
Abstract
The purpose of this study was to compare strength, bulk and time of repair of human cadaveric flexor digitorum profundus tendons repaired in situ versus ex situ. Ninety-six human cadaveric flexor digitorum profundus tendons were transected 5 mm distal to the A2-pulley and randomized to 2-strand, 4-strand or 6-strand repairs. We found no significant differences in repair strength between in situ and ex situ repairs, but repair strength increased with increasing number of strands. The cross-sectional area of the repair was not significantly related to the number of strands, but 4- and 6-strand in situ repairs were bulkier than ex situ repairs. In situ repair took longer, and repair time increased with increasing number of strands. We suggest that cadaveric studies of flexor tendon repair should be performed in situ in order to better mimic the clinical reality of tissue handling and repair bulkiness.
Introduction
Many different techniques have been described to repair flexor tendons, varying mainly in the complexity of suture configuration. Most of these studies focus only on biomechanical strength and examine repair techniques performed after tendon extraction (ex situ) (Calfee et al., 2015; Chen et al., 2014; Marrero-Amadeo et al., 2011; Tran et al., 2002; Vanhees et al., 2013; Zhao et al., 2004) and with non-human specimens (Al-Qattan et al., 2013; Kozono et al., 2018; Lawrence et al., 2005; Manchio et al., 2009; Savage, 1985; Tang et al., 2005; Wong and Tay, 2018; Wu and Tang, 2014). In situ tendon repair is more technically difficult, since tendon handling and suture placement must be performed within the tendon sheath. This makes accurate placement of core sutures difficult, which may affect the strength and bulk of the repair site. Moreover, a complex suture configuration has limited applicability in clinical practice if it requires an excessive amount of time. Consequently, biomechanical data derived from ex situ repairs may not be applicable to real-life treatment of the patient with a flexor tendon injury.
The purpose of this investigation was to compare cadaveric human flexor tendons repaired in situ and ex situ, with repairs of increasing complexity and with 2-, 4- or 6-strand repairs. The following hypotheses were tested: (1) repairs performed in situ will be weaker than the same repairs performed ex situ; (2) repairs performed in situ will be bulkier than the same repairs performed ex situ; and (3) more complex suture configurations take more time to perform, implying more tendon handling.
Materials and methods
Specimens
Twelve matched pairs of fresh frozen cadaveric hands were used, providing 96 flexor digitorum profundus (FDP) tendons. Thumb flexors were not used. Donor demographics are shown in Table 1. A priori power analysis indicated that 12 pairs of 2-strand repairs, and 11 pairs of both 4- and 6-strand repairs were necessary to detect a 25% difference in force at failure between in situ and ex situ repairs with 80% power. Block randomization was used to assign tendons to 2-strand, 4-strand and 6-strand repairs, with equal numbers of index, long, ring and small fingers in each group. Half of the repairs in each group were performed in situ. For the contralateral matched digit, the repair was performed on the lab bench after the tendon harvest (ex situ). Within each group, equal numbers of in situ and ex situ tendons were randomized to right- versus left-handed tendons. The order of in situ and ex situ repairs was alternated.
Demographics of donors.
aThese data are expressed in mean (SD, range).
bThese data are numbers.
Repairs
Through a Bruner incision, tendons were exposed by incising the sheath between the A2 and A4 pulleys. A complete, transverse laceration was made in the FDP tendon 5 mm distal to the A2 pulley using a #15 scalpel. To improve tendon exposure for in situ repair the distal 5 mm of the A2 pulley was vented, consistent with common clinical practice. Tendon width and thickness were measured by the same investigator with electronic callipers at the injury site, producing on average three separate measurements. The cross-sectional area (CSA) was calculated, assuming an ellipsoid tendon shape (π × width/2 × thickness/2). Tendons randomized to the in situ group were repaired through existing exposure (Figure 1). Tendons in the ex situ group were harvested from the finger and immediately repaired by clamping the proximal and distal ends of the tendon to alligator clips affixed to the lab bench (Figure 2). The 2-strand locking Kessler, 4-strand locking cruciate and 6-strand cross-stitch Savage repairs were used (Figure 3). These repair types were chosen because of their prevalence in peer-reviewed literature and their use of a single (not looped) suture with a single knot made within the repair site. The core suture was 3-0 braided polyester suture (Ethibond, Johnson and Johnson Medical Technologies, Piscataway, NJ, USA) and was placed to exit the tendon 10–12 mm from the cut surface. A running epitendinous stitch of 6-0 nylon (Ethilon, Johnson and Johnson Medical Technologies, Piscataway, NJ, USA) was then placed. All repairs were performed under loupe magnification by the same investigator (CL). All repairs were timed from the initiation of core suturing until the completion of the epitendinous stitch. In situ specimens were harvested from the digit after tendon repair was complete. Post-repair, all specimens were then remeasured for width and thickness at the repair, and the CSA was calculated. Specimens were frozen until mechanical testing.
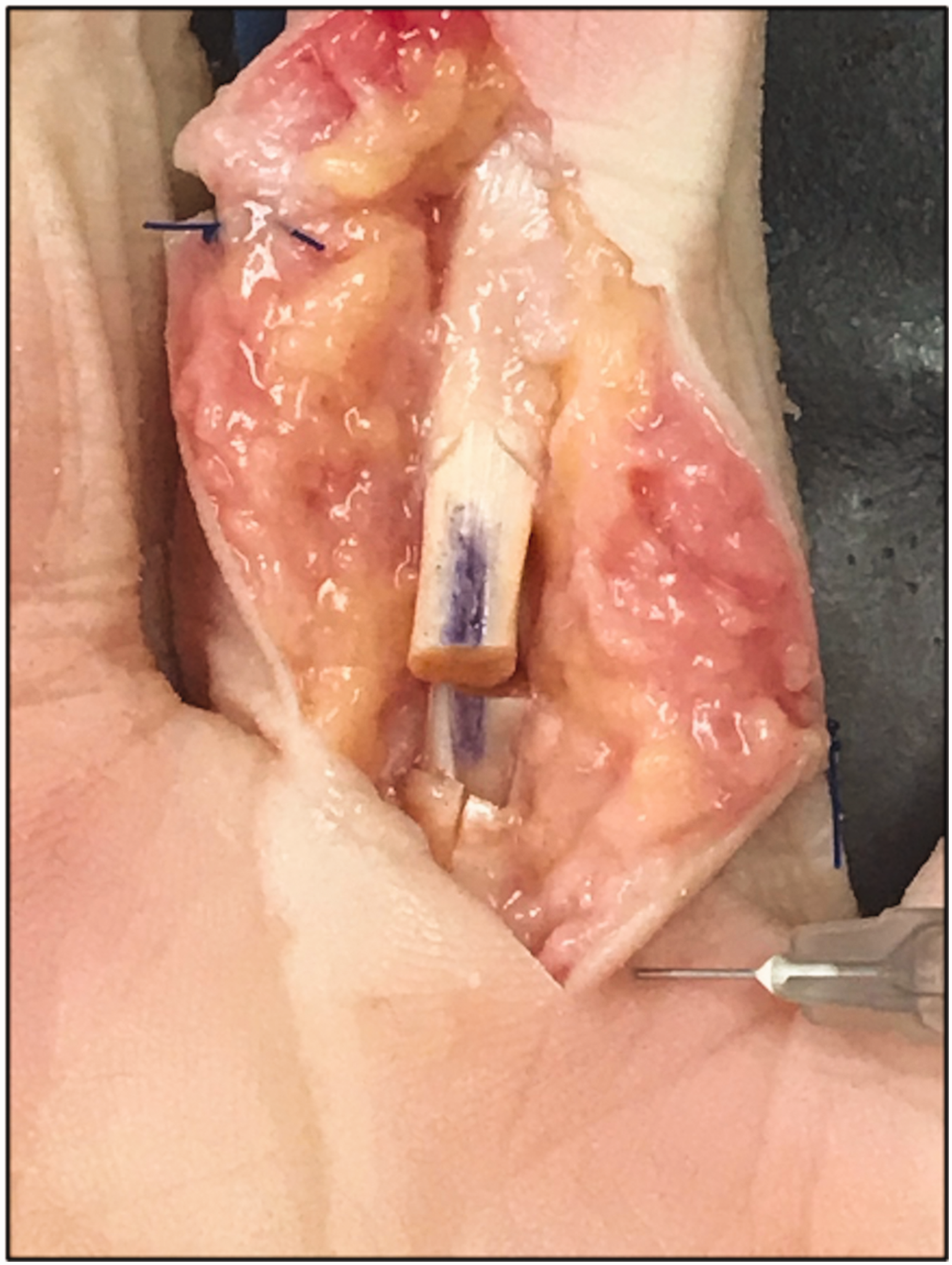
Example of in situ repair setup. The 5 mm vent in the A2 pulley can be seen in the proximal end of the wound.
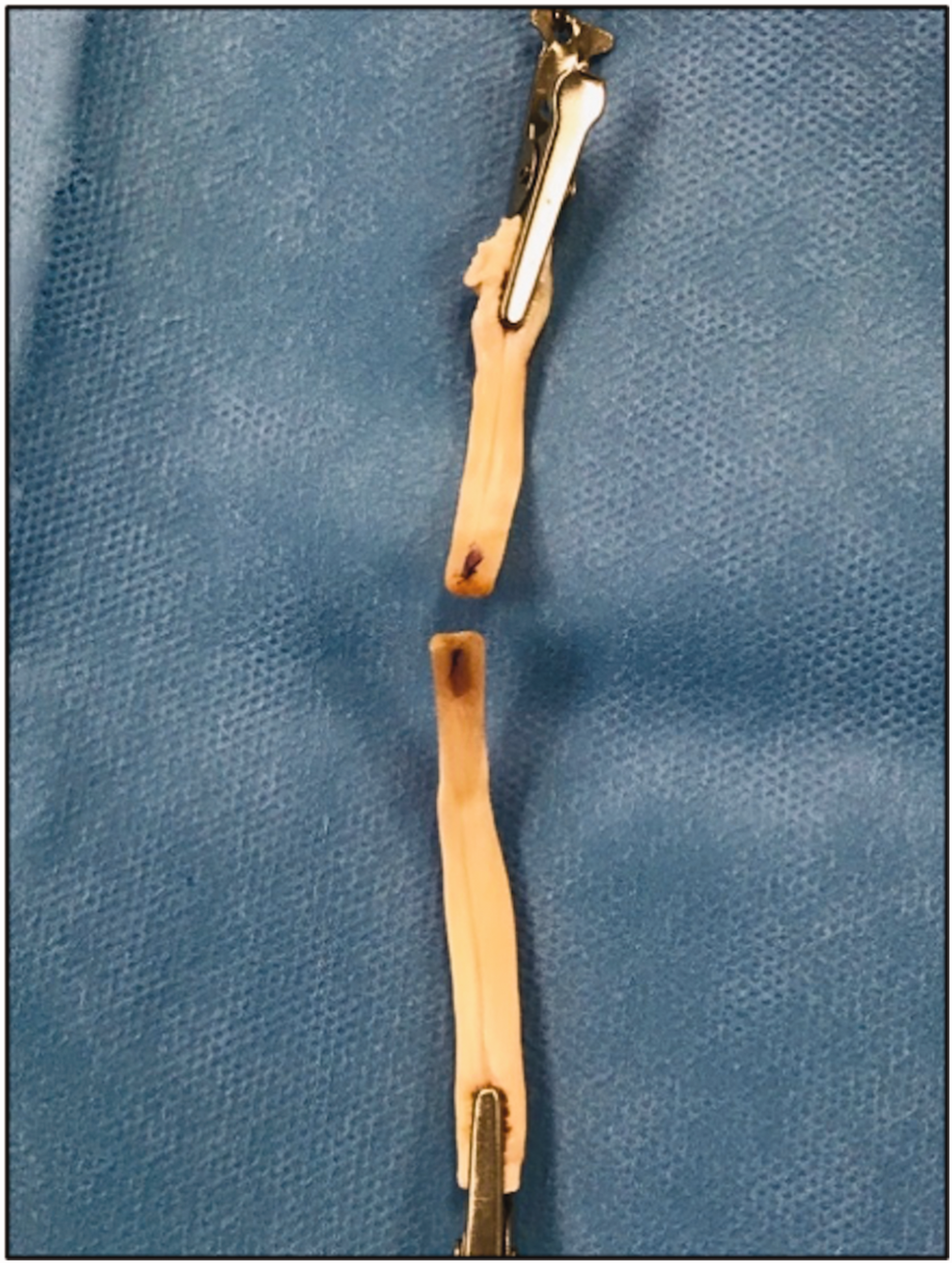
Example of ex situ repair setup with tendon secured distally and proximally with alligator clips.

Repairs performed included: (a) 2-strand locking Kessler, (b) 4-strand cruciate and (c) 6-strand Savage repair.
Testing
After thawing to room temperature, tendons were mounted on custom-made tendon clamps (Figure 4). Tendon repair strength (tension, measured in Newtons (N)) was determined using an MTS 858 Bionix II testing platform (MTS Systems, Eden Prairie, MN, USA). Tendons were pre-loaded to 2 N and axially displaced at 20 mm/min. Force at ultimate failure was recorded. Video footage was recorded at 30 frames per second, and both force at initial gap and force at 2 mm gap was determined by post-hoc analysis of video taken during repairs, with measurements taken by three independent observers in a blinded fashion.
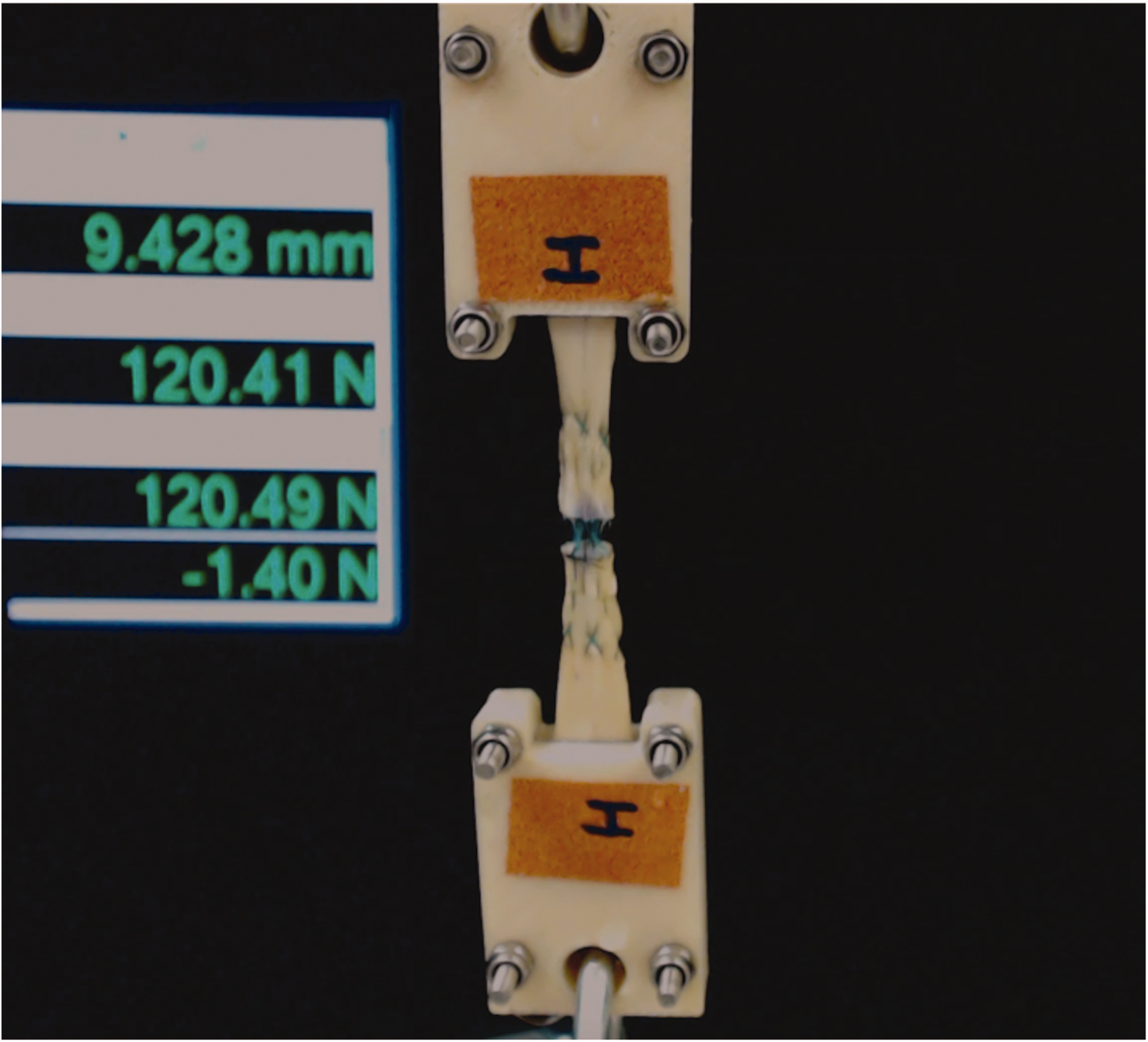
Characteristic tendon mounted on custom-made clamps during axial tension testing. Force and displacement can be seen to the left, as well as 2 mm reference marks on the tendon clamps, for videographic measurement of tendon gapping.
Statistical methods
Repeated measures analysis of variance was used to compare mean force at failure and the pre- to post-repair percentage change in CSA within and between repair groups. The mean time to complete the repairs was similarly analysed. Because multiple pairwise comparisons between groups can increase the potential for a Type I error, we adjusted p-values using the Tukey method. To evaluate the effect of tendon size on bulk of repair, we separately analysed the small and long finger repairs, using paired t-tests to compare in situ versus ex situ mean percentage change in CSA. The intra-class correlation coefficient (ICC 2,1) was used to describe the inter-rater reliability for video measurements of force at initial gap as well as force at 2 mm gap. A p-value <0.05 was considered statistically significant.
Results
Repair strength
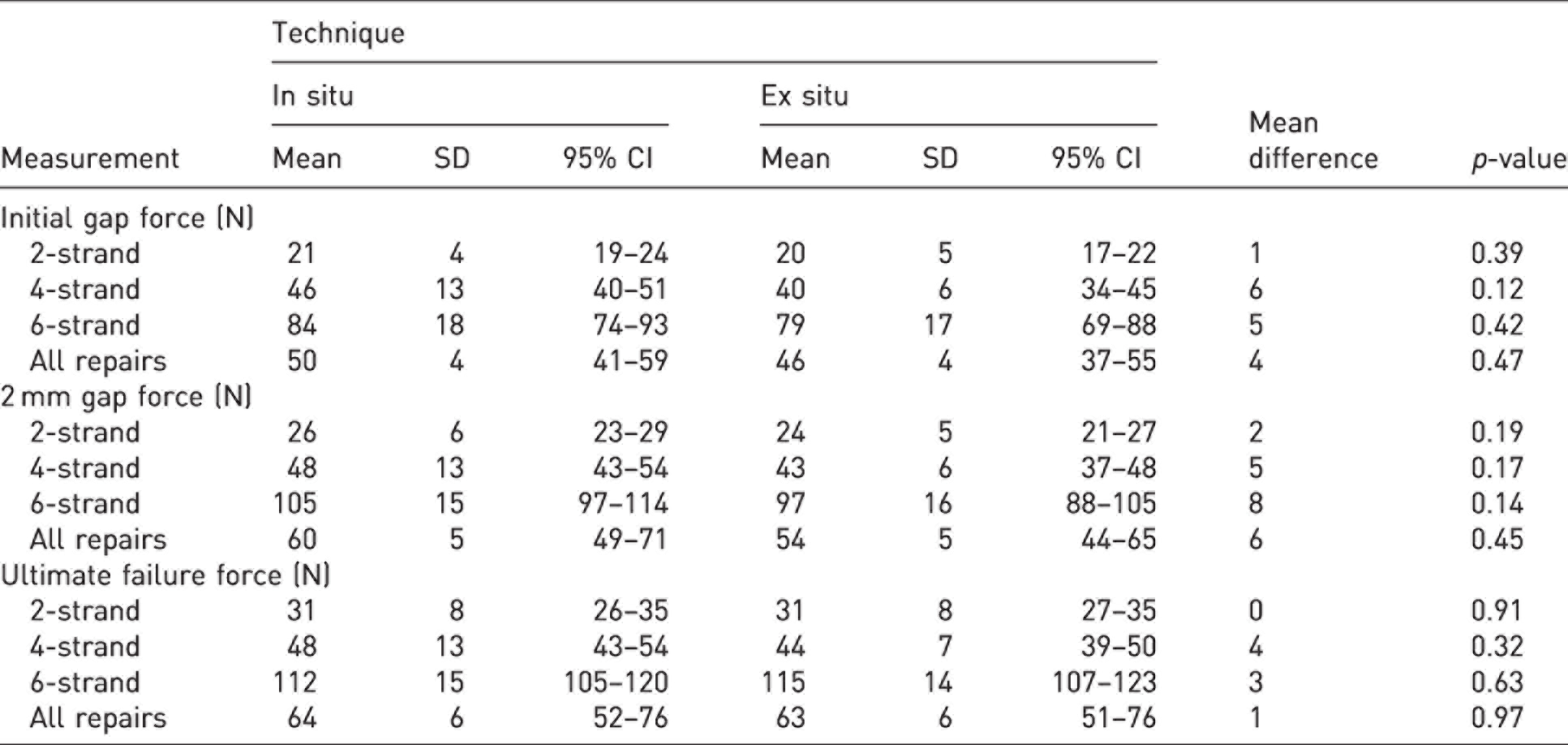
For both ex situ and in situ groups, 6-strand repairs were stronger than 4-strand repair (114 N versus 46 N, p < 0.001), and 4-strand repairs were stronger than 2-strand repairs (46 N versus 31 N, p < 0.001) at ultimate failure. The same trend was observed for force at initial gap and force required for 2 mm gap formation (all p < 0.001). There was no statistically significant difference in force at initial gap, 2 mm gap or ultimate failure between ex situ and in situ repairs in any group (Table 2). The ICC was 0.99 (95% CI, 0.988–0.994) (p < 0.001) for independent video measurements of initial gap, and 1.00 (95% CI, 0.994–0.997) (p < 0.001) for 2 mm gap.
Gap and failure force for the repairs.
Bulk at repair site
Overall, the CSA of the tendon at the repair site increased by 93% after a 2-strand technique, 117% after a 4-strand technique and 105% after a 6-strand technique. Although the percentage increase in CSA at the repair site was greatest for 4-strand repairs, this was not significantly larger than 6-strand repairs (p = 0.23), and there was no significant difference between 2- and 4-strand repairs (p = 0.06). There was a significantly greater percentage increase in CSA after 4- and 6-strand in situ repair compared with ex situ repair but not after 2-strand repair (Table 3). In a separate analysis of the small finger and long fingers, a significant difference (p = 0.03) in CSA between ex situ and in situ repairs was present for small finger flexor tendons, but not for long fingers (Table 3). There was no significant difference in percent increase in CSA between small versus long fingers.
Repair time and bulk at repair site.
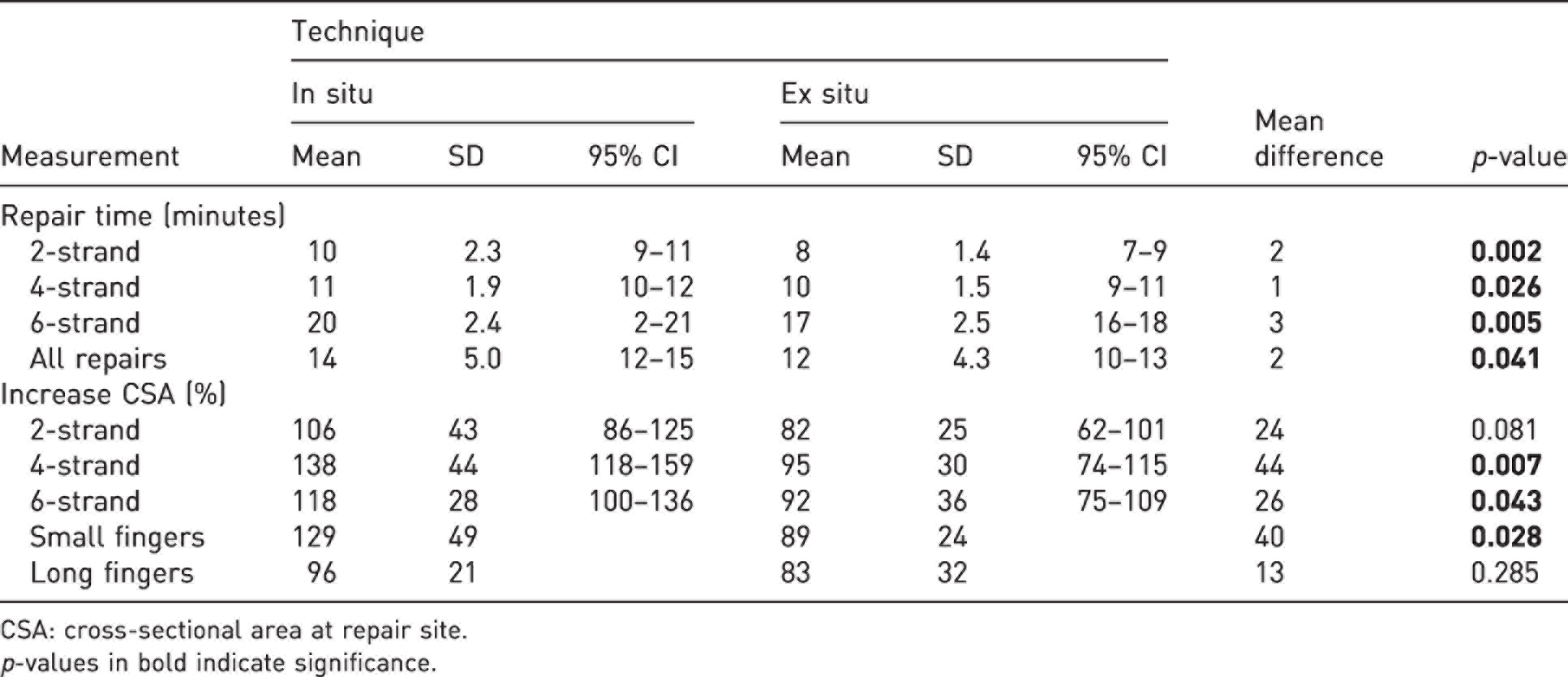
CSA: cross-sectional area at repair site.
p-values in bold indicate significance.
Repair time
Repair times were significantly longer for repairs with increasing number of strands, with mean repair times of 9, 10 and 18 minutes, respectively (p = 0.02 for 2- versus 4-strand, p < 0.001 for other comparisons. In situ repairs took significantly longer for all groups (Table 3). The duration of each repair type was consistent throughout the course of the study, without large variations or deviations (Figure 5).
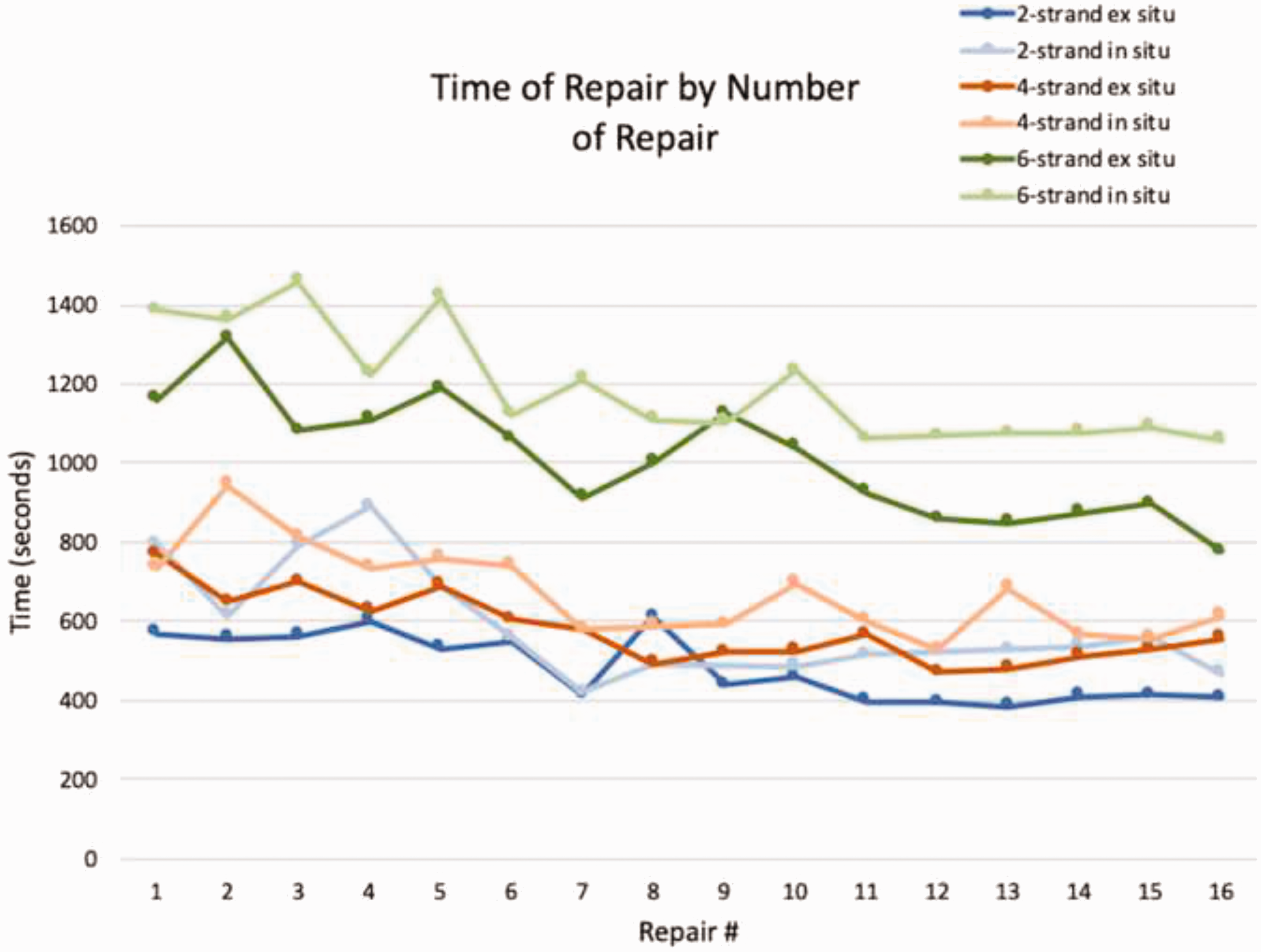
The duration of each repair, broken down by the order of repair in each repair type. Differences between in situ and ex situ repairs in each group are present at nearly every time point and persist over time.
Discussion
This investigation tested the hypotheses that flexor tendon repairs performed in situ would be weaker, bulkier and require more time to execute than the same repair performed ex situ.
The first hypothesis was not proven. Load to failure of in situ repairs was similar to ex situ repairs. Consistent with previous studies, strength of repair increased moving from 2- to 4- to 6-strand repairs. The load to repair failure in this study was comparable with that demonstrated in other studies of 2-, 4- and 6 strand repairs (Manchio et al., 2009; Vanhees et al., 2013).
All repairs resulted in increased bulk at the repair site. Repairs performed in situ were significantly bulkier than the ex situ counterpart for 4- and 6-strand repairs supporting the second hypothesis. We believe these differences are due to a more challenging technique (implying more tissue handling) when used in situ. The percentage increases in CSA are similar to results reported by Lawrence et al. (2005) in a study of 2- and 4-strand repairs using porcine tendons. Kozono et al. (2018) in porcine tendons and Bernstein et al. (2019) in human tendons reported post-repair CSAs in tendons that were larger than the absolute CSA increases seen in this study, but neither reported the data as a percentage increase. In contrast, Sanders et al. (2001) reported an increase in CSA of only 20% and 55% in 2- and 6-strand repairs, respectively.
In our study, a subgroup analysis of small and long fingers revealed a greater percentage increase in CSA after in situ versus ex situ repairs in small fingers compared with long finger tendons, although this trend did not reach statistical significance. Boyer et al. (2001) found that CSA did not affect tensile properties of a repair, and Bernstein et al. (2019) found that small finger tendons gapped and failed earlier than tendons from the other three digits, suggesting this was due to difficulty in accurately suturing smaller tendons. In several studies, the small finger was omitted from analysis due to the small size (Marrero-Amadeo et al., 2011; Xu et al., 2013; Zhao et al., 2004). We find this problematic since small finger flexor tendons are commonly lacerated (Gunturk et al., 2018; Su et al., 2005).
In support of our third hypothesis, the time required to repair a tendon in situ took significantly longer than the same repair performed ex situ (Figure 5). Whereas 4-strand repairs required an average of 1–2 minutes longer to perform than a 2-strand repair, 6-strand repairs required over 18 minutes to complete. Our data are comparable with that of Lawrence et al. (2005), although their investigation used porcine tendon and reported only time required for 2- and 4-strand repairs. The logical explanation for the time increases is that more complicated repairs have more steps and require more tendon handling, which has been hypothesized to promote adhesion formation by damaging the surface of the tendon.
Strengths of this study include the use of matched cadaveric hands and an injury model that simulates clinical flexor tendon injury. Load to failure was assessed by three observers working independently, and the interobserver reliability was high. Weaknesses of the study include the use of cadaveric material that differs biomechanically from living tissue. The suture techniques we employed may perform differently from other 2-, 4- and 6-strand techniques. While the same investigator tied all the sutures, no measurements were made of the tension on the sutures as they were tied, which could affect the bulk created at the repair site. CSA was calculated by making width and thickness measurements using callipers, which may introduce imprecision and inaccuracy given tendon elasticity. Also regarding CSA, an ellipsoid shape was assumed for the calculation, which is an estimate of the true tendon shape. Finally, flexor tendon injuries occur along the entire flexor tendon sheath. The data derived from this study, with injuries created 5 mm distal to the A2 pulley, may not be applicable to other flexor tendon injuries.
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.