
Abstract

Dear Editor,
Congenital constriction band syndrome (CBS) can be characterized by the presence of a constriction band, lymph oedema, acrosyndactyly or amputation. Previous studies have indicated that structures proximal to a band in affected digits are usually normal (Burgess, 1991; Miura, 1984; Ogino and Saitou, 1987). However, a recent study showed that 30% of hands with amputated digits secondary to CBS demonstrated metacarpal hypoplasia (Satake et al., 2012). It remains uncertain as to whether the metacarpal hypoplasia existed at birth or developed gradually during growth. In this study, we investigated the incidence of metacarpal hypoplasia using quantitative measurement based on preoperative radiographic findings, as well as to determine whether the incidence of metacarpal hypoplasia of the amputated digits changed postoperatively in patients with CBS.
The medical records of 82 fingers of 26 hands in 17 patients with CBS who had undergone surgery and were subsequently followed for more than 5 years, were examined. Informed consent was obtained from the patients and their family before enrolment in this study. The study was approved by the Institutional Review Board of the university hospital (No. 322-20) and performed in compliance with the Declaration of Helsinki. Inclusion criteria included: (1) the presence of a constriction band, acrosyndactyly, amputation or lymphedema affecting the finger; (2) the corresponding finger of the contralateral hand was normal; and (3) there was no constriction band lesion on the upper limb proximal to the affected hand. Bilaterally affected hand or upper limbs where there were bands proximal to the affected hand were excluded. Of the 82 fingers, 29 fingers of 15 hands in 11 patients were eligible for inclusion in the study as follows. The mean age of the patients was 11 months (range 3–25), mean duration of the postoperative follow-up was 9.3 years (range 5–16) and mean age at the last observation was 10.3 years (range 6–17).The metacarpal area of the 29 affected fingers was measured using image-J (National Institutes of Health, Bethesda, MD, USA) based on the radiographic findings, and the ratio to the area of the healthy contralateral side was calculated (Figure 1). Metacarpals with a ratio of less than 90% of the healthy side were defined as hypoplastic.
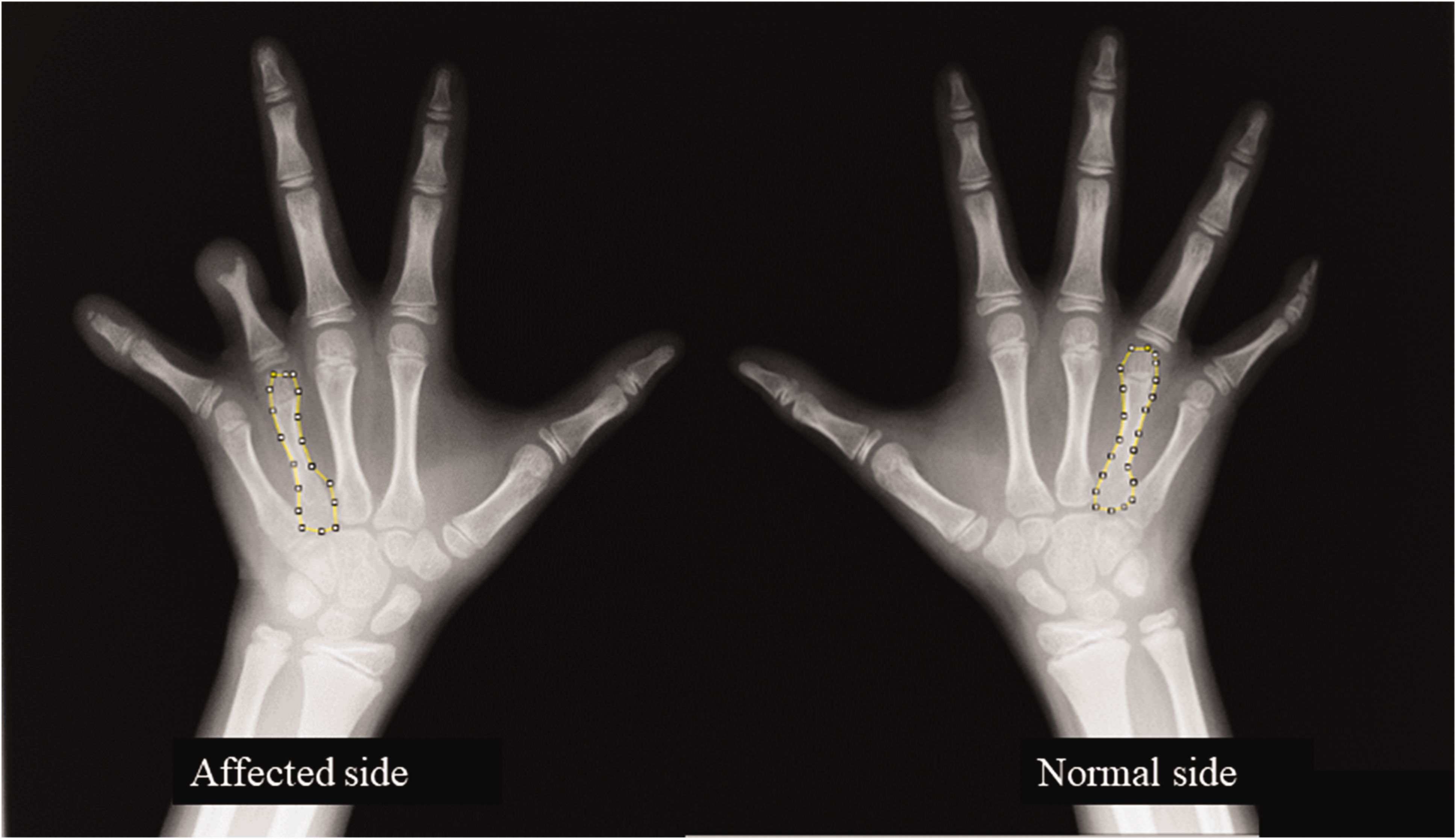
Quantitative evaluation of metacarpal area. The metacarpal area of the affected finger and the contralateral normal finger was quantitatively measured using Image-J. A metacarpal for which the area was 90% or less than that in the healthy side was defined as hypoplastic.
Our analysis revealed metacarpal hypoplasia proximal to an affected digit in 10 of 29 (35%) fingers based on the preoperative radiographic findings for patients with CBS. Evaluation based on the last postoperative follow-up revealed that eight (28%) of 29 fingers demonstrated metacarpal hypoplasia. In five (26%) of 19 fingers without metacarpal hypoplasia as a preoperative finding, metacarpal hypoplasia was subsequently identified at the last follow-up. Conversely, seven (70%) of 10 fingers with preoperative metacarpal hypoplasia did not demonstrate hypoplastic change at the last postoperative follow-up, while metacarpal hypoplasia remained in the other three fingers.
From this study, we also demonstrated that hypoplastic changes in the metacarpals in fingers affected with CBS may improve postoperatively during growth, although the aetiology of those changes remains unknown. The ratio of the metacarpal area of normal digits on the affected hand to those on the contralateral unaffected hand was more than 90% at the preoperative and last evaluation in all cases. We therefore consider that the normal fingers on the affected hand might not demonstrate any metacarpal hypoplasia. We believe that these findings provide information regarding the unique characteristics of digital growth and development observed in patients with CBS. Further research combining the fields of morphometric measurements and pathogenesis may shed light on the aetiology of this enigmatic condition.
Footnotes
Acknowledgements
We thank Drs Yuko Akutsu (Orthopaedic Surgery, Hokkaido Ohno Memorial Hospital, Sapporo Japan) and Hikaru Hayakawa (Department of Orthopaedic Surgery, Sapporo Medical University School of Medicine, Sapporo, Japan) for their advice concerning the evaluation of the patients; Atsushi Teramoto and Makoto Emori (Department of Orthopaedic Surgery, Sapporo Medical University School of Medicine, Sapporo, Japan) for their pre- and postoperative assessment of clinical and radiographic findings and help in drafting the manuscript; and Dr Toshihiko Yamashita (Sapporo Medical University, Sapporo, Japan) for the study coordination and help in drafting manuscript.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Kousuke Iba has an endowed chair at Department of Musculoskeletal Anti-aging Medicine, Sapporo Medical University. The other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Informed consent was obtained from patients’ parents/guardians before enrolment in this study and the study was approved by the Institutional Review Board of Sapporo Medical University.
Informed consent
Informed consent was obtained from the patients and their family before enrolment in this study.