
Abstract
The scaphoid is the largest of the carpal bones, articulating with both proximal and distal carpal rows. If scaphoid fractures are not appropriately diagnosed and treated, there is a risk of nonunion, osteonecrosis and degenerative arthritis. Operative management of the scaphoid fracture is primarily determined by the fracture location and amount of displacement. There is increased momentum for dual screw fixation constructs, intended to provide greater stability and reduce the risk of nonunion. Our current practice is to utilize two screws without graft as a first-line treatment for scaphoid nonunion with or without humpback deformity and cyst formation. This review will discuss the management of acute scaphoid fractures and the treatment of nonunion.
Introduction
The scaphoid is the most frequently fractured carpal bone (Wolfe et al., 2022), accounting for 60% to 90% of all carpal fractures. The proximal pole is attached to the lunate by the scapholunate ligament and tends to be pulled into extension by the proximal carpal row (Figure 1). The distal pole is firmly attached to the trapezium and trapezoid. The extrinsic carpal ligaments, the dorsal intercarpal ligament and the radioscaphocapitate ligament further secure the distal portion of the bone. The scaphoid is often described as having a tenuous blood supply due to the single primary irrigation, which enters the scaphoid in a retrograde direction. There is a high risk of blood supply disruption in scaphoid fracture, especially in more proximal fracture patterns. Although vascularity may play a role in nonunion, the force vectors across the scaphoid during motion also interfere with healing. In our practice, delayed union is defined as failure to unite at 3 months, and nonunion is defined as failure to unite at 6 months. More proximal fractures have smaller proximal fragments that are not stabilized by articulation with the capitate or the ligaments of the scaphotrapeziotrapezoid (STT) joint. The extension moment of the proximal carpal row displaces the proximal fracture fragment, making the distal fragment appear in relative flexion. This is often termed a ‘humpback’ deformity of the scaphoid. If scaphoid fractures are not appropriately diagnosed and treated, they are at risk for nonunion, osteonecrosis and degenerative arthritis (Wolfe et al., 2022). This review will discuss the management of acute scaphoid fractures and the treatment of nonunion.
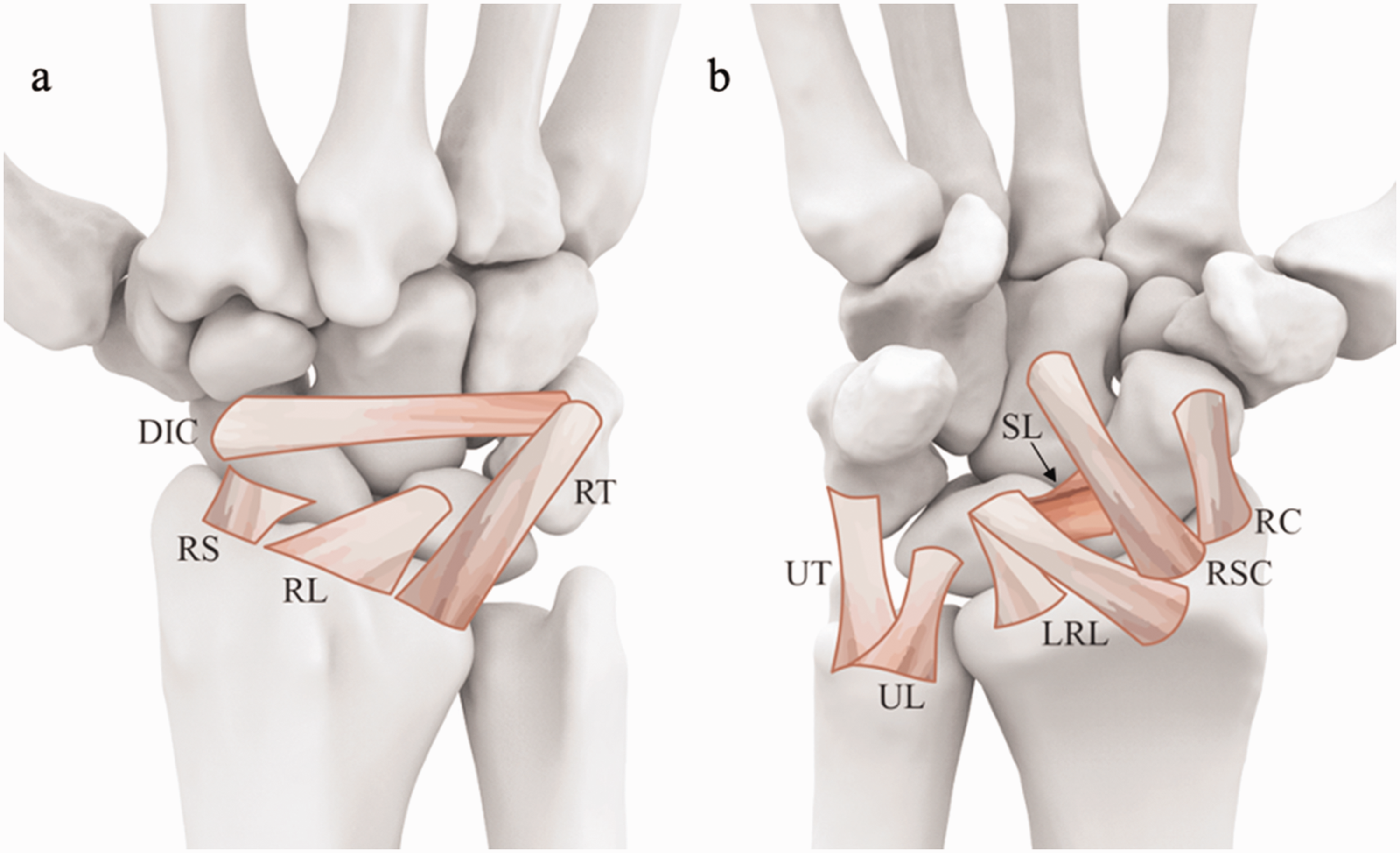
(a) Anatomic depiction of dorsal extrinsic ligaments of the wrist and (b) volar extrinsic and intrinsic ligaments of the wrist.
Acute fractures
Diagnosis
Most scaphoid fractures are detected on plain radiography. Standard views typically include posteroanterior (PA), lateral and oblique views. These are often augmented with a ‘scaphoid view’, which is a PA radiograph with the wrist in ulnar deviation and 20° to 30° of supination. Unfortunately, radiography in the acute period may only detect fractures in approximately 90% of cases with a high false-negatives, reported in up to 20% of cases (Leslie and Dickson, 1981; Waeckerle, 1987). Traditionally, a clinically suspected scaphoid fracture with negative initial radiographs was treated with immobilization and repeat imaging in 10 to 14 days (Wolfe et al., 2022).
Alternatively, magnetic resonance imaging (MRI) can be utilized in the acute phase to detect occult fractures with a sensitivity of 88% to 100% and a specificity value approaching 100% (Mallee et al., 2015). Specifically, a T2 MRI scan with fat suppression is sensitive for demonstrating marrow oedema. Diagnostic accuracy can be improved by the addition of a high-resolution T1-weighted series. This allows for better visualization of the fracture line to differentiate between a true fracture and a bony contusion (Amrami et al., 2019). Our preference is for three planes of proton density sequence and an inversion recovery sequence in the coronal plane for identifying an acute scaphoid fracture.
Earlier evaluation with MRI can provide a more expeditious diagnosis, which spares patients the loss of productivity associated with 2 weeks of immobilization. It has the additional benefit of identifying other ligamentous injuries that may be present (Sabbagh et al., 2019). In a prospective case series, Dean et al. (2021) reported that 13% of negative radiographs were found to have a scaphoid fracture on MRI examination.
Nonoperative treatment
Cast immobilization is a well-described treatment for non-displaced or minimally displaced acute scaphoid fractures. Overall, there is a high rate of union, but this rate is substantially lower than the union rate for other common fractures, such as the distal radius. Healing time can be relatively short, averaging approximately 7 weeks. Cystic resorption at the fracture site and delayed casting have been shown to increase the time to union (Grewal et al., 2015).
Historically, surgeons thought extended immobilization was required for adequate fracture treatment and commonly utilized an above-elbow thumb spica cast. More recently, surgeons have favoured short-arm thumb spica casts. However, a current evaluation of the literature shows that neither the length of the cast nor the presence of thumb immobilization has a clinically relevant effect on union rates in acute scaphoid fractures (Siotos et al., 2022).
The multicentre randomized SWIFFT trial reported on over 400 cases of acute presentation of scaphoid wrist fracture (Dias et al., 2020). Although rates of full union and almost union were higher in the surgery group compared to the cast immobilization group, they did not reach the level of significance. There is emerging evidence to suggest that casting is a successful treatment for subacute scaphoid fractures with a union rate of 82%. When excluding patients with diabetes, combination and/or a humpback deformity, the union rate for casting in subacute fractures can be as high as 96% (Grewal et al., 2016).
Operative fixation
Operative management of scaphoid fractures is primarily determined by the fracture location and amount of displacement. Distal pole fractures and nondisplaced scaphoid waist fractures are often treated nonoperatively. Indications for operative treatment include open fractures, displaced waist fractures and proximal pole fractures. Operative treatment is particularly important for proximal pole fractures due to the potential for articular involvement and the tenuous blood supply, which increases the risk of nonunion (Wolfe et al., 2022).
A variety of fixation methods can be used, including Kirschner wires (K-wire), screws, staples and plates. K-wires are simplistic in application but provide no compression and minimal stability, which necessitates postoperative immobilization. The most common fixation option is headless compression screws, which provide a stable construct, the ability to bury the head of the screw and compression across the fracture (Suh and Grewal, 2018). Although most scaphoid fractures can be treated from a volar, transtrapezial or direct dorsal approach, proximal fractures are preferentially treated with dorsally inserted screws and distal fractures with volarly inserted screws. Limited open or percutaneous approaches are typically employed from a dorsal or volar approach in fractures treated without bone graft.
Dual screw fixation has received increased attention in recent years. This method of fixation is intended to provide greater stability and rotational control and reduce the risk of nonunion (Figure 2). Indeed, this advantage is especially important in unstable displaced fracture patterns. There is established understanding for the importance of stability and rotational control in fracture healing. These factors are especially crucial in scaphoid fracture repair given the rotational forces across the proximal carpal row during wrist motion (Stoesser et al., 2017). Clinical outcomes have been satisfactory for dual screw fixation in cases of primary fractures and nonunion (Garcia et al., 2014; DiPrinzio et al., 2022). In 2017, results by Quadlbauer et al. (2017) reported higher union rates in scaphoid fractures fixed with two screws compared to fractures fixed with one screw. Biomechanical evidence has demonstrated efficacy for dual screw fixation with greater stiffness, torsional control and energy absorption compared to single screw fixation (Mandaleson et al., 2018; Nicholson et al., 2021). The planar orientation of dual screws is influenced by fracture pattern, the anatomy and access. Sagittal plane alignment of screws could be appropriate during antegrade insertion and coronal plane alignment could be appropriate during retrograde insertion due to scaphoid morphology and the surrounding structures. Planar orientation of dual screws was studied by Surke et al. (2021) with results demonstrating no difference in stability between dual screws aligned in the sagittal and coronal planes. In aggregate, the literature displays satisfactory clinical outcomes for dual screw fixation of acute scaphoid fractures and scaphoid nonunion. In addition, there is clear biomechanical evidence for improved stability and rotational control in dual screw constructs compared to single screw constructs.
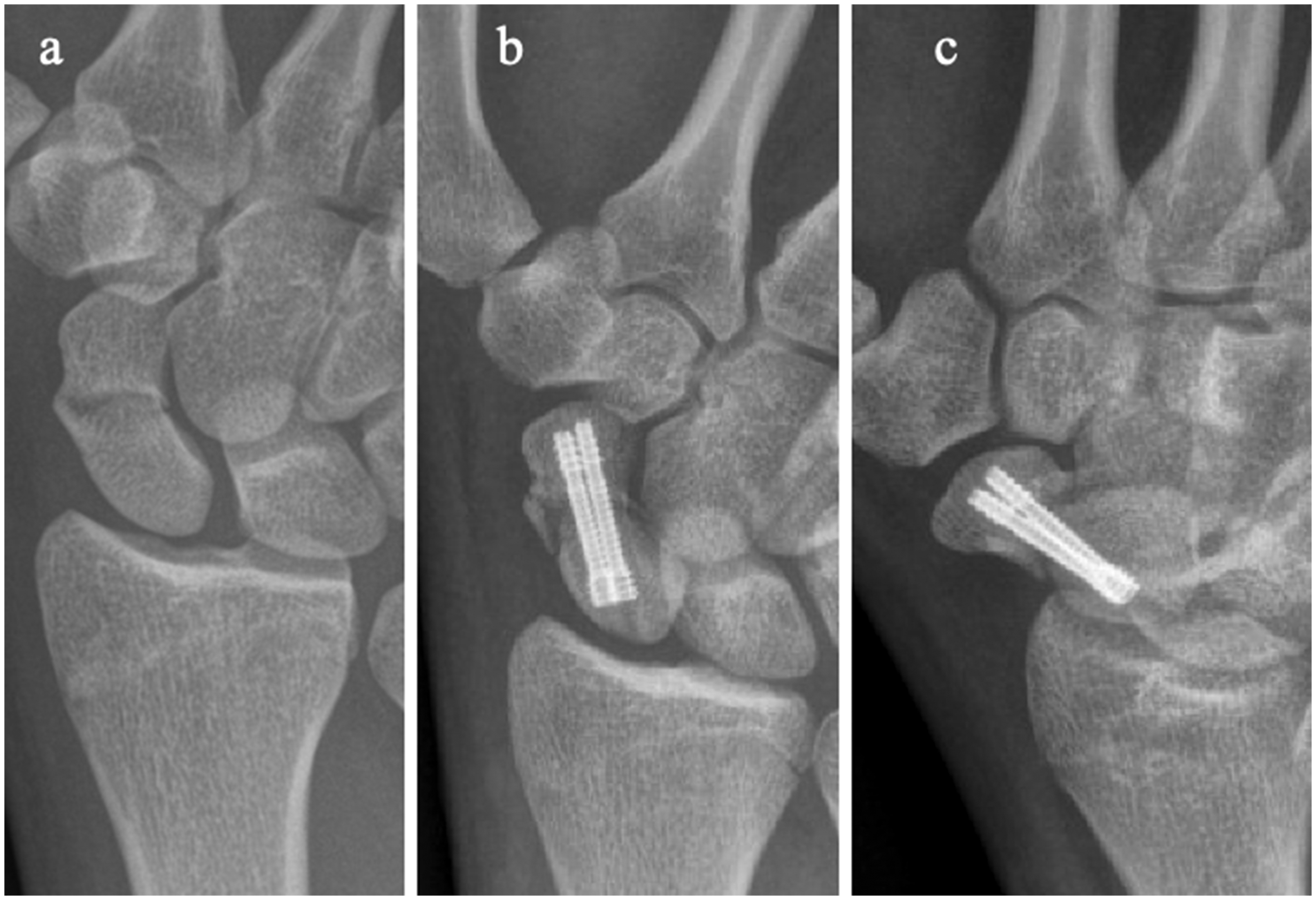
(a) Radiography demonstrating acute scaphoid fracture with comminution of the waist, treated with (b, c) dual screw fixation.
Staple fixation is an option in cases with a short proximal or distal fragment, where screw fixation may not adequately capture the fragment. Staples are relatively simple to apply, and novel devices have the capability for improved compression across the fracture site (De Vitis et al., 2019). A recent systematic review by Dunn et al. (2017) concluded that staple fixation for scaphoid fractures yielded high rates of union and low rates of complication in a heterogenous series of acute fractures and delayed or nonunion. The authors noted complications after screw fixation due to technical errors, such as screw prominence, and suggested that the risk of technical error may be mitigated in staple fixation due to the simplicity of implantation.
Plate and screw constructs provide stable fixation for fractures with extensive comminution and in cases of nonunion. The application of plates requires more extensive exposure, which can compromise blood supply. Hardware prominence is a concern, especially with wrist flexion and the potential for flexor carpi radialis tendinitis. Reports describe satisfactory clinical outcomes though rates of hardware complication are concerning (Dodds et al., 2018; Mehling et al., 2019).
Nonunion
Diagnosis of avascular necrosis
Scaphoid nonunion has been reported in 15.5% of scaphoid fractures (Zura et al., 2016). The tenuous vascular supply and frequency of delayed diagnosis contribute to scaphoid nonunion. There is ongoing controversy regarding the diagnosis of avascular necrosis of the scaphoid. Current diagnostic options include radiography, enhanced and unenhanced MRI, histological examination and intraoperative punctate bleeding (Figure 3). Although there is no gold standard criteria for imaging diagnosis, intraoperative identification of punctate bleeding of the proximal pole was the standard established by Green (Higgins and Giladi, 2021). The literature displays conflicting evidence for the diagnostic efficacy of commonly utilized methods.

(a) Radiography and (b) magnetic resonance imaging of scaphoid nonunion with cyst formation treated with (c, d) bone graft and dual screw fixation.
Vascularized and non-vascularized bone graft
Discussions on the treatment of scaphoid nonunion are rife with controversy, including the use of a vascularized versus non-vascularized graft, the harvest site of the graft and the fixation technique. A benefit of vascularized bone graft is the potential for new vascular channels to sprout in the avascular bone. Theoretically, this would be an ideal option for avascular necrosis of the scaphoid. A literature review by Duncumb et al. (2022) revealed that there was no difference in union rates between vascularized and non-vascularized bone graft for the treatment of scaphoid nonunion. The aggregated data demonstrated that 90% of the cases with vascularized bone graft had evidence of avascular necrosis, while only 2% of the cases with non-vascularized bone graft had evidence of avascular necrosis. Goyal et al. (2013) performed a prospective randomized series comparing iliac crest bone graft to non-vascularized distal radius grafts when used in cases of scaphoid nonunion. At a minimum of 3 years follow-up, there were no differences between the groups for wrist range of motion, functional scores and union rates. Notably, the iliac crest bone graft group had a considerable incidence of donor sight morbidity. In their review of management of scaphoid nonunion, Ferguson et al. (2016) reported that rates of avascular necrosis were higher after vascularized bone graft (74%) compared to those after non-vascularized bone graft (62%). The authors reported that rates were highly variable with a myriad of factors contributing, importantly noting the lack of consistent reporting. Graft shape is also a consideration due to the force vectors across the scaphoid, which may hinder union. Biomechanical data demonstrate that longitudinally oriented strut grafting has greater resistance to torsional forces compared to wedge grafts (Gire et al., 2020).
Graft-less fixation
There is evidence that surgical treatment of scaphoid nonunion does not require bone graft. Vanhees et al. (2017) describe healing in 15 of 16 patients with scaphoid nonunion treated with a single percutaneous screw. Slade et al. (2003) reported a healing rate of 100% across 15 cases of scaphoid nonunion treated from a dorsal approach without graft. Radford et al. (1990) reported no difference in union rates when comparing scaphoid nonunion cases treated with graft to cases treated without graft.
Overall, the lack of compelling evidence for the use of bone graft and for the superiority of one graft type indicates that graft-less fixation of nonunion is a viable option. Our current choice as first-line treatment of scaphoid nonunion is two screws without bone graft for cases with and cases without humpback deformity and cyst formation.
Surgical technique
Many techniques are described to achieve reduction and fixation of the scaphoid. We hold the patient’s thumb between our non-dominant index and middle finger. The ring finger facilitates reduction by applying a dorsally directed force to the distal pole of the scaphoid. Flexing the wrist provides access to the proximal pole so the guide wire trajectory is co-planar with the axis the scaphoid (Figure 4). The guide wires are inserted into the proximal fragment. Reduction of the humpback deformity is attained by the concurrent action of wrist extension and the dorsally directed force applied by the surgeon’s ring finger. The wires are advanced across the fracture site, securing reduction. Headless screws are implanted in standard fashion. In our hands, surgical fixation is indicated acutely in the presence of displacement. In non-displaced fractures that have been treated conservatively, surgical fixation is indicated after approximately 6 weeks without evidence of sufficient healing and continued symptoms.
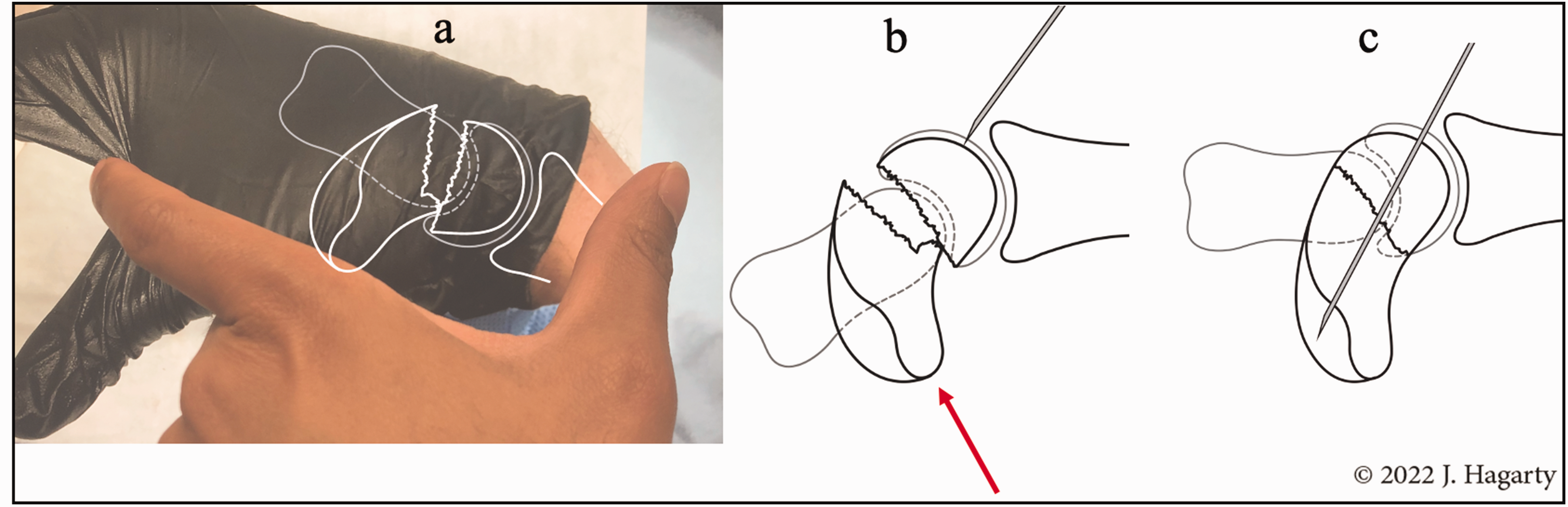
Graphical sequence of preferred surgical technique for reduction and fixation of scaphoid waist fracture with humpback deformity. (a) The surgeon flexes the wrist, which provides access to the proximal pole of the scaphoid for wire insertion, (b) then applies a dorsally directed force to the distal scaphoid (arrow) and (c) The wire is advanced across the fracture as the wrist is extended.
Conclusion
Operative management of the scaphoid fracture is primarily determined by the fracture location and amount of displacement. There is increased momentum for dual screw fixation constructs, intended to provide greater stability and reduce the risk of nonunion. The planar orientation of these screws is influenced by fracture pattern, the anatomy and access. Our current practice is to utilize two screws without graft as a first-line treatment for scaphoid nonunion with or without humpback deformity and cyst formation.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: RRLG declares relationships with Skeletal Dynamics, Trice/Tenex, BioTissue and Innomed. The remaining authors declare no conflicts of interest.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.