
Abstract
In this clinical trial, patients were randomized to receive a pedicled vascularized bone graft, based on the 1,2-intercompartmental supraretinacular artery, or a non-vascularized iliac crest graft. Fixation was done with K-wires. Union and time to union were assessed using CT scans at regular intervals. Twenty-three patients received a vascularized graft, and 22 received a non-vascularized graft. Thirty-eight patients were available for union assessment and 23 for clinical measurements. There were no significant differences in union incidence, time to union, incidence of complications, patient-reported outcome scores, or wrist mobility and grip strength at final follow-up between the treatment groups. Smokers were 60% less likely to achieve union, independent of graft type. When controlling for smoking, patients receiving a vascularized graft were 72% more likely to achieve union. Given our small sample size, results should be interpreted with caution.
Keywords
Introduction
Biologically, vascularized bone grafting (VBG) has been shown to enhance bony healing. Using a canine model of surgically induced scaphoid proximal pole avascular necrosis (AVN), Sunagawa et al. (2000) demonstrated that VBG increases bony perfusion, osteoblast density, and osteoid coverage compared with non-vascularized bone grafting (NVBG). However, the current literature is inconclusive on whether VBG provides a clinical benefit for the treatment of scaphoid nonunion (Merrell et al., 2002; Munk and Larsen, 2004; Pinder et al., 2015).
The objective of this randomized clinical trial (RCT) was to compare the results of VBG based upon the 1,2-intercompartmental supraretinacular artery (1,2-ICSRA) to NVBG from the iliac crest in patients with established scaphoid nonunions and assess the feasibility of using VBG as the index procedure. We hypothesized that VBG would result in more rapid and higher incidence of union in comparison with NVBG in the treatment of scaphoid nonunions.
Methods
Institutional ethics review board approval was obtained, and the Consolidated Standards of Reporting Trials guidelines were adhered to. All patients presenting to a tertiary academic upper extremity unit between January 2008 and June 2016 were assessed for eligibility for enrolment in this RCT (Figure 1).
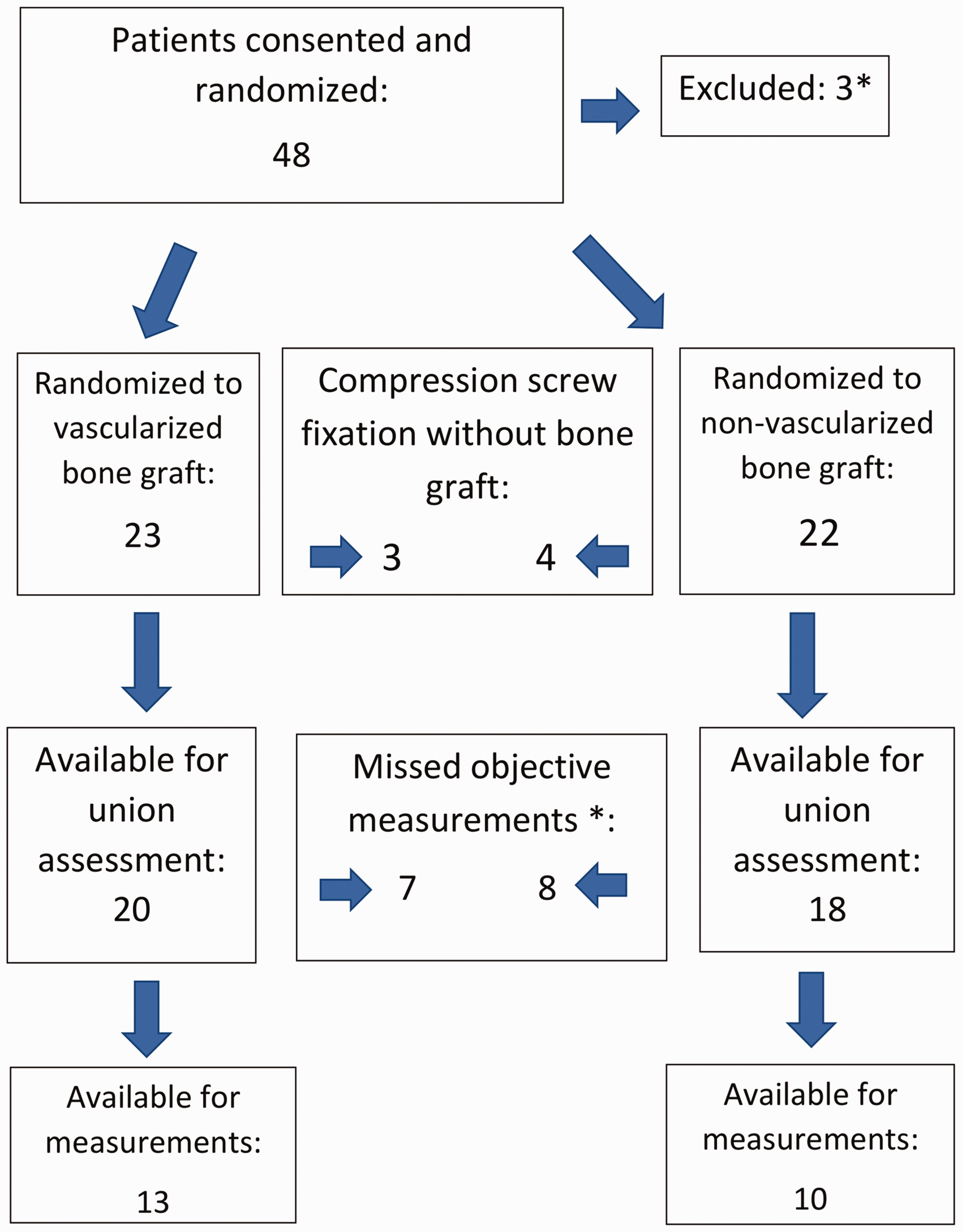
Consolidated Standards of Reporting Trials flow diagram.
Inclusion criteria
All patients with a confirmed diagnosis of a scaphoid nonunion that were deemed surgical candidates and consented to participate in the study were randomized to receive either a pedicled VBG based upon the 1,2-ICSRA, or a NVBG from the iliac crest. Nonunion was defined as a scaphoid fracture with <10% bony union across the fracture site on sagittal CT (120 kV, 200 mA, 0.8 s rotation, 0.625 mm thick) (Bain et al., 1995) after at least 16 weeks of appropriate non-operative treatment or morphologic features of nonunion on plain radiographs and/or CT, such as resorption and sclerosis at the fracture site or major cyst formation.
Exclusion criteria
Our goal was to study a homogeneous cohort of patients. For that reason, we excluded those that demonstrated proximal pole fragmentation or AVN on preoperative magnetic resonance imaging scan with gadolinium. Patients were also excluded if they were skeletally immature, exhibited radiographic evidence of Grade 2 or higher scaphoid nonunion advanced collapse arthritis (Mack et al., 1984), if they had any medical conditions precluding anaesthetic use or refused to give consent for participation.
Randomization and blinding
Patients were randomized to surgical intervention using sealed envelopes. Once allocated, neither patients nor surgeons were blinded to the treatment group.
Clinical assessment
Clinical assessments were performed at baseline, 3, 6 and 12 months post-surgery by two research assistants. The assessments included patient-rated wrist evaluation score (MacDermid, 1996), Disabilities of the Arm, Shoulder and Hand questionnaire (Gummesson et al., 2003), the 12-Item Short Form Health Survey (Ware et al., 1996), wrist range of motion (ROM) (Bashardoust Tajali et al., 2016) and grip strength assessment with an electronic hand dynamometer (MacDermid et al., 2001). Patients were excluded from ROM and grip strength analysis if they had a nonunion, were missing measurements or if they were lost to follow-up after 3 months after surgery.
Radiographic assessment
Scaphoid CT scans were performed at baseline to evaluate scaphoid morphology, displacement and to the assist in the diagnosis of arthritis. They were repeated at 6, 9, 12 and 16 weeks postoperatively to assess union. If patients failed to demonstrate union at the 16-week mark, timing of additional scans was based on the treating surgeon’s discretion. Evidence of union on CT imaging (GE Discovery 750 HD scanner (Milwaukee, WI, USA) (120 kV, 200 mA, 0.8 s rotation, 0.625 mm thick)) was defined as >50% of total cross-sectional area on sagittal view (Singh et al., 2005). We did not consider union to be present unless this threshold was met on CT scan, even if the patient was non-tender on physical examination. In addition, plain radiographs were performed at baseline, immediately postoperatively and at 6-month and 1-year follow-up appointments. Imaging was assessed by the principal investigator and a musculoskeletal radiologist.
Surgical technique
Proximal pole nonunions were approached dorsally, and waist nonunions were approached either palmarly or dorsally. The nonunion was debrided. Intraoperative assessment confirmed punctate bleeding of the proximal and distal scaphoid poles in all patients. Bone grafting was performed according to the patient randomization group, and additional cancellous graft was packed into both the distal and proximal poles. All cases were stabilized with two to three 1.6 mm (0.062″) diameter titanium, smooth K-wires cut below the skin. All patients were placed in a short-arm thumb spica cast postoperatively until union was achieved. K-wires were removed in the clinic under local anaesthetic. The 1,2-ICSRA VBG was harvested as described by Zaidemberg et al. (1991) through a dorsal approach, but we placed the 1,2-ICSRA graft palmarly as an interposition wedge bone graft for scaphoid waist nonunions with a humpback deformity. The pedicle had to be dissected to an approximate length of 15–20 mm to allow palmar placement (Ingari et al., 2019). For NVBG, a corticocancellous graft was obtained from the outer table of the iliac crest as described by Fernandez (1984). The cortical aspect of the bone graft was positioned palmarly and secured with K-wires.
Statistical methods
Primary outcomes included union incidence and time to union assessed by CT imaging. The secondary outcomes were complication incidences, ROM, grip strength and patient-reported outcomes. Student’s t-test was used to compare means between groups. Chi-squared testing was used to compare outcomes of bony union. A Cox regression analysis was used to control for confounding variables, such as smoking status.
Results
Forty-eight patients were enrolled in the study (Figure 1); 25 (20 men, five women) were randomized to the VBG group, and 23 (all men) were randomized to NVBG group. Overall, the two groups had similar demographics (Table 1); however, there were more smokers in the NVBG group (9/18 versus 4/20, p = 0.05). Three patients consented to surgery but never received an operation and were excluded from analysis. Intraoperatively, three patients from the VBG group and four patients from the NVBG group had intact stable cartilage caps. Consequently, they did not receive any bone grafting and instead underwent open reduction internal fixation with a single headless compression screw. Thus, 20 patients were finally included in the VBG group and 18 patients in the NVBG group. There was no crossover of patients between groups.
Patient demographic data.
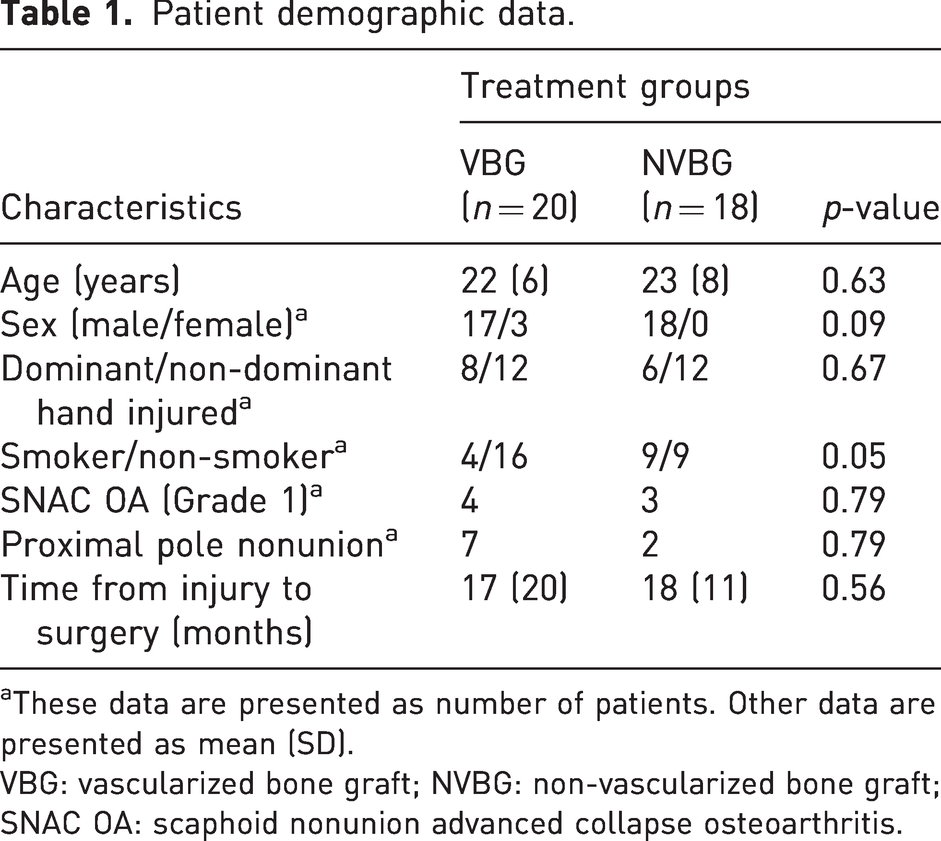
aThese data are presented as number of patients. Other data are presented as mean (SD).
VBG: vascularized bone graft; NVBG: non-vascularized bone graft; SNAC OA: scaphoid nonunion advanced collapse osteoarthritis.
Bone union
Overall, there were three nonunions at follow-up, one in VBG group and two in NVBG group, (p = 0.49). All three of these patients were active smokers at the time of surgery and experienced K-wire migration postoperatively. The time to union was similar between groups (VBG: 16 weeks (SD 22); NVBG: 17 weeks (SD 33)). Details are provided in Table 2. When smoking status was controlled for by using a Cox proportional hazards regression, a hazard ratio of 1.7 (95% confidence interval, 1.0 to 2.9) was reported for VBG (p = 0.045). This suggests that VBG were 72% more likely to achieve union compared with NVBG. Similarly, when surgery type was controlled for, a hazard ratio of 0.4 (95% confidence interval, 0.2 to 0.9) was reported for smokers, suggesting that smokers were 60% less likely to achieve union (p = 0.024).
Time to union (number of cases united at a given time interval).
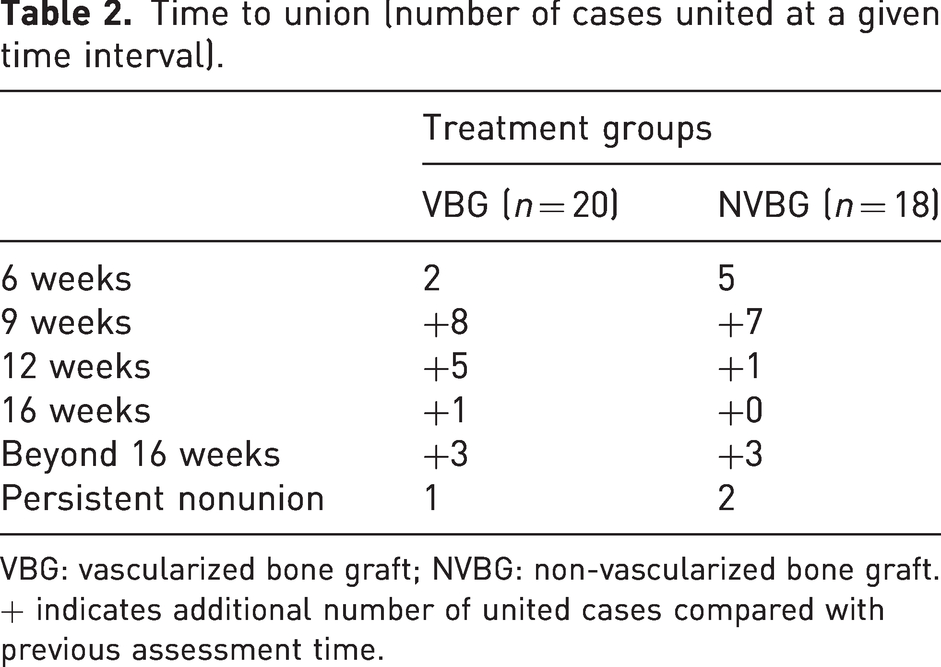
VBG: vascularized bone graft; NVBG: non-vascularized bone graft.
+ indicates additional number of united cases compared with previous assessment time.
Clinical outcomes
Besides the three patients with nonunion at follow-up, eight patients were lost to follow-up (four in each group), and four missed objective measurements (two in each group). There were no significant differences between the two groups in ROM, grip strength or patient-reported outcome measures (Tables 3 and 4).
Range of motion and grip strength.
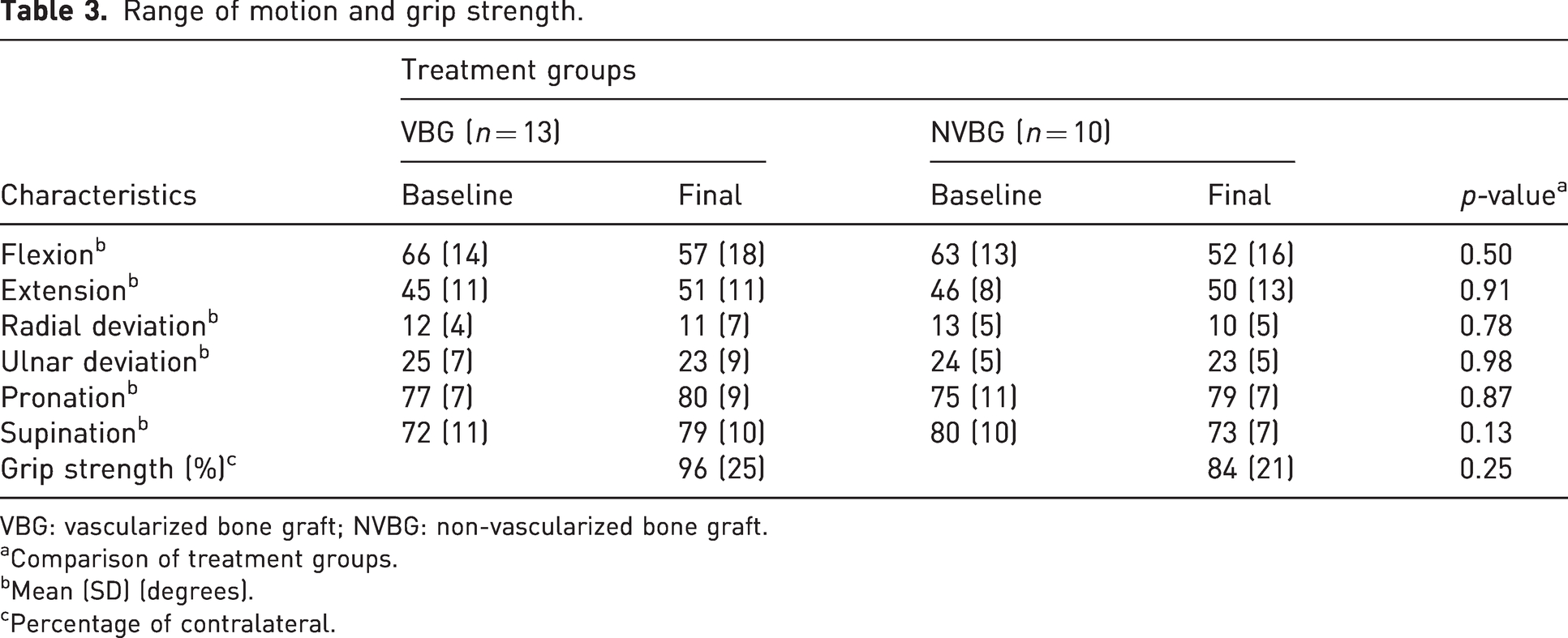
VBG: vascularized bone graft; NVBG: non-vascularized bone graft.
aComparison of treatment groups.
bMean (SD) (degrees).
cPercentage of contralateral.
Patient-reported outcome scores at 12 months.
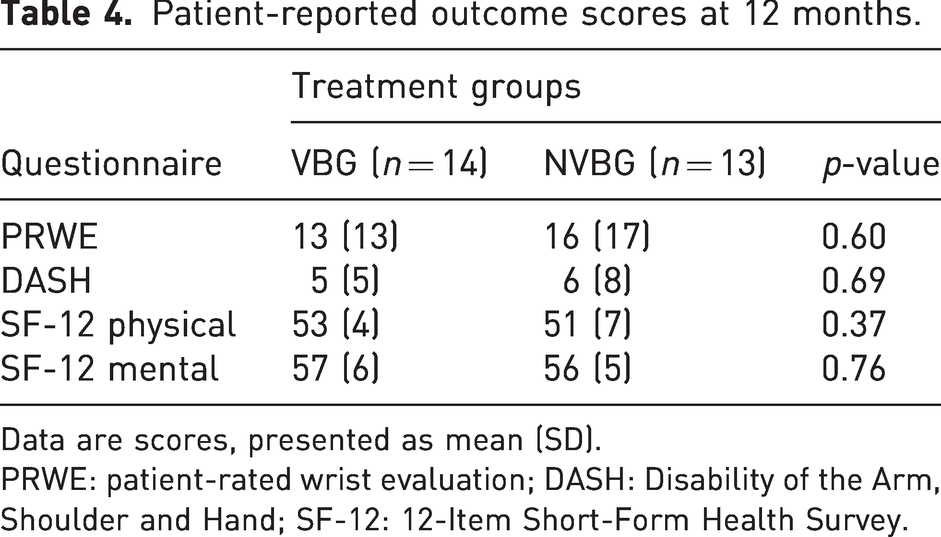
Data are scores, presented as mean (SD).
PRWE: patient-rated wrist evaluation; DASH: Disability of the Arm, Shoulder and Hand; SF-12: 12-Item Short-Form Health Survey.
Complications
Complication incidences were generally similar between groups, although the incidence of transient numbness postoperatively was significantly higher in the VBG group (Table 5). These were all cases in which a dorsoradial skin flap was elevated and the VBG graft was implanted palmarly. Five patients in the NVBG group and four from the VBG group experienced K-wire migration (p = 0.51). Three of these cases were the nonunions described above.
Complications.
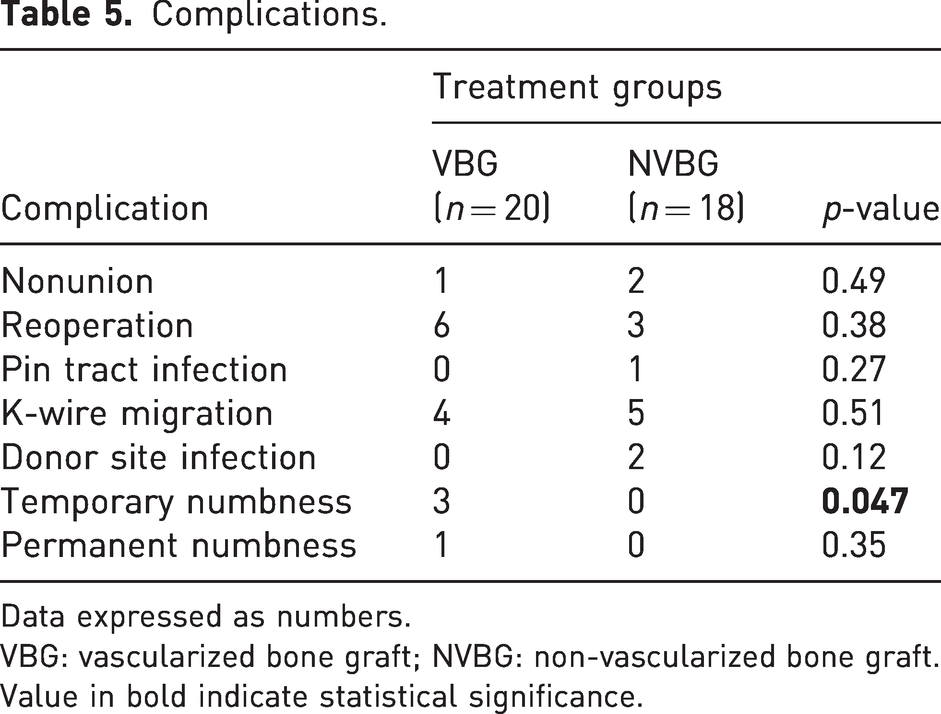
Data expressed as numbers.
VBG: vascularized bone graft; NVBG: non-vascularized bone graft.
Value in bold indicate statistical significance.
Six patients who received a VBG and three who received NVBG required a second operation (p = 0.33). One patient in the NVBG group underwent a repeat procedure for persistent scaphoid nonunion using an iliac crest graft from the contralateral side fixed with a headless screw. The other two patients accepted nonunion and preferred not to have a repeat procedure (either attempted revision surgery or salvage). Five patients required a return to the operating room for K-wire removal. Two patients from the NVBG group experienced donor site infection, both requiring hospitalization for intravenous antibiotics and incision and drainage. Additionally, one patient in the VBG group who was a professional American football player, was dissatisfied with postoperative ROM (flexion 40°, extension 45°) and underwent dorsal capsulectomy to improve wrist flexion.
Discussion
In this study of scaphoid nonunion without AVN treated with bone grafting and K-wire fixation, we obtained an overall union incidence of 35/38 with no significant difference in union incidence or time to union between the groups. All three nonunions occurred in smokers and in whom the K-wires had migrated. Our analysis showed that smokers were 60% less likely to achieve union.
The role of VBG in scaphoid nonunion remains controversial. Two prospective randomized controlled trials have been conducted on this topic. Braga-Silva et al. (2008), found that VBG and NVBG in patients with or without AVN had similar times to union (8 versus 9 weeks, respectively). However, the type of fixation used was not standardized (K-wires for VBG versus compression screw for NVBG). Conversely, Ribak et al. (2010) demonstrated that vascularized grafting was associated with higher union incidences (41/46 with VBG and 29/40 with NVBG) and faster time to union (10 weeks with VBG and 12 weeks with NVBG). Other studies report advantages of VBG over NVBG. Merrell et al. (2002) reported an advantage to VBG (88% union VBG versus 47% NVBG) in the setting of AVN. A meta-analysis revealed no significant difference in union incidence (88% NVBG versus 92% VBG) or time to union (14 weeks) (Pinder et al., 2015). Rancy et al. (2018) reported on 35 subjects with scaphoid nonunion treated with NVBG and compression screw fixation. Despite noting impaired vascularity in multiple patients, 33/35 of them achieved union by 12 weeks, and there was no correlation between impaired vascularity and union incidence or time to union.
The small sample size of our study does not permit clear assessment as to which procedure is superior. Thus, we could not confirm our hypothesis that VBG would result in more rapid and higher incidences of union in comparison with iliac crest bone grafting. Moreover, we could not assess potential benefits of VBG in cases with AVN, since these cases were excluded. Neither could we assess potential benefits in surgery for recurrent nonunion; however, we could determine that it is acceptable to consider a VBG as a primary procedure since there was no increased risk of complications.
The use of K-wires for fixation may be criticized. We decided to use K-wires to eliminate the method of fixation as a possible confounding factor. While headless compression screws may offer biomechanical advantages, nonunions with extensive bony absorption and cystic degeneration may not be amenable to headless compression screw fixation due to over-compression resulting in bony collapse. In a systematic review evaluating VBG in scaphoid nonunion, K-wire fixation had a higher union incidence (25%) compared with screw fixation and was associated with a shorter time to union by 7 weeks (Alluri et al., 2017). The authors hypothesized that this finding was secondary to impaired vascular inflow from larger diameter compression screws. Conversely, our study demonstrates some drawbacks of using K-wires. In nine cases the K-wires migrated, which possibly contributed to failure of union in three cases, and five cases required a return to the operating room for K-wire removal.
Limitations to our study include the small sample size, missing data and the imbalance of smokers and number of proximal pole nonunions between the two groups.
Footnotes
Acknowledgements
We would like to thank Steve Lu for his assistance with our statistical analysis.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this work was supported by the Internal Research Fund Grant from Department of Surgery, University of Western Ontario, and Lawson Health Research Institute.
Ethical approval
Ethical approval was obtained from the University of Western Ontario Research Ethics Board approval (REB# 13343).
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
ClinicalTrials.gov (NCT01419808).