
Abstract

Introduction
The hand and wrist are complex anatomical structures, with their function dependent on the integrity of bones, joints and ligaments. Different modalities of wrist imaging are used routinely for diagnosing fractures, joint malalignment, degenerative and inflammatory changes as well as for the assessment of healing and hardware position. Because of the complex three-dimensional (3-D) anatomy and wide spectrsum of diagnostic challenges, computed tomography (CT) now plays an important role, providing multiplanar reconstructions and better diagnostic accuracy (Müller et al., 2020; Welling et al., 2008).
Conventional CT scanners
Conventional CT scanners, also known as energy-integrating detector CT (EID-CT) scanners, however, have limited spatial resolutions, which can make it difficult to correctly diagnose pathologies such as subtle fractures, small joint incongruencies or changes in osteoporotic bone (Carpenter et al., 2014; Mallee et al., 2011; Matcuk et al., 2016; Nuchtern et al., 2015). Despite massive technical improvements in image reconstruction over the last decade, the use of EID-CT in diagnosis and follow-up of hand and wrist pathology remains limited because of the relatively high radiation doses and the severity of artifacts in the presence of metallic implants.
Photon-counting detector CT (PCD-CT) scanners
In recent years, the manufacturers of CT scanners have been working on new prototypes, so-called photon-counting detector CT (PCD-CT) scanners (Flohr et al., 2020; Willemink et al., 2018). The premise of these scanners is that the detectors count the number of individual incoming X-ray particles (photons) and measure their energy, which greatly reduces the inherent noise that is obtained with conventional X-ray detectors. Because the X-rays are directly converted to electronic signals, individual detector elements can also be made much smaller. Compared with the scan protocols currently used in EID-CT, PCD-CT therefore offers significantly sharper and more detailed images with increased contrast-to-noise ratio and a spatial resolution that enables accurate distinguishing of structures down to 0.2 mm in size (Bette et al., 2022; Kämmerling et al., 2022; Rajendran et al., 2021). This provides improved visualization of cortical and trabecular bone microarchitecture, also in smaller joints, at a 49% reduced radiation exposure compared with EID-CT (Rajendran et al., 2021).
Another feature of the PCD-CT is its ability to assess tissues with low attenuation (radiodensity), such as cartilage, ligaments, tendons, surface replacement materials and bone marrow. With EID-CT scanners, imaging of such structures remains challenging, due to the low attenuation of X-rays passing through the structures and resulting in poor image contrast. By utilizing the information about the energy of the detected photons, the user of PCD-CT can enhance or suppress tissues of interest, as well as materials such as calcium or intravenous contrast agents. As all X-ray spectral data is always available, multiple tissues and materials can be quantified and differentiated from each other simultaneously. With PCD-CT, images can be reconstructed at different X-ray energy levels. Low energy levels provide high bone contrast, but at high energy levels streak artifacts are less pronounced. Thus, spectral information, combined with advanced beam filtering, reduces metal artifacts, which makes it easier to visualize bone healing and may even allow for assessment of osseointegration of metallic implants.
Another advantage is that by processing multi-energy data, highly valuable information on other materials, such as prosthetic implants, can be visualized. Pilot projects on knee implants have shown that it is possible to detect polyethylene insert wear and metallic implant wear, something that no other imaging techniques could previously assess radiologically (Lau et al., 2021). Such high-resolution structural information can be of crucial importance for future evaluation of new prosthetic implants in the wrist and finger joints, allowing, for example, implant osseointegration and loosening to be assessed at the same time as grading of surface wear.
Because of its ability to measure the energy of each detected X-ray photon, PCD-CT could be used to combine bone density measurements while at the same time accurately visualizing bone microstructure. This could potentially revolutionize diagnosis and management of osteoporosis (Klintström et al., 2022; Willemink et al., 2018), and visualization of early trabecular healing.
The first clinical PCD-CT scanner was recently presented by Siemens Healthineers, (Forchheim, Germany) and one of the first installation was in April 2021 in The Netherlands (Erasmus MC, Rotterdam), after prototypes had initially been installed at centres in Sweden (Linköping University Hospital) and the United States (Mayo Clinic, Rochester). These clinically available scanners are now rapidly being introduced at centres worldwide and other CT vendors are expected to soon follow with new PCD-CT models in the near future. The rapid expansion and utilization of PCD-CT is also underlined by the steep increase of articles published around the technique in the last 5 years (Figure 1).
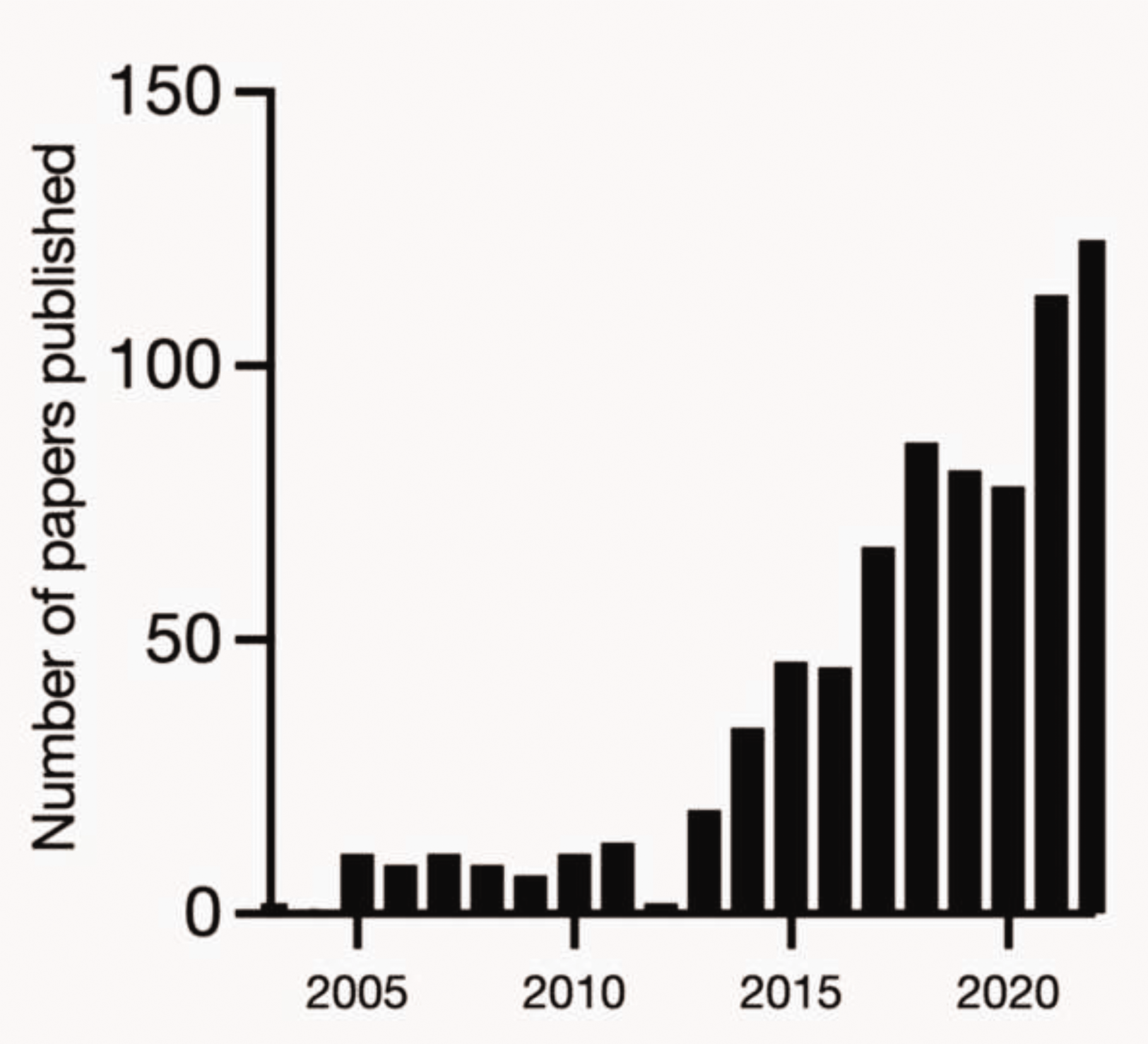
Number of articles published on photon-counting detector CT in the past 20 years.
Clinical applications in the hand and wrist
Ultra-high-resolution imaging in fractures
A major advantage of PCD-CT is its high spatial resolution (Etli et al., 2020). This enables a sharp delineation of even small fracture lines that would be easy to miss, for example, carpal bone fractures and small finger joints. Current state-of-the-art EID-CT scanners can already obtain high resolution by using a so-called comb filter, which partially cover detector elements, allowing for the reconstruction of slices thinner than the individual detector elements or the use of a ultra-high-resolution (UHR) scan mode (Flohr et al., 2007; Gondim Teixeira et al., 2021). This, however, comes at the cost of a higher radiation dose, and also spectral X-ray information and scan speed. In contrast, PCD-CT has a better spatial resolution while maintaining a low dose, high scan speed and spectral information. PCD-CT in the UHR mode reduces scan speed but remains faster than the UHR mode in EID-CT, while providing images with higher kernels and a large image matrix size. This allows for an image pixel size of 0.2 × 0.2 mm (at isocentre), which yields a sharp visualization of trabecular bone structures (Figures 2 and 3).

Three-dimensional visualization by the cinematic rendering technique. Input images were reconstructed with 0.2 mm slice thickness, high kernel (Br92) and high matrix size (1024 × 1024).
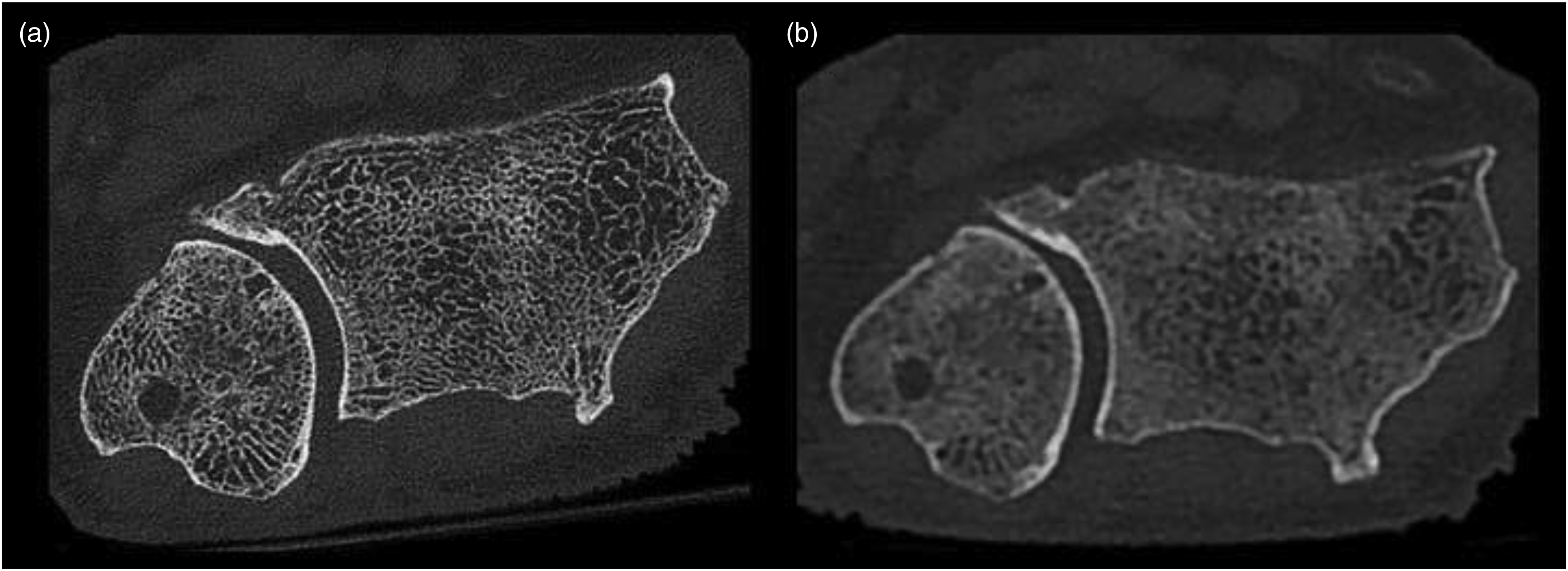
Axial images of the DRUJ obtained from a (a) clinically used UHR photon-counting detector CT protocol with a spatial resolution of 0.2 mm with half of the dose compared with the EID-CT image in a state-of-the art EID-CT UHR protocol (b), with a maximum spatial resolution of 0.4 mm acquired at a clinically used CTDIvol of 12 mGy.
Besides the ability to use thinner slices with PCD-CT as compared with EID-CT, images can be reconstructed with a sharper image kernel and larger image matrix. Thus, the image voxels are smaller and the edges between the voxels are more enhanced, providing substantially sharper images (Figure 4).
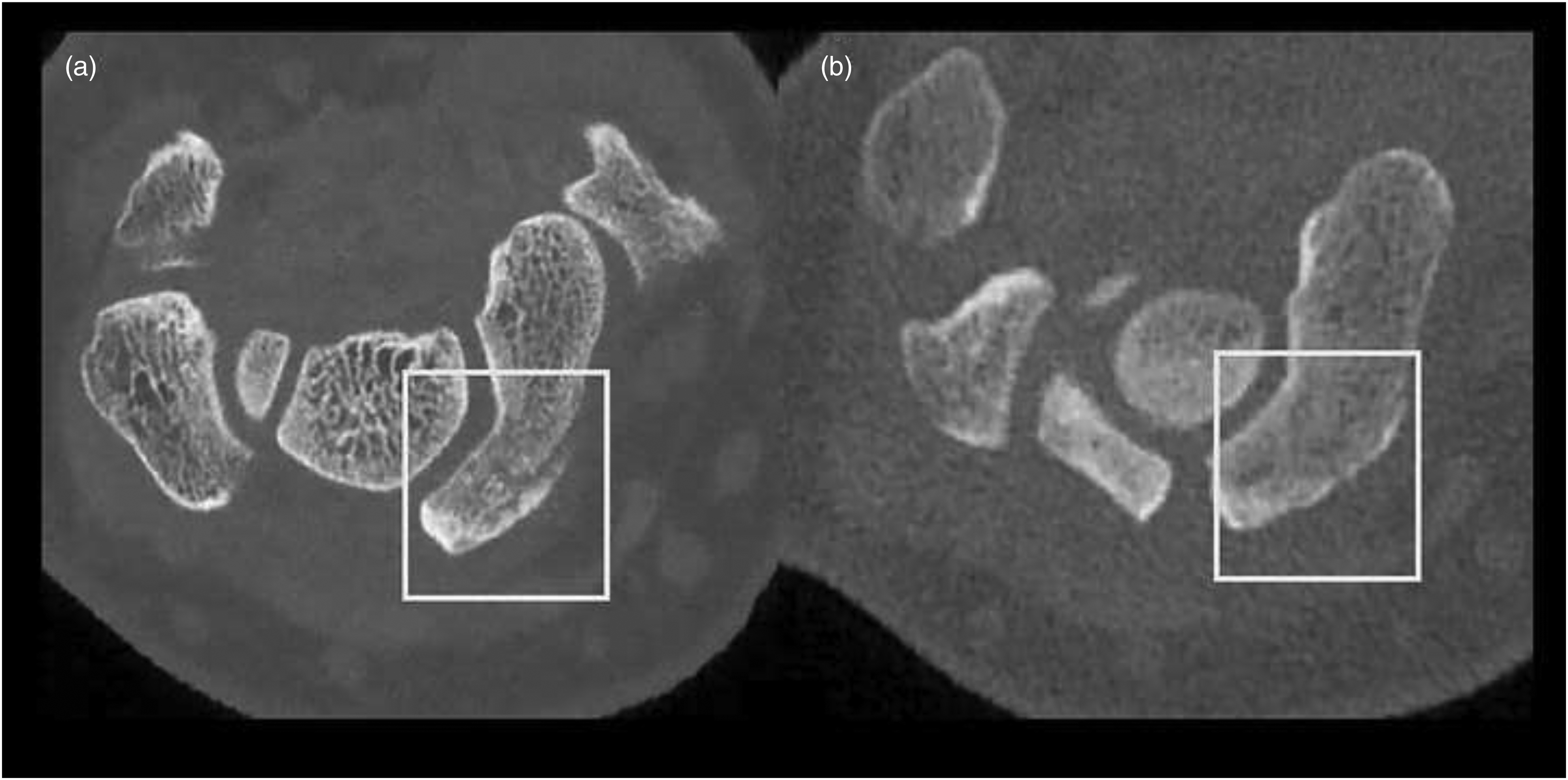
Photon-counting detector CT (a) can provide even higher spatial resolution of 0.2 mm than energy-integrating detector CT (b) with a spatial resolution of 0.4 mm, demonstrating more sharp delineation of the scaphoid fracture line (fracture indicated by the white box). Images are acquired at the same radiation dose of CTDIvol32 of 2.65 mGy.
Osteosynthesis material and protheses imaging
Imaging of the wrist and hand where osteosynthesis materials and protheses are present, often present with metal artifacts. These can appear as streaks, shading or rings and bands in the images (Barrett and Keat, 2004). Artifacts can sometimes be reduced by adaptation of scan parameters, such as high tube voltage, spectral shaping by the use of additional tin filtration or the use of dual-energy CT (Wellenberg et al., 2018). Within the reconstruction parameters, in particular using commercially available metal artifact reduction (MAR) algorithms, metal artifacts can be reduced as well (Rajendran et al., 2020; Wellenberg et al., 2018). Another technique is to use dual-energy CT with EID-CT and reconstruct images acquired from two photon spectra at different tube voltages, TwinBeam CT or the use of dual-layer CT (Booij et al., 2020), as this allows for reconstruction of so called virtual monoenergetic images (VMI) at arbitrary energy levels (keV) and the ability for artifact reduction. However, acquiring these dual-energy images with EID-CT often demands a dedicated protocol at the cost of scan speed due to shortening of the longitudinal coverage or cost of sacrificing the ability to scan with UHR.
The clinically used PCD-CT has all the tools available to acquire and reconstruct sharp images with reduced metal artifacts, while at the same time provide thin slices, spectral shaping, sharp reconstruction kernel, high matrix size, VMI and MAR (Figures 5 and 6).
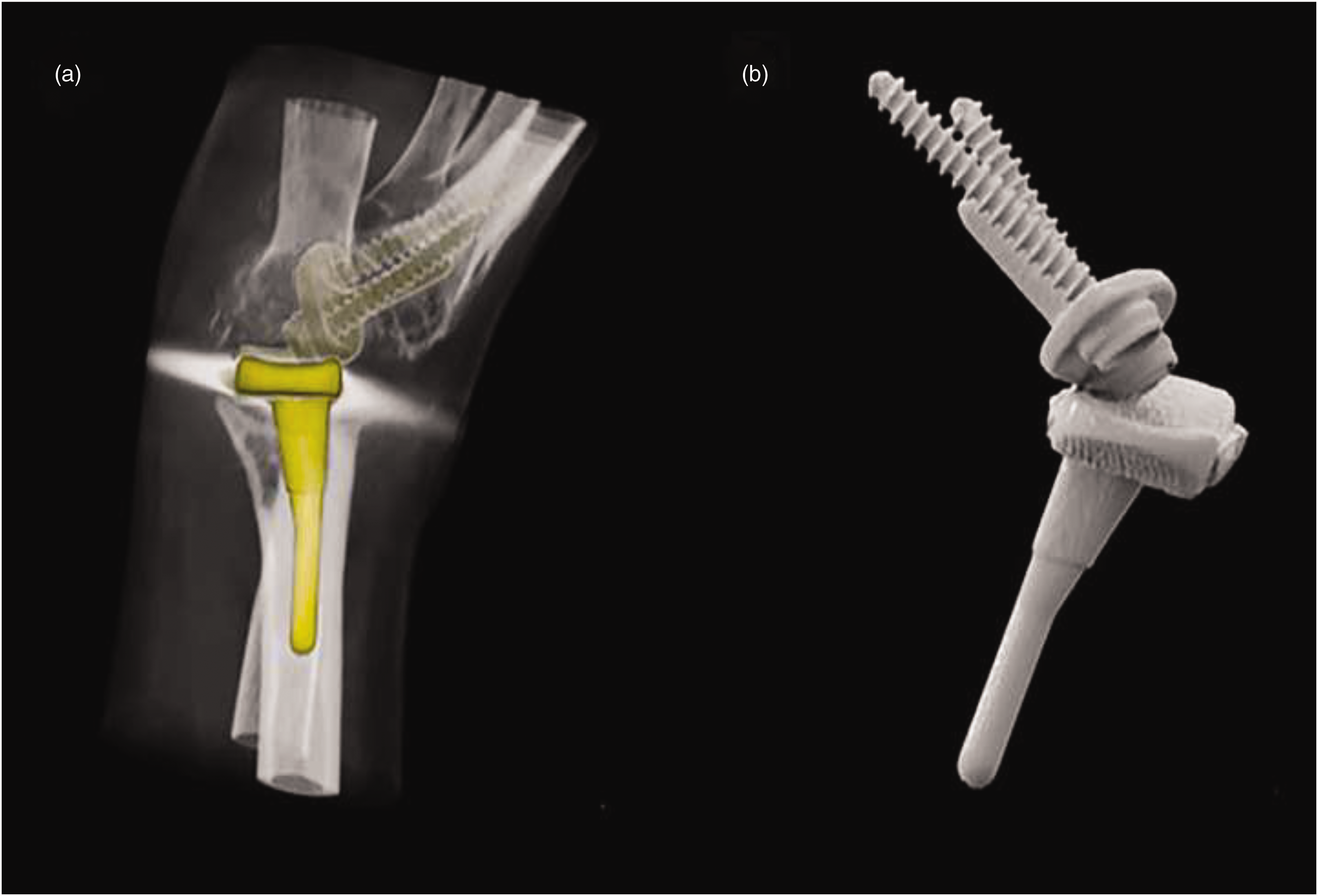
PCD-CT images showing great promise in visualization of implants. Ongoing projects include assessment of osseointegration, prosthetic movements using CT-based micromotion analysis (CTMA) and polyethylene implant wear. (a) Depicts prosthesis placement without metal artifacts and (b) the same prosthesis where bone structures are removed.

Scaphoid fracture with screw of a 20-year-old male. Scan was acquired with a dedicated spectral shaping (tin filtration) protocol with ultra-high-resolution kernel (Br89). (a,b) Greyscale images in the axial (a) and coronal (b) plane of the PCD-CT. (c,d) Greyscale images in the axial (c) and coronal (d) plane of a high-end EID-CT 2 weeks before the PCD-CT. (e) Cinematic rendering of the screw in the scaphoid from PCD-CT data.
Conclusion
The use of PCD-CT is likely to revolutionize many fields of medical imaging, but the improvement in image resolution and versatility would especially benefit musculoskeletal imaging. Due to fundamentally different detector technology, PCD-CT enables visualization of bone structures and small fracture lines, and is likely to provide better diagnostic accuracy.
Preliminary studies suggest that the availability of spectral information combined with high spatial resolution and low noise may prove valuable in reducing metal artifacts and visualizing bone marrow oedema and soft tissues, although further research is needed to determine the clinical benefit of these features.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CMIV and Erasmus MC receive institutional research support from Siemens Healthineers.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.