson et al., 2000, 2003).
PTSD, defined as the experience of one or more symptoms of avoidance, intrusive thoughts and arousal 1 month post-exposure to a traumatic event (American Psychiatric Association, 2013), affects 19% of patients with brachial plexus injury (Landers et al., 2018). An elevated risk of suicide is recognized for people suffering traumatic injury, and 17% of brachial plexus injury patients reported suicidal ideation (Landers et al., 2018). A study in the United States (US) of over 1.6 million injured participants aged 7 to 26 years found that hospitalized individuals had three times greater risk of suicide compared with the general population (Zambon et al., 2011). While the information on the psychological impacts of traumatic injury is emerging, there remain gaps in the literature for specific injury types, including hand injury. This evidence gap precludes early intervention and potential prevention of negative outcomes, including suicide, for people following a hand injury. Therefore, it is essential to identify the characteristics and degree of psychological harm attributable to a hand injury and to identify those at risk. It is important to bear in mind that individuals may experience the impact of trauma differently and may vary in their response and management. Therefore, treatment needs to be individually tailored.
The following research questions were posed.
Which psychological sequelae can accompany a hand injury? At what time points in relation to the original trauma/surgery do psychological sequelae occur? Which factors have been reported to influence the psychological sequelae development, type and intensity?
Methods
We performed an integrative review to facilitate the combination of evidence from various sources and different methodologies (Whittemore and Knafl, 2005). The preferred reporting items for systematic reviews and meta-analyses (PRISMA) group recommendations were followed. We systematically searched Medline, PsychINFO, PubMed, EMBASE and CINAHL databases. Additionally, reference lists of relevant studies were checked, and a hand search of key journals tracked relevant citations. Inclusion and exclusion criteria are shown in Online Table S1 and terms used to identify the search strategy components in Online Table S2.
After removing duplicates, 4329 articles remained and were screened by title and abstract for relevance. Following the exclusion of ineligible articles, the remaining articles were accessed and read in full, resulting in the exclusion of a further nine articles that did not meet eligibility criteria. These excluded articles focused on disability, injuries proximal to the elbow, assessment or were systematic/literature reviews. The PRISMA search and screen process is summarized in Figure 1.
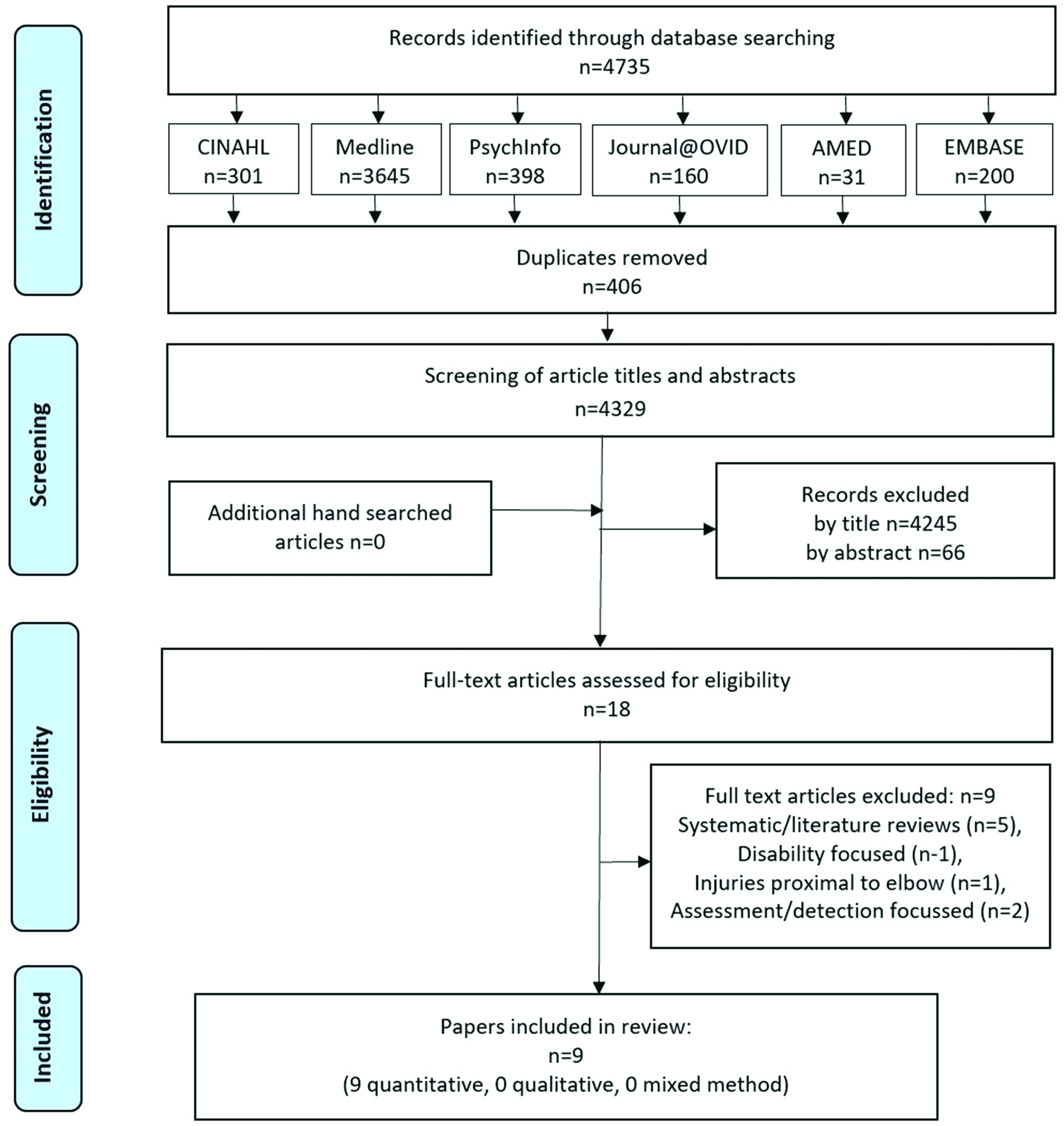
Preferred reporting items for systematic reviews and meta-analyses.
The remaining nine articles were then appraised using the design-specific appraisal tool for cohort studies of the Critical Appraisal Skills Programme (Critical Appraisal Skills Programme, 2017). Each author appraised these articles separately. Findings were compared, discussed and agreed upon, and all nine articles were retained.
Data were then extracted, collated and tabulated by year of publication, country of origin, study design, sample size, characteristics and details of injury (Online Table S3). Tools used to assess psychological symptoms, quality of life, social support and hand function were extracted (Online Table S3). In response to each of the three research questions, findings from each article were extracted and tabulated (Table 1).
Data extracted from included articles in response to research questions.
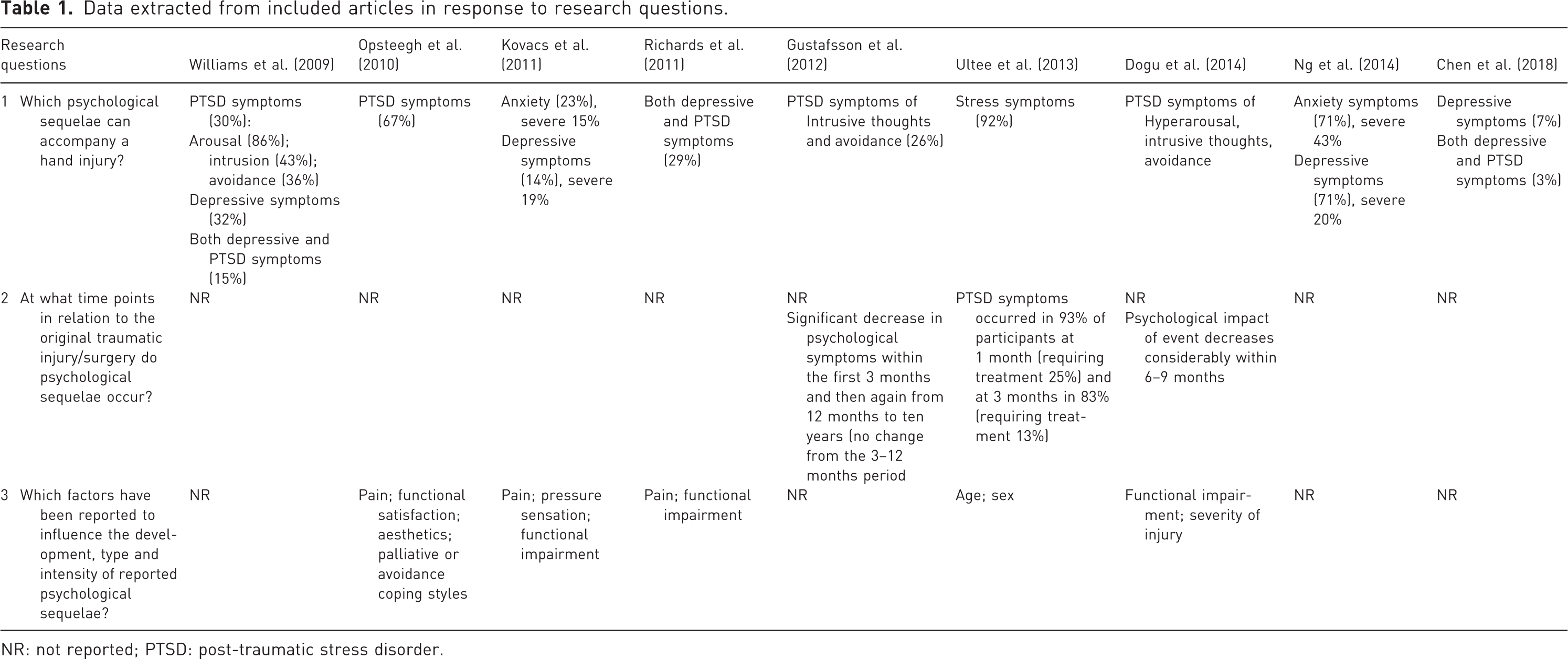
NR: not reported; PTSD: post-traumatic stress disorder.
A narrative synthesis approach was adopted for analysis as it allows data from different research designs to be systematically examined and integrated, enabling conclusions to be drawn through descriptive narration (Ryan, 2013).
Results
All nine included articles were prospective quantitative studies from the northern hemisphere with cross-sectional (n = 6) (Chen et al., 2018; Kovacs et al., 2011; Ng et al., 2014; Opsteegh et al., 2010; Richards et al., 2011; Williams et al., 2009) and longitudinal cohort study designs (n = 3) (Dogu et al., 2014; Gustafsson et al., 2012; Ultee et al., 2013). Four studies recruited participants by retrospective assessment of patients' medical notes (Chen et al., 2018; Kovacs et al., 2011; Ng et al., 2014; Opsteegh et al., 2010). Three other studies recruited participants consecutively on entering the research facility (Dogu et al., 2014; Gustafsson et al., 2012; Ultee et al., 2013). Richards et al. (2011) did not explain the recruitment of their cohort, and Williams et al. (2009) enrolled patients seeking follow-up post-treatment without stating whether this was routine follow-up or requested due to ongoing problems. Kovacs et al. (2011) recruited participants based on a Hand Injury Severity Score greater than 50. Participant demographics and injury analysis in the nine included articles showed participants were predominantly male, early to middle-aged, with mainly occupational injuries of various severity, types and locations occurring distal to the elbow. These injuries caused pain that affected the lives of patients and impacted their functional abilities (Online Table S3).
Follow-up time frames for the five cross-sectional studies ranged from 1 month (Williams et al., 2009) to 27 years (Kovacs et al., 2011) post-injury. The three longitudinal studies reported different follow-up time intervals: one used four follow-up time points (at 1 week, 3 months, 12 months and 10 years) (Gustafsson et al., 2012); two articles, Dogu et al. (2014) and Ultee et al. (2013) reported two data collection time points (at 1 and 3 months; at 7 and 35 weeks, respectively).
All studies surveyed participants using subjective tools, with Ng et al. (2014) and Chen et al. (2018) also collecting objective functional data through grip strength, key pinch and 2-point discrimination tests. Additionally, Chen et al. (2018) included active range of motion, cold intolerance and Semmes–Weinstein monofilament objective testing. Instruments assessed hand function and disability, PTSD, depression, anxiety, stress reactions, coping reactions, quality of life, social support, body image and general health (Online Table S3). Comparisons among study findings were challenging, and meta-analysis was impossible. Findings were therefore analysed to create a narrative synthesis.
Types of psychological sequelae in hand injuries
For our first research question, we found relevant data in nine articles, with participants experiencing symptoms related to depression (five articles), PTSD (six articles), anxiety (two articles) and stress (one article). Only one article referred to specific symptoms (intrusive thoughts and avoidance) (Gustafsson et al., 2012). Results are summarized in Tables 1 and 2.
Psychological sequelae reported following traumatic hand injury (research question 1).
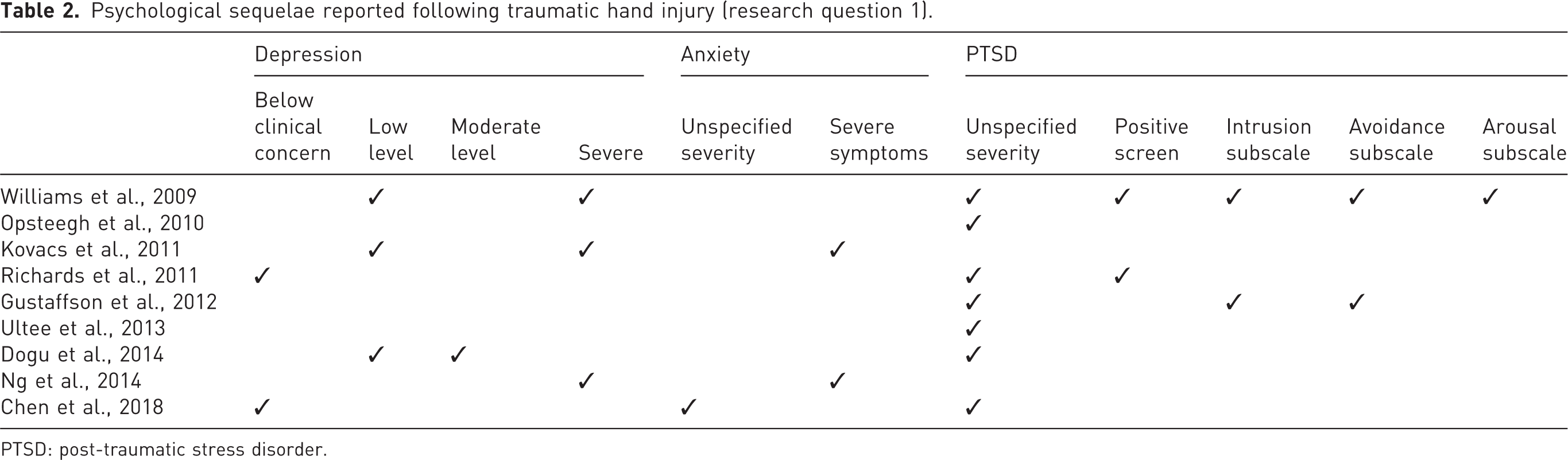
PTSD: post-traumatic stress disorder.
Depression was reported in six articles using three different scales (Online Table S3). In two articles, it was described as below clinical concern (Chen et al., 2018; Richards et al., 2011), and three articles reported that most participants' depressive symptoms were low level (Dogu et al., 2014; Kovacs et al., 2011; Williams et al., 2009). Five articles reported participants with some depressive symptoms. Dogu et al. (2014) assessed depression at two time points and revealed 41% of participants were symptomatic in the acute stage, but this subsequently reduced to 15%. Of the participants who reported depressive symptoms, 19% (Kovacs et al., 2011), 32% (Williams et al., 2009) and 20% (Ng et al., 2014) were reported to experience this within the severe range.
PTSD scores were reported in six articles using five different tools (Online Table S3). Overall, 30% of participants screened positive for PTSD (Richards et al., 2011; Williams et al., 2009). The median number of PTSD symptoms reported was one, with more PTSD symptoms reported in the presence of pain (Opsteegh et al., 2010).
Anxiety was reported in three articles using two scales (Online Table S3). Kovacs et al. (2011) reported 23% of participants with symptoms of anxiety, whereas Ng et al. (2014) reported that 71% of participants were affected. Severe symptoms were reported for 15% of participants (Kovacs et al., 2011) and (following amputation injuries) by 43% (Ng et al., 2014). Overall, findings revealed that psychological sequelae were common among patients experiencing diverse hand injuries (mild to major).
Time points for psychological sequelae in relation to the original trauma or surgery
Our second research question explored the time when psychological symptoms were first experienced. None of the articles provided this information, but prevalence rates at various time points were supplied. Ultee et al. (2013) reported that 93% of participants experienced stress symptoms at 1 month and 83% 3 months post-injury. Gustafsson et al. (2012) said that 24% of participants experienced psychological symptoms 1 week post-injury and decreased to 8% at 3 months. No further decrease was reported between the 3-month and 1-year assessments. However, symptoms improved between the 1- and 10-year data collection points, with the remaining 8% and 2% of patients, respectively, affected.
Factors influencing the development, type and intensity of psychological sequelae
Four articles reported that the degree of hand functional loss impacted the extent of psychological symptomatology (Chen et al., 2018; Dogu et al., 2014; Opsteegh et al., 2010; Richards et al., 2011). Two studies reported positive correlations between functional disability with anxiety and depression (Kovacs et al., 2011; Ng et al., 2014). Both functional impairment and pain correlated significantly with perceived stress (both p < 0.01) (Richards et al., 2011).
The passage of time was another important influence, with anxiety and PTSD symptoms subsiding after injury (Dogu et al., 2014; Gustafsson et al., 2012; Kovacs et al., 2011; Ng et al., 2014; Ultee et al., 2013). Similarly, Impact of the Event Scale scores were reduced by half between the initial and the second assessment at 3 months (Gustafsson et al., 2012; Ultee et al., 2013), and Gustafsson et al. (2012) reported this change as significant (p = 0.024). However, for Dogu et al. (2014), this level of reduction did not occur until 28 weeks post-injury.
Other influences identified included life changes such as ongoing pain experiences (Kovacs et al., 2011; Williams et al., 2009) and reduced social functioning (Williams et al., 2009). One article examined body image (Kovacs et al., 2011) using two tools (Online Table S3). Major changes in employment, marked decreases in income, persistent pain and increased pressure sensation were all associated with the highest Body Dysmorphic Disorder Examination – Self-report questionnaire scores (Kovacs et al., 2011). Further, increasing pain frequency, cold intolerance and dissatisfaction with work correlated with lower levels of perceived attractiveness and self-confidence; pressure sensation changes and lower incomes following hand injuries correlated with lower satisfaction with life (Kovacs et al., 2011).
Discussion
The findings of this systematic review reveal the dearth of data on this topic. However, included studies, sampling across different hand-injured patient groups assessed at various points post-injury demonstrated that the common mental disorders were frequently reported among these patients. We found high rates of anxiety, depression and PTSD symptoms of intrusive thoughts, avoidance and hyper-arousal experiences. In patients with hand injuries, depression was reported to affect between 7% and 71%; anxiety, between 23% and 71%; and PTSD, between 3% and 95%. Comparatively, in an Australian study of mental health sequelae of any form of trauma, the prevalence of depression was reported to be 16%, anxiety disorder (11%) and PTSD (10%); in total, 31% of injured patients had encountered a psychiatric diagnosis within the first 12 months post-injury (Bryant et al., 2010).
The timeframe in which psychological sequelae were reported in the included studies ranged from 1 week to 12 months post-injury. While symptoms decreased over time, and markedly so within the initial 3 months post-injury, suffering in some patients remained prevalent and enduring. In their study of traumatic pelvic injuries, McMinn et al. (2020) also reported that psychological symptoms of PTSD and depression decreased over time. In these patients (with non-hand-related injuries) only those with a pre-injury diagnosis of PTSD reported ongoing symptoms at 12 months.
Factors reported to predict the development, type and intensity of reported psychological sequelae of traumatic hand injury included injury severity, pain, pressure sensations, limb dysfunction, limb appearance, suboptimal coping mechanisms and limited social support. In addition, pain correlated positively with symptoms of depression, anxiety and PTSD (Kovacs et al., 2011; Opsteegh et al., 2010; Richards et al., 2011; Williams et al., 2009) and with higher numbers of PTSD symptoms (Opsteegh et al., 2010; Williams et al., 2009). However, such analyses did not distinguish whether, for example, depressed patients reported more pain or patients in pain suffered greater depression. In the broader traumatic injury literature (including orthopaedic trauma and brain injuries), the presence of pain is reported to be a major influence in injury recovery and has a direct relationship with psychiatric disorders (Bryant, 2011). Similarly, Adiyeke et al. (2019) studied fifth metacarpal neck fractures and reported that pain intensity and decreased range of motion were affected by psychological factors in participants with chronic pain. Moreover, in the literature relating to traumatic injuries of other body parts, pain plays a contributory role to depression and PTSD (McMinn et al., 2020).
The patient sex was also reported as a predictive factor; Ultee et al. (2013) reported that women are at greater risk of early post-traumatic psychological stress. Similarly, a systematic review and meta-analysis of the prevalence of PTSD and depression following acute orthopaedic trauma reported that women were four times more likely to experience PTSD than men and one-third more likely to experience depression (Muscatelli et al., 2017).
Other potential factors included injury severity and loss of hand function. The greater incidence and severity of psychological symptoms (anxiety, depression) reported by Ng et al. (2014) could be attributed to the more severe type of injury reported (amputations). Three articles linked the degree of functional loss to the extent of psychological symptomatology (Dogu et al., 2014; Opsteegh et al., 2010; Richards et al., 2011).
Symptoms tended to occur in clusters (dependent on what was sought in each study), with positive correlations reported between PTSD and depression (Chen et al., 2018; Richards et al., 2011; Williams et al., 2009); between PTSD and body pain, role emotion, social function and mental health (Williams et al., 2009); with higher numbers of PTSD symptoms reported with pain and palliative or avoidant coping styles (Opsteegh et al., 2010). Similarly, an integrative literature review of mental health following traumatic physical injury supported the finding of symptom clusters and suggested that psychological symptoms of depression, PTSD and anxiety were associated with decreased coping strategies, poorer quality of life and prolonged recovery times (Wiseman et al., 2013).
This review has some limitations. First, the small number, variable quality and methods used by included studies precluded firm general conclusions. Second, there is no representation of the patients' experiences and voices. The perspective of those injured, expressed through their own words, does not feature in this literature. Their experiences are solely reported through objective assessment tools that reduce individual and unique histories to standardized ratings.
Overall, the review identified psychological sequelae as ubiquitous across this patient population and care trajectory. These findings have implications for hand surgeons and the interdisciplinary team in providing early intervention for better psychological care for these patients, including access to psychological support and patient education. Treatment models should direct and enable staff to provide psychological support to traumatically hand-injured persons to optimize recovery. Awareness of prolonged psychological sequelae following traumatic hand injury has an essential bearing on medico-legal personal injury claims and should be considered. Given the heterogeneous, often small scale and selective nature of current studies, further research is needed to explore the clustered nature of symptom complexes suggested by findings to date. Local information needs to be collected to support identifying and initiating context-appropriate treatment of those at risk of psychological harm following hand injuries.
Supplemental Material
sj-pdf-1-jhs-10.1177_17531934221117429 - Supplemental material for Psychological sequelae of hand injuries: an integrative review
Supplemental material, sj-pdf-1-jhs-10.1177_17531934221117429 for Psychological sequelae of hand injuries: an integrative review by Kay Maddison, Lin Perry and Deborah Debono in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-2-jhs-10.1177_17531934221117429 - Supplemental material for Psychological sequelae of hand injuries: an integrative review
Supplemental material, sj-pdf-2-jhs-10.1177_17531934221117429 for Psychological sequelae of hand injuries: an integrative review by Kay Maddison, Lin Perry and Deborah Debono in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-3-jhs-10.1177_17531934221117429 - Supplemental material for Psychological sequelae of hand injuries: an integrative review
Supplemental material, sj-pdf-3-jhs-10.1177_17531934221117429 for Psychological sequelae of hand injuries: an integrative review by Kay Maddison, Lin Perry and Deborah Debono in Journal of Hand Surgery (European Volume)
Footnotes
Acknowledgements
We would like to thank the Hand Surgeons from the Hand Unit at Sydney Hospital for their advice and continual support with this article.
Conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article. The corresponding author is a current recipient of an Australian Government Research Training Program scholarship to support doctoral studies.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.