
Abstract
Introduction
The Federation of European Societies for Surgery of the Hand (FESSH) was established in 1990 and not long after, an examination was introduced to determine the European standard for hand surgeons (FESSH White Book on Hand Surgery in Europe, EBHS, 2020). The examination was first held in Paris in 1996 with 38 candidates (Calcagni, 2013). The examination subsequently evolved into today's European Board of Hand Surgery (EBHS) examination through the combined efforts of FESSH and the Multidisciplinary Joint Committee (MJC) on Hand Surgery of the Union Européenne des Médecins Spécialistes (UEMS) (FESSH, 2023a).
This article, written by recently successful diplomates from various countries aims to provide an insider's perspective of the EBHS diploma examination for future candidates, set against the context of different hand surgery training programmes across Europe.
The EBHS examination
The EBHS examination is held once a year. Individual entry requirements are strict and require a minimum level of hand and wrist surgery experience with the detailed criteria outlined on the FESSH website (Muir et al., 2018). Candidates are advised to study the application criteria carefully and make every effort to submit the correct documentation to avoid a prolonged correspondence with the examination board. In particular, the EBHS consolidation sheet of surgical procedures will take some time to prepare.
The examination is divided into three components. The written part takes place mid-March via an online web-based platform and a Zoom invigilator link. Consisting of 60 multiple choice questions (MCQs) with five parts each, candidates are negatively marking for incorrect answers. The MCQs are written by the exam board and almost all are freshly constructed every year. The second and third parts are held in conjunction with the annual FESSH congress. The practical examination is a 30-minute session, during which a practical skill is assessed. The oral examination follows and is held over 2 days. It is divided into three ‘themed' vivas of 30 minutes, each covering three different clinical cases/scenarios. The viva themes are (1) acute trauma, (2) reconstructive surgery, including reconstructive surgery after trauma and degenerative change (e.g. contractures, non-union, osteoarthritis) and (3) miscellaneous (e.g. Dupuytren's, Kienböck's tumours, congenital, nerve compressions). Each clinical case is accompanied by a brief description of the scenario, a radiograph or photograph, and an opening/starter question. While the viva should proceed like all post-graduate examinations, with logical progress through the history, examination and management options, presenting appropriate evidence is required for candidates to obtain the highest scores. Passing the oral examination requires breadth of knowledge and sensible judgement (incorporating practical clinical experience) of common hand problems. It is important to mention all salient points on the topic, avoid major errors or dangerous practices, and to take a methodical approach to answering questions and as far as possible, to do so without prompting from the examiners. The examination website contains the marking descriptors for the orals, which will help understand how the ideal answer might be structured and what the examiners are looking for.
If the oral component is failed, a resit is currently possible for up to 2 years without needing to retake the written exam. However, the structure of the examination is under constant scrutiny and refinement by bodies such as the Council for European Specialists Medical Assessment (CESMA) and the above information is subject to change. Changes will always be reflected on the exam web site.
Preparing for and passing the EBHS: candidates’ perspectives
All the authors passed the examination in 2022, and in this article they hope to offer some advice and encouragement to future candidates. The first thing to mention is that the preparation should be seen as ‘a marathon and not a sprint’, particularly as most candidates will be undertaking full time clinical work. In other words, brief but regular revision sessions are the optimal way to maintain momentum rather than taking protracted time off. Our cohort started studying 4–6 months prior to the MCQs.
Multiple reference materials are available to aid preparation; regularly alternating between these is the key to prevent boredom. Many textbooks exist although Green's operative hand surgery (Wolfe et al., 2022) remains our gold-standard reference to consolidate the fundamentals. It is unlikely that candidates have time to read the book cover-to-cover, but the summary boxes at the end of each chapter provide a useful precis of key facts and concepts, and detailed reading can then be reserved for less familiar topics. Orthopaedic surgeons will invariably need to focus on the ‘soft tissue’ topics (e.g. burns, flaps, reconstruction), whereas plastic surgeons should concentrate on the ‘bone and joint’ topics (e.g. wrist, scaphoid, arthroscopy). It is beneficial to make notes or flashcards from the outset as these can be taken into the rest areas for last minute revision between viva sessions.
Popular websites such as Orthobullets (www.orthobullets.com), Radiopaedia (www.radiopaedia.org/) and MyOrthoEvidence (www.myorthoevidence.com) are helpful, alongside the many excellent recent webinars and online resources (e.g. the Pulvertaft Webinars – @pulvertaftvideos5886 (www.youtube.com) and others). These resources are ideal when tired after work, as watching a webinar is a great ‘passive’ way to absorb information, particularly for the viva. For the MCQs, various practice question banks exist via the Journal of Hand Surgery European (JHSE) and American Society for Surgery of the Hand (ASSH) websites. Practicing timed mock examinations is helpful, particularly closer to the real examination. The EBHS website also offers a small question bank that can be purchased and is useful to sit as a mock timed test. For those that prefer more structured teaching, European courses such as the FESSH Academy run annually, as do those led by individual national hand surgery organizations, such as the Young Hand Surgeons mock examination and preparation course in Switzerland and the British Society for Surgery of the Hand (BSSH) Instructional courses in the United Kingdom.
For the viva component, a study group with fellow candidates is highly recommended to help practice questioning and answering techniques and to share knowledge, as each surgeon invariably has different experiences and interests. In addition, during personal studying it is helpful to prepare a 1–2 minute ‘script’ for every topic in the curriculum and then reading them out loud. These can be supplemented by audio or video recordings that can then be played back during commutes to work. This is especially helpful for candidates who are less confident with spoken English. It is advisable to start early with tutorials and mock vivas with multiple senior consultants, who will each have their unique viva techniques as these are invaluable in gaining confidence and regurgitating facts, in case panic sets in and you need to think on your feet. This will not be enjoyable to start with, but will undoubtedly make the ‘real thing’ feel far more routine and less of a shock.
Collectively, the feeling was that the MCQ examination was difficult, particularly with negative marking, as a risk-benefit judgement is required for each question based upon one’s relative confidence in the topic. Questions often seek knowledge of specific facts, so a good technique is to rapidly advance through the test answering only those for which you confidently know the response, and to then go back through for a second time, answering only those for which a confident educated guess can be made. If you are uncertain about an answer, then it is best to leave the response blank, so you do not lose points.
The viva was felt to be more balanced, with generally friendly and polite examiners who, while often remaining ‘poker faced’ as in all professional examinations, did help clarify language issues and attempted to extract as much information from candidates to help them the score maximum points. The viva was conducted in the manner of a ‘case discussion among colleagues’ rather than an interrogation. Having multiple stations also offered the opportunity for ‘good’ stations to compensate for those that went badly (which will inevitably happen). With vivas spread across two days, the waiting between stations was the most nerve-wracking part. During these gaps, some preferred to study their own notes, while others went to nearby cafes to relax and refresh before their next timetabled session.
National hand examinations and training differences across Europe
The EBHS diploma has the obvious advantage of being recognized all across Europe. However, national equivalents do exist, which may have more standing in individual nations. We are not able to compare all national hand surgery examinations across the world with the EBHS diploma model but wish to highlight some examples from the authors who originated from the following countries.
France
The hand surgery pathway requires 5 years of training (in plastic/orthopaedic/paediatric surgery, or a mix), of which two are dedicated to hand surgery. A microsurgery diploma (1 year university-led diploma with a written and practical examination) is required, alongside a national hand and wrist surgery diploma (2-year programme, with vivas and a written examination). Following this, a 2-year post-residency senior surgeon post in a hand unit is required before a panel of senior surgeons scrutinize candidates' portfolios and confer the title of hand surgeon. While this title places surgeons in a select cohort of around 600 surgeons, this qualification is not mandatory to practice hand surgery (CFECM, 2023). Very few French surgeons go on to take the EBHS diploma; since its inception, merely 30 candidates have been awarded this additional qualification.
Germany
After 6 years of training in a surgical speciality, surgeons have to complete a further 3 years of training in hand surgery. Additionally, a logbook with minimum numbers of specific operations must be completed prior to taking the national oral hand surgery examination and becoming an accredited German hand surgeon. Compared with the EBHS diploma, completion of the national hand surgery examination is more common among surgeons in Germany. In contrast, when a German surgeon takes the EBHS exam, this is usually due to a specific sub-specialist interest in hand surgery and a desire to advance in the field. The EBHS diploma is well recognized within the German hand surgery community, with candidates choosing to complete this to both demonstrate consolidation of their knowledge, and to use this prestigious qualification to improve their prospects when applying for hand surgery posts.
Netherlands
Hand surgery can be practiced by surgeons trained in plastic, orthopaedic or general (trauma) surgery. Each have their own specialist training programme, allowing for later sub-specialization in hand surgery. Since 2014, the Dutch Society for Hand Surgery (Nederlandse Vereniging voor Handchirurgie, NVvH) has been developing its official criteria for sub-specialization in hand surgery, due to commence in 2023. International certifications – such as the EBHS diploma – are intended to become a vital part of the Dutch certification. Candidates therefore chose to complete the diploma as it is considered a key qualification for those wishing to be recognized as a sub-specialist in hand surgery.
Switzerland
Hand surgery has existed as a sub-speciality since 1988, being ultimately recognized as an independent speciality in 2015 (SSCM, 2023; Vögelin, 2019). Training lasts at least 6 years, comprising 2 to 3 years of general, orthopaedic or plastic surgery, and 3 to 4 years in a hand surgery unit. Since 2007, there has been no national examination, and the EBHS diploma is required as a speciality exam. Applications need to be sent to the head of the Swiss Hand Surgery Society, which are then assessed for eligibility. The number of successful EBHS diplomates in recent years has tripled, now accounting for around 20% of all EBHS diploma candidates each year.
United Kingdom
Following its inception in 2007, the BSSH's postgraduate British Diploma in Hand Surgery adopts a ‘distributed learning’ approach via a bank of experienced hand surgeon tutors. The programme consists of approximately 1200 hours of learning and assessment, including completion of a signed booklet of tutorials across eight modules, an operative video, a clinical algorithm, a review article and attendance at relevant educational events. Once completed, candidates sit the written and viva examinations. While a growing number complete the British diploma, relatively few sit the EBHS examination, although both are considered equivalent for consultant applications. Common reasons UK surgeons sit the EBHS are the reduced additional workload (i.e. no coursework, overlapping curriculum) and helpful timing of the examination (i.e. completion during the academic year of a fellowship, rather than the BSSH diploma that often takes place early in the next post).
The key differences between the various examinations are summarized in Table 1.
Comparison of various national examinations with the EBHS.
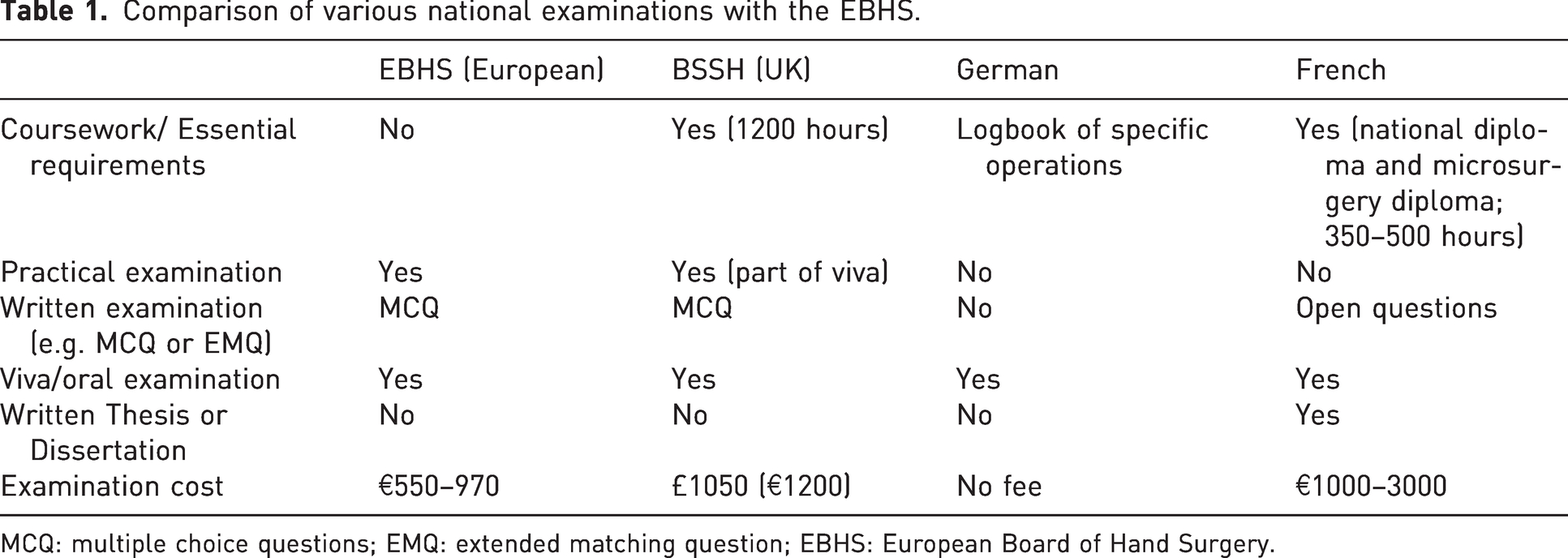
MCQ: multiple choice questions; EMQ: extended matching question; EBHS: European Board of Hand Surgery.
EBHS diploma statistics from 2020 to 2022
Over the past 3 years, the EBHS diploma examination has attracted between 161 and 171 applicants annually. Of those, 35 to 45 (20–30%) were rejected. Between 12 and 22 candidates (14–33%) failed the written MCQ. Seventeen to 20 candidates who previously failed the oral examination re-sat only the oral part. In total, 65 to 100 candidates sat the oral examination, of whom seven to 22 failed (12–28%). Overall, 58 to 78 candidates passed all components, which represents 50–57% of all accepted applications.
The examination has attracted candidates from both Europe and beyond, including those practicing in Australia, Argentina, Egypt, India, Israel, Pakistan, UAE, Ukraine, Russia, Saudi Arabia, South Africa and Yemen. During this 3-year period, those from Germany, Switzerland and the UK comprised the majority of both candidates and successful diplomates. Of these three nations, Switzerland had the lowest MCQ examination failure rate and the UK the lowest viva examination failure rate. The least represented countries (i.e. those with at least one candidate every year) were Czech Republic, Poland and Turkey. Some European countries were not represented every year, including Finland, Greece, Hungary, Ireland, Luxembourg, Norway, Romania, Sweden.
In the most recent 2022 sitting, 108 candidates from 14 different countries sat the virtual written examination on 18 March 2022. Seventy-seven candidates passed the written and proceeded to sit the viva and practical examinations, which were held over 3 days at the newly refurbished Royal College of Surgeons of England, London, over the Queen’s Platinum Jubilee Weekend on 3–5 June 2022. After 3 days of rigorous quizzing from 33 examiners across Europe, 65 candidates passed and were awarded their diplomas before going on to enjoy the FESSH–IFSSH meeting in London (FESSH, 2023b).
Conclusion
The EBHS diploma examination continues to grow in popularity and standing among the European hand surgeon community, playing an important role in credentialization and standard setting alongside the individual national hand surgery examinations. Its pan-European status also has the additional benefit of promoting the growth of hand surgeon networks across the continent. Holding the exam prior to the annual FESSH meeting allows for further networking opportunities. Over the years, candidates have made long-lasting connections with colleagues, going on to build strong friendships and academic collaborations. As an exit examination, the EBHS diploma is intended to maintain standard that is at post-training/early consultant level, with most trainees sitting this toward the end of a dedicated hand surgery fellowship.
A downside of the diploma – like any sub-specialist qualification – is that it requires a significant amount of work, which can have an adverse impact on work–life balance at a challenging time towards the end a young surgeon's career (Galloway et al., 2022; Ruparell et al., 2022). However, the lack of coursework (unlike the UK hand diploma) does help ‘compartmentalize' workload to a limited period, thereby mitigating the additional coursework workload of some of the national exams.
The authors can testify that while the revision process and examination were undoubtedly tough, successfully coming through the other side was a rewarding experience through which we have all gained confidence from our success, valuable credentials that have undoubtedly benefited our careers, and built an international network of new friends and colleagues. We encourage budding hand surgeons to consider completing the diploma and we wish future candidates the very best of luck!
Footnotes
Acknowledgements
Dr Ana Carreño, Kaplan Institute, Hospital Clinic, Universitat de Barcelona, Barcelona, Spain, for her contribution and revision. Dr Lindsay Muir Manchester Hand Centre, Salford Royal NHS Foundation Trust, Salford, UK, for the data and information about EBHS. The administration team at FESSH for their work and assistance with data and information.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.