
Abstract
The functional results of proximal row carpectomy with a proximal capitate resurfacing using a pyrocarbon implant were evaluated in a retrospective, multicentric, multi-operator study. The outcomes of patients operated on at five surgical centres between January 2005 and December 2018 were reviewed. The data were collected by an independent observer during standardized consultations. Based on 30 patients with a mean follow-up of 7 years, the median range of flexion and extension was 65° and the median radioulnar tilt was 45°. The median Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH) score was 14 and the improvements in strength and pain were good. Compared with the preoperative values, significant improvements were seen in the flexion and extension range of motion, radioulnar tilt and pain score. No postoperative complications were recorded.
Introduction
Midcarpal arthrosis is a common pathology that results in pain, loss of strength and decreased range of motion. The aetiology is multifactorial and includes traumatic and genetic causes. Therapeutic solutions depend on the location of the damage. In patients with degenerated radioscaphoid and proximal capitate surfaces, proximal row carpectomy with replacement of the proximal capitate by a pyrocarbon implant is one of the treatment options. Pyrocarbon, being inert, does not integrate with the surrounding bone. However, the long-term behaviour of pyrocarbon in relation to human bone and soft tissues is unclear. Thus, the objective of this study was to evaluate the long-term outcomes of patients who underwent proximal row carpectomy with capitate resurfacing using a pyrocarbon implant.
Material and methods
Patients who underwent proximal row carpectomy and proximal capitate resurfacing for scapholunate advanced collapse (SLAC), scaphoid nonunion advanced collapse (SNAC) or scaphoid chondrocalcinosis advanced collapse (SCAC) with proximal capitate arthrosis between January 2005 and December 2018 at five French surgical centres were included in this study. Clinical indications for initial surgery were pain, loss of strength and functional disability of the wrist. Patients with degenerative damage to the radiolunate joint, as determined on preoperative radiographs and arthro-CT of the wrist, were excluded. Of the 45 patients who met the inclusion criteria, 10 were lost to follow-up and five refused to participate. The final study population therefore consisted of 30 patients. The mean age of the four women and 26 men was 59 years (range 50 to 65). Two patients had non-manual jobs and the rest were manual workers. In 20 patients, surgery was performed on the dominant side. Among the participants, 26 had wrist arthrosis due to Stage 3 SLAC (Watson and Ballet, 1984), and the remaining four had a Stage 3 SNAC. Proximal row carpectomy with capitate resurfacing was the primary surgical procedure in 28 patients. Revision surgery with capitate resurfacing for ongoing pain following proximal row carpectomy was performed in two patients.
All patients were evaluated clinically and radiologically once by a single independent observer at the last clinical follow-up. Consultations were performed in the clinic after the retrieval of all relevant clinical data from the medical files. The primary outcomes were the functional results as defined by wrist range of motion in flexion and extension, radioulnar tilt, pronosupination, as well as grip strength on the operated side and the Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH) score. Secondary outcomes were the delay in return to work and the radiological changes, including peri-implant fracture, implant loosening and carpal height. The carpal height index was calculated manually for all patients according to the Youm index (Youm et al., 1978) (Figure 1). These criteria were chosen because they are commonly used in the assessment of proximal row carpectomy and capitate resurfacing (Jager et al., 2017; Kendall et al., 2005; Krakauer et al., 1994; Mulford et al., 2009; Vance et al., 2005; Watson and Ballet, 1984; Watson et al., 1999). The data retrieved during the consultation included habitus, medical history, ongoing treatments, date of surgery and postoperative complications such as infection or capitate fracture. A clinical examination of the wrist was then performed. The range of motion of the wrist was measured using a goniometer and grip strength of the operated wrist was measured using a Jamar dynamometer. In addition, patients completed a self-reported pain questionnaire based on a visual analogue scale (VAS) and a QuickDASH assessment. At the last clinical follow-up, the most recent radiographs were analysed to detect implant loosening and to determine carpal height.
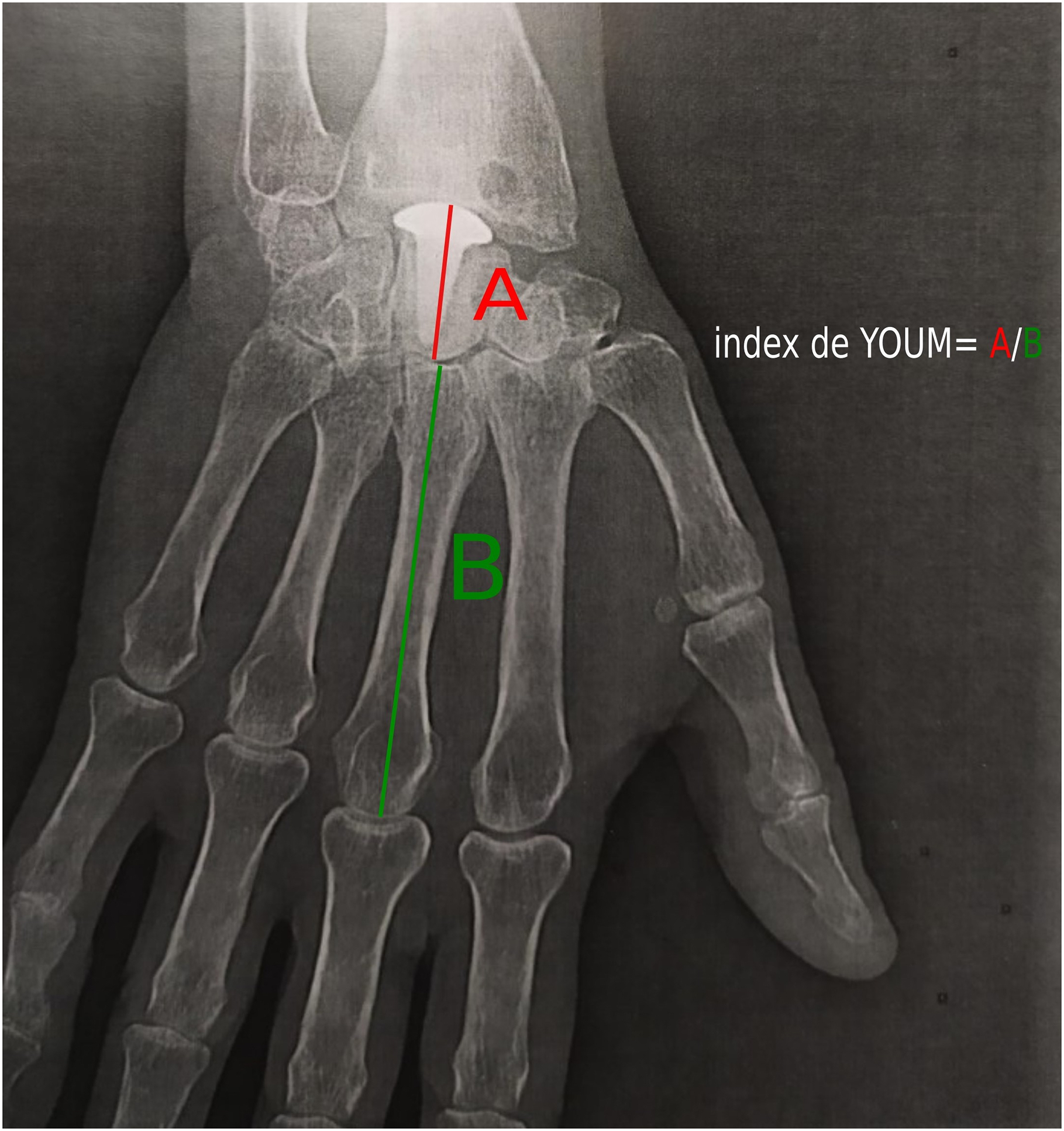
Radiograph demonstrating measurements for calculation of Youm index (Youm index = A/B).
Statistical analysis
Continuous variables are expressed as the median and range, and categorical variables as frequencies and proportions. The non-parametric Wilcoxon rank sum test and non-parametric Fisher’s exact test were used for univariate analysis, to compare pre- and postoperative results. A p-value <0.05 was considered statistically significant. All statistical analyses were performed using R software (version 3.3.2; R Foundation for Statistical Computing, Vienna, Austria).
Results
The median follow-up was 7 years (range 3 to16). At the last follow-up, improvements in the wrist range of movements and the pain score were found to be statistically significant (Table 1). The median grip strength and the QuickDASH score were also better, but this did not reach statistical significance.
Pre- and postoperative values.
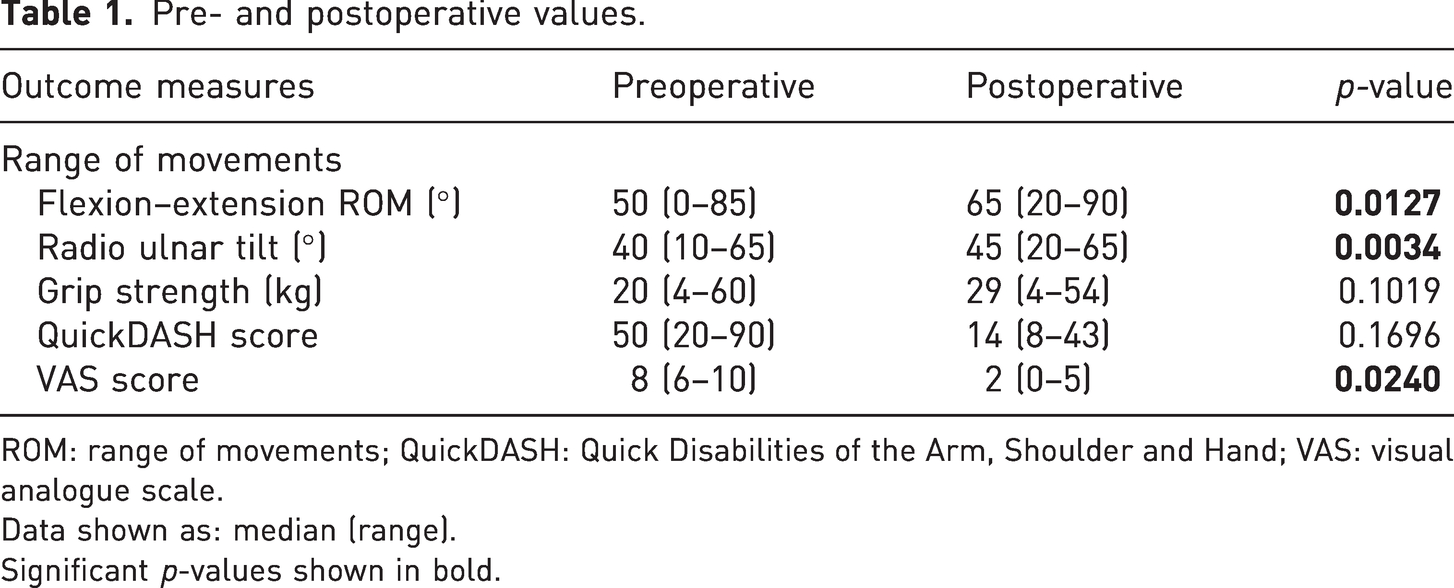
ROM: range of movements; QuickDASH: Quick Disabilities of the Arm, Shoulder and Hand; VAS: visual analogue scale.
Data shown as: median (range).
Significant p-values shown in bold.
At the last clinical follow-up, the two patients who had non-manual work had returned to the same job. Among the 28 manual workers, eight had retired but 20 were still working. Seven out of those 20 were able to return to their previous job. The remaining 13 had to adapt by using less strength during work-related activities. Among the patients who had retired, two had been able to continue in the same job after surgery and retired at the expected retirement age, whereas six had to take early retirement as a result of their wrist problems. The median delay before returning to work for all the 30 patients was 3 months (range 1.5 to 8).
There were no signs of peri-implant fracture or implant loosening in any patient on the radiographs. The radiolucent border around the implants seen on every radiograph remained unchanged during follow-up. The median Youm index at the last radiological follow-up was 0.38 (range 0.31 to 0.44).
There were no postoperative complications recorded, including infections or capitate fracture. None of the patients required further wrist surgery following proximal row carpectomy with capitate resurfacing.
Discussion
Wrist arthritis is a common pathology. According to the Watson classification, damage beyond Stage 3 involves the midcarpal joint (Watson and Ballet, 1984). When the proximal part of the capitate is arthritic, several therapeutic options are available. Midcarpal arthrodesis remains the first choice as it provides good pain relief and strength preservation, although it is associated with a decrease in wrist range of motion and a risk of dorsal impingement or hardware issues (Kendall et al., 2005; Krakauer et al., 1994; Mulford et al., 2009; Vance et al., 2005; Watson et al., 1999). Proximal row carpectomy with proximal pyrocarbon capitate resurfacing is an alternative option. It has broader indications than an isolated proximal row carpectomy, which is more suitable for patients with less advanced wrist arthritis and an intact proximal capitate surface.
Our assessment showed that surgery significantly improved wrist movements based on comparisons of the preoperative values and those at the last clinical follow-up. These results are in agreement with the main studies on this subject (Giacalone et al., 2017; Kopel, 2018; Marcuzzi et al., 2014; Szalay et al., 2012). Goubier et al. (2011) however, reported decreased range of movements in their study, but there is lack of information on their rehabilitation protocol or on the duration of the postoperative immobilization. In more recent studies showing results consistent with ours, emphasis is placed on the importance of the dorsal approach with preservation of the dorsal intercarpal ligament and the limitation of postoperative immobilization time (Marcuzzi et al., 2014). We speculate that an evolution of the surgical approach and the duration of postoperative immobilization may have helped to improve the postoperative range of movements and may explain this difference in results between Goubier et al. (2011) and the other main studies on resurfacing capitate pyrocarbon implants (RCPI) published subsequently (Giacalone et al., 2017; Kopel, 2018; Marcuzzi et al., 2014; Szalay et al., 2012).
The grip strength evaluation in our patients showed an improvement between the preoperative value and the last clinical follow-up, although the differences were not statistically significant. The improvement in VAS score for pain, however, was statistically significant. These findings are consistent with other studies (Giacalone et al., 2017; Kopel, 2018; Marcuzzi et al., 2014; Szalay et al., 2012).
Although the improvement in the QuickDASH score was not statistically significant in this study, the trend was similar to that noted by Kopel (2018) in his study of 35 RCPI with a mean follow-up of 30 months. Szalay et al. (2012) reporting on five patients with a mean follow-up of 34 months, also showed an objective improvement in the function of the operated wrists without specifying a score.
Two recent studies on first row carpectomy with RCPI highlighted higher rates of return to work compared with our study (Giacalone et al., 2017; Marcuzzi et al., 2014). In fact, Giacalone et al. (2017) achieved an 84% return to work in his study of 25 RCPI with a minimum follow-up of 2 years. However, there was no precise information on the details of work of the patients in these two studies. It would be logical to assume that it will be more difficult for an individual who had a wrist operation to resume manual work that required repeated carrying of heavy loads than someone who did an office-based job. The larger proportion of manual workers in our study might explain this slightly lower percentage of return to work.
There is lack of information on the relevance of radiolucent border around the RCPI in the literature, but there is no suggestion that it affects the clinical results. This radiolucent border visible around the implant is created as a result of the graphite centre of the implant being visible on radiographs while the surrounding pyrocarbon is radiolucent. Widening of the radiolucent border in the radiographs during the last clinical follow-up compared with the immediate postoperative radiographs could be suggestive of osteolysis. However, other authors have described a normal reaction of the bone to pyrocarbon with other implants, such as the adaptative proximal scaphoid implant (Tornier Cie., Montbonnot, Saint Martin, France) used for replacement of the proximal scaphoid (Santos et al., 2018). None of our patients experienced implant loosening, and all the pyrocarbon implants remained in the same position after surgery, perhaps because pyrocarbon is an inert material with no possibility of bone integration.
In our study, the mean Youm index of 0.35 used to measure carpal height was lower than that reported in other publications (range 0.51 to 0.57) (Gilula et al., 2002; Laronde et al., 2016; Youm et al., 1978). Previous authors concluded that the loss of carpal height in wrist osteoarthritis was of concern as the functional results were directly impacted (Gjika et al., 2012; McMurtry et al., 1978; Youm et al., 1978). However, this was not the experience of Laronde et al. (2016), who reported no correlation between loss of strength and loss of carpal height. The loss in carpal height was greater after a proximal row carpectomy than following a midcarpal arthrodesis, but there was no significant difference in postoperative strength. This finding is in accordance with our results, as none of our patients experienced major functional consequences of a reduced carpal height below the normal value.
We had no early or late postoperative complications requiring surgical revision, which agrees with other published series (Giacalone et al., 2017; Kopel, 2018).
The limitations of our study were related to its descriptive and retrospective nature, as well as the small sample size. Nonetheless, our cohort was among the largest published so far, and the duration of follow-up was longer than the other studies (Giacalone et al., 2017; Goubier et al., 2011; Kopel, 2018; Marcuzzi et al., 2014). Although we did not evaluate intraobserver variability, we assumed that this was minimal because the same method was used for each radiological analysis. We used the QuickDASH score as in several other wrist studies, rather than a specific wrist functional score such as the Patient-Related Wrist Evaluation (PRWE) score (Bellemère et al., 2012a, 2012b; Dickson et al., 2015; Kopel, 2018). The PRWE score would have allowed us to assess the function of the wrist more precisely than the QuickDASH by assessing difficulties in performing very specific activities (Shafiee et al., 2021). However, the QuickDASH score remains a reliable and valid score for assessing upper limb function frequently used for wrist and hand evaluation (Peters et al., 2015; Smith et al., 2022).
Proximal row carpectomy with proximal capitate resurfacing using a pyrocarbon implant provided satisfactory long-term outcomes in our study. Additional comparative studies are needed to investigate the advantage of this surgical procedure over midcarpal arthrodesis.
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.