
Abstract

Introduction
Self-harm is a significant and increasing healthcare problem that is often met with prejudice and stigma, even by healthcare staff (Kilroy-Findley, 2015; MIND, 2016; NICE, 2022; Saunders et al., 2012). It is exceedingly common, with approximately one in ten adolescents reported as having self-harmed (NICE, 2022). Those who frequently self-harm require the input of hand surgery services, usually due to lacerations from self-cutting and foreign body soft tissue insertion (FBSTI) (Rogers et al., 2009).
Of those who self-harm, over 50% will repeatedly do so in the future. Self-harm also remains the strongest risk factor for a subsequent suicide attempt (Hawton et al., 2012; Madge et al., 2008) with a 19-fold increased risk of suicide and a 3.6 fold increased risk in all-cause mortality (Kapur et al., 2015). This is a significant burden of disease, estimated to cost health services from £200 up to £10,000 per patient, per year (Hunt, 2017; Rogers et al., 2009).
The management of patients who self-harm requires collaboration between the psychiatric and surgical services. Despite the integral role of the hand surgery team in the management of such patients, self-harm receives very little attention in the surgical literature and there are no clear guidelines nor consensus on the surgical management of these patients. This article aims to better equip hand surgeons when managing patients who have self-harmed by summarizing the available evidence and guidelines on both the nature of self-harm and its management.
National guidance
National guidance has been released in the United Kingdom (UK), Australia and New Zealand (Carter et al., 2016; NICE, 2013; NICE, 2022). These guidelines are broad, covering many types of self-harm and are designed for use across many healthcare settings, and discussion of their entirety is outside the scope of this article. However, all of these advocate to prompt psychosocial assessment and treatment of patients in addition to the management of the physical consequences of their actions.
Psychological features
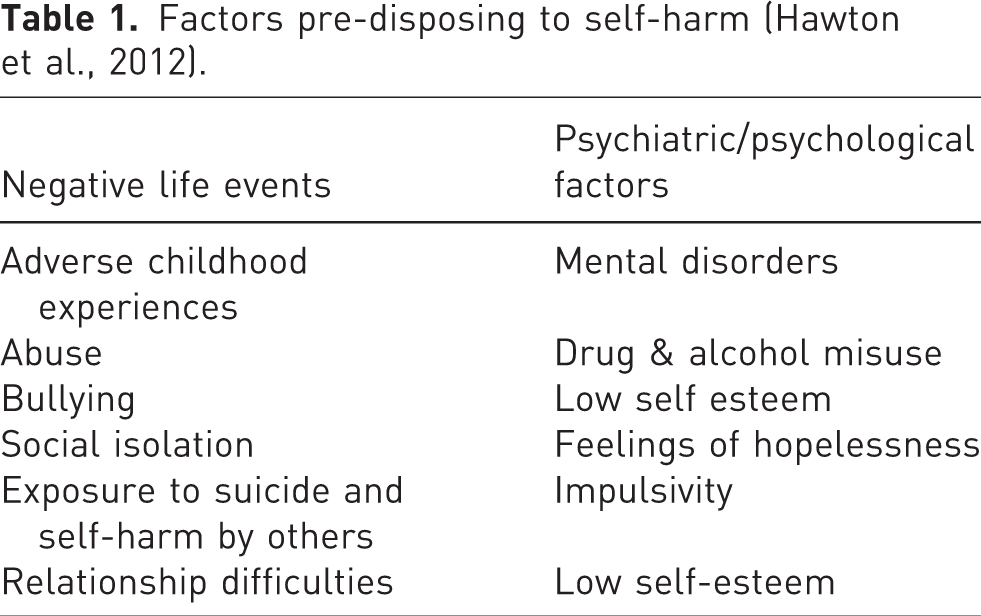
Self-harm is considered to be multifactorial in origin; the result of predisposing psychiatric and psychological factors combined with negative life events (Table 1) (Hawton et al., 2012). Although there is an increased risk of suicide, self-harm is often carried out without any suicidal intent (MIND, 2016) and represents a coping mechanism to deal with overwhelming emotional distress (Hunt, 2017; MIND, 2016). Patients usually follow a pattern of pent up negative emotions resulting in the act of self-harm followed by relaxation and relief of emotion (Hunt, 2017; MIND, 2016). The return of this compulsion after the period of initial relief results in further injury, giving rise to difficult clinical scenarios, such as repeated soft tissue trauma that may prevent wound healing.
Factors pre-disposing to self-harm (Hawton et al., 2012).
It is estimated that up to 50% of patients admitted to a surgical ward following self-harm have not undergone a psychiatric assessment (Concannon et al., 2019; Rashid and Brennen, 2006). Early involvement of psychiatric services will aid surgical decision-making and the management of the patient by helping risk assess and optimize these patients prior to surgical intervention (Hold et al., 2010; NICE, 2022; Rashid and Brennen, 2006; Rogers et al., 2009). This will ensure patients are managed in a safe environment and allow time for them to regain capacity and consent for a procedure should they not be able to do so at the time of presentation.
Physical features
There are many forms of self-harm, but these can be broadly categorized into self-poisoning or self-injury (NICE, 2022). Paracetamol and anti-depressant overdose are the two most common forms of self-poisoning (NICE, 2022). Physical acts of self-harm range from skin cutting, burning, picking, excessive scratching, foreign body insertion and breaking bones by striking objects.
Self-cutting
Self-cutting is the most common form of self-harm but commonly co-exists with self-poisoning and therefore it is important to specifically enquire about potential overdose as the medical management of poisoning takes priority over surgical management of the wound (Madge et al., 2008). The volar wrist and forearm is the most common site for self-cutting injuries (Cho and Choi, 2020). The current United Kingdom (UK) guidance recommends assessing the severity of the injury and how urgently treatment is required, but does not offer further guidance on how this should be assessed (NICE, 2022). Significant injury to a tendon or nerve can occur following self-harm, around 50% of self-inflicted wounds to the wrist are deep, with 33% injuring an anatomical structure (Cho and Choi, 2020; Fujioka et al., 2012). Those with multiple lacerations, fewer previous acts of self-harm and males are also more likely to have a deep injury (Fujioka et al., 2012). In any patient, the wound should be examined to exclude infection, gross contamination or underlying tendinous or neurovascular injury regardless of size or apparent depth.
The injury pattern in self-inflicted wounds differ from accidental or inflicted wounds (Kisch et al., 2019; Lee et al., 2016). Due to the mechanism of injury, wounds to the left volar wrist are sustained using the right hand leading to predominantly radial-sided or median injuries, most commonly injuring the palmaris longus (Kisch et al., 2019; Lee et al., 2016). In contrast, non-intentional wounds are more likely to involve ulnar structures (Lee et al., 2016). Self-cutting often normally results in transverse lacerations, increasing the risk of tendinous injury but reducing the risk of arterial injury in comparison with longitudinal wounds (Kisch et al., 2019). Wherever possible, it is recommended that wounds be closed with skin adhesive or steri-strips rather than sutures, with the benefit of being less painful and avoiding a further attendance for suture removal. Moreover, there is currently no evidence that one form of wound closure is better in terms of complication rates or cosmetic outcomes (Esmailian et al., 2018).
Over 50% of patients will go on to injure themselves again, and unfortunately, one in 15 of these will be within 30 days of the initial injury (Arensman et al., 2014; Madge et al., 2008). The repeat trauma can present obstacles to wound healing, with the patient attempting to re-open the wound or use it as a site for foreign body insertion (Rogers et al., 2009). For this reason, some would advocate a conservative approach to wound management, favouring healing by secondary intention, and intervening only in cases where there is evidence of underlying structural injury or infection. However, this approach has been associated with an increased wound infection rate and patients continuing to present with episodes of self-harm (Rogers et al., 2009).
A reasonable surgical rationale would be to manage hand and wrist wounds initially in the emergency department (ED) with irrigation and haemostasis. Wounds without evidence of infection or underlying structural injury should be closed in the ED, where possible. In patients where there are deeper wounds with clinical evidence of underlying injury, it is still more appropriate to await psychiatric input and for the patient’s mental state to recover before offering surgical intervention unless there is sepsis from wound infection or life-threatening bleeding needing emergent management, both of which are rare. This will ensure the patient is able to comply with the postoperative rehabilitation regime required to protect tendon and nerve repairs from failure or postoperative stiffness.
Soft tissue foreign body insertion
This form of self-harm involves the insertion of objects into the soft tissues, more frequently in the upper limbs. Wounds from self-cutting are sometimes used as a point of access (Wraight et al., 2008) for their insertion. Definitive management varies depending on the site and presence of infection; foreign bodies can be left in-situ provided there is no evidence of neurovascular or tendon injury (Wraight et al., 2008). This is particularly so where there are multiple items or when the foreign bodies are in close proximity to vulnerable structures. Surgical removal remains the mainstay in many units. However, in centres with the available expertise, image-guided foreign body removal (IGFBR), is an increasing popular treatment method (Bradley, 2012; Young et al., 2010). The technique typically involves the use of ultrasonography or fluoroscopy to detect the foreign body that facilitates its removal, usually performed under local anaesthetic.
There are few reports on the surgical management of self-inflicted foreign bodies in subcutaneous tissues. Given the number of reports of successful conservative management, a reasoned approach would be to remove foreign bodies only in cases of infection, structural injury or if the object is made of poisonous or harmful material.
Medicolegal considerations
It is not uncommon for patients who self-harm to refuse treatment, which raises several ethical and legal difficulties. Anyone over the age of 16 should be assumed to have capacity until proven otherwise, as per the Mental Capacity Act (Department of Health, 2005). Consequently, this may allow the patient to make unwise medical decisions putting them (but not others) at risk of harm. Both UK guidance and the Montgomery ruling specifies that all treatment options should be fully discussed with patient and all efforts made for the patient to give informed consent (Montgomery vs Lanarkshire Heath Authority, 2015; NICE, 2022).
Patients who lack capacity to consent should be treated in their best interests. Loss of capacity may be due to temporary factors, for example intoxication or acute psychiatric illness, in which case the surgical management of their injuries can be delayed until the effects of these have resolved. If they are actively refusing treatment or lacking capacity but treatment is required urgently, then it is permissible to proceed under the Mental Capacity Act. Alternatively, the patient can be detained under the Mental Health Act (Department of Health, 2007) if there is evidence of mental illness.
Both these legal powers should only be used if there are no less restrictive alternatives to treatment. Applying guidance into clinical practice can be challenging, highlighting the importance of combined decision-making and a sound understanding of the ethical issues surrounding treatment. Figure 1 outlines a decision-making algorithm adapted from previous NICE guidance to aid clinicians in managing patients who are refusing treatment.
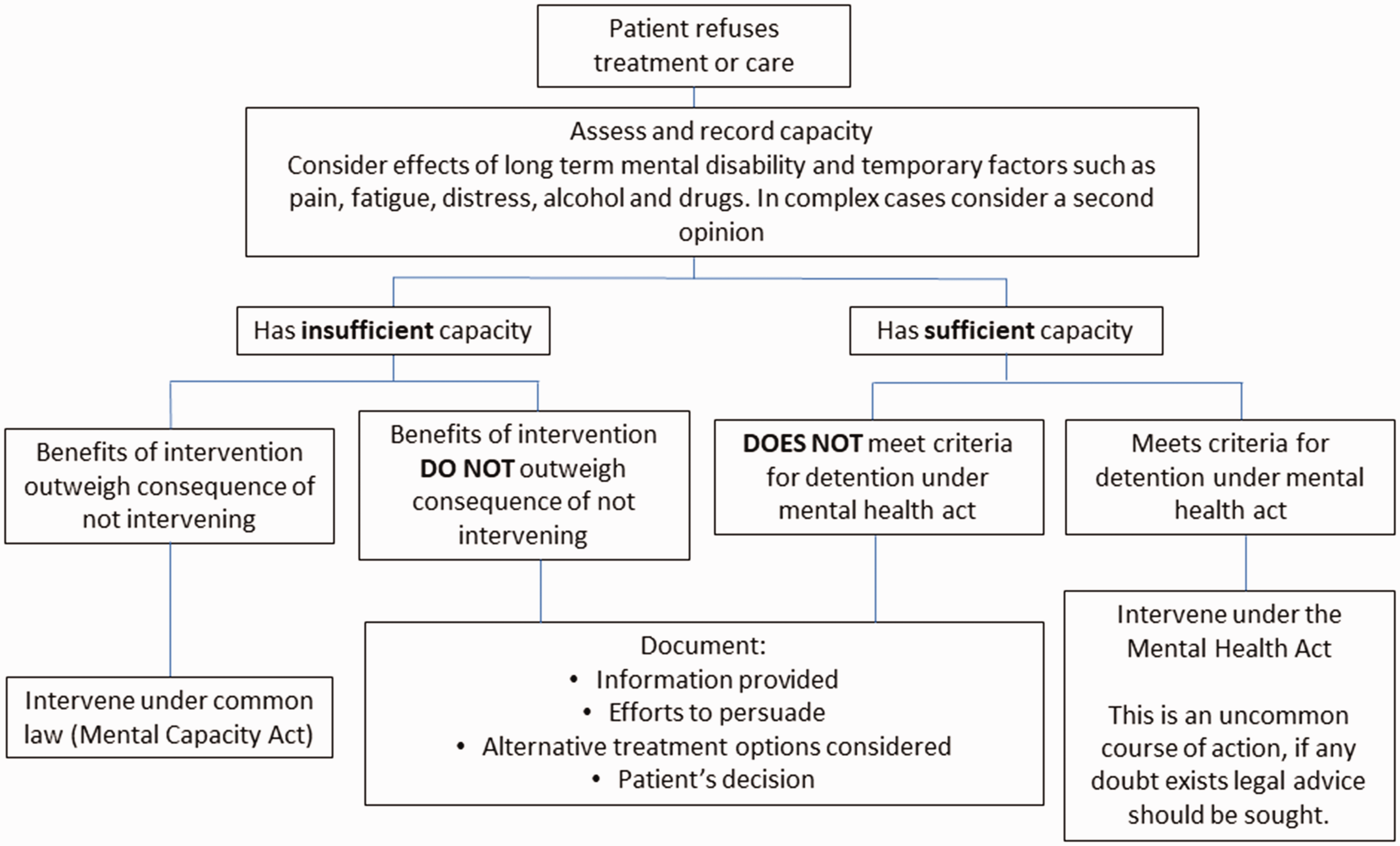
Decision-making algorithm for patients refusing treatment. Adapted with permission from previous NICE guidance.
Conclusion
Self-harm is a common and increasingly prevalent problem. It is important to improve the awareness of psychological factors and the medicolegal aspects of self-harm among those involved in caring for this group of patients. While most orthopaedic and plastic surgery departments have considerable experience in the management of these injuries, few have clear guidelines. Given the limited evidence in the surgical outcomes for these patients, early involvement by a psychiatry team will benefit subsequent surgical decision-making and treatment plans.
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.