
Abstract
The aim of this study was to compare the symptomatic, functional and satisfaction outcomes of patients with different temperaments undergoing carpal tunnel surgery by a single surgeon. Dominant temperaments of 171 patients with carpal tunnel syndrome were determined using the Temperament Evaluation of Memphis, Pisa, Paris and San Diego Autoquestionnaire (TEMPS-A). Patients were divided into six temperament groups, and the impact of their respective group measured against preoperative and postoperative symptom severity and functional capacity using the Boston Carpal Tunnel Questionnaire (BCTQ] and satisfaction using the Patient Evaluation Measure (PEM). Patients in the depressive group had the largest improvement in symptoms (BCTQ score change, –2.2) as well as a significant improvement in function (BCTQ score change, –2.1), yet had the lowest postoperative satisfaction (mean PEM score 9). Determination of patient temperament before surgery for carpal tunnel syndrome (CTS) may be useful as an ancillary technique to help predict postoperative satisfaction, which may in turn help guide preoperative communication and expectation setting.
Introduction
Carpal tunnel release for carpal tunnel syndrome (CTS) is the most common surgical procedure performed in hand surgery. A variety of patient-reported questionnaires and surveys have been used to assess the severity of CTS and measure outcomes after surgery, including the Medical Outcomes Short Form 36 (SF-36); Disabilities of the Arm, Shoulder and Hand (DASH) score, Quick DASH and Patient Evaluation Measure (PEM) (Giannini et al., 2002). Many of these instruments have been validated for use in patients with CTS, although the impact of different personality types and temperaments on the outcomes of surgery, including post-surgical satisfaction, have not been studied.
Temperament has been described as a constellation of inherited structural features; attitudes and behaviours with a genetic and biological basis (Goodwin and Jamison, 1990) that do not change much during our life span (Sayın et al., 2005). The concept of temperament is a product of German nosological research from a century ago that began with the works of Kraepelin (Akiskal et al., 2005a). Five basic affective temperaments in human beings have been described: anxious (worried), depressive, cyclothymic (mood swings), irritable (nervous) and hyperthymic, a term borrowed from Schneider and corresponding to the manic-cheerful and uninhibited types as defined by Kraepelin (Akiskal et al., 2005b).
In practice, clinicians may encounter patients with certain temperaments that would remain dissatisfied with their treatment, no matter the outcome. The question remains as to whether the temperament of patients with CTS would have an impact on their level of satisfaction after carpal tunnel release surgery. We hypothesized that patients with CTS who have predominately anxious, depressive or irritable temperaments would have the lowest levels of satisfaction despite achieving good symptomatic and functional relief after carpal tunnel surgery. The aim of our study was to compare the symptomatic, functional and satisfaction outcomes of patients with different temperaments undergoing carpal tunnel surgery.
Methods
Study population
This retrospective study involved consecutive patients who had surgery for CTS from 2009 through 2011 by a single surgeon (MK) of Level 3 expertise (Tang and Giddins, 2016). The diagnosis of CTS in each patient was based on a history of paraesthesia and pain in the median nerve distribution along with abnormal Tinel’s and Phalen’s provocative tests, as well as our departmental criteria on grip and pinch strength measurements (Baker et al., 2013) and a positive electromyogram test (Preston and Shapiro, 2020). The typical indication for surgery was a lack of improvement in CTS with conservative treatment, such as a wrist splint and/or analgesics. Patients with inflammatory arthropathy, peripheral neuropathy, cervical discopathy, thoracic outlet syndrome or a history of hand or wrist fracture were excluded from the study. Patients with any established history of psychiatric illness were also excluded from the study. Informed consent was obtained from all patients before surgery, and the present study was approved by our Faculty of Medicine Clinical Research Ethics Committee.
Outcome measures
The Temperament Evaluation of Memphis, Pisa, Paris and San Diego Autoquestionnaire (TEMPS-A) was used to determine the dominant temperament of each patient in the study (Akiskal et al., 2005b). This temperament scale is a 110-item psychometric tool that was developed in 1997 and validated in Turkish (Vahip et al., 2005). Patients' TEMPS-A scores were evaluated during hospital admission for their surgery at the point of initial discharge. The patients were divided into six temperament groups according to their TEMPS-A scores: Group 1, anxious; Group 2, no dominant temperament; Group 3, depressive; Group 4, cyclothymic; Group 5, irritable; Group 6, hyperthymic. The cut-offs for each temperament were based on z-scores higher than +1 standard deviation (SD).
The preoperative and 3-month postoperative symptoms and functional capacity of the patients in this study using the Boston Carpal Tunnel Questionnaire (BCTQ) (Levine et al., 1993). The BCTQ is a patient-reported questionnaire that examines the symptom severity and overall functional status of patients with carpal tunnel syndrome. Its Symptom Severity Scale contained 11 questions (scores 1 to 5), and its Functional Status Scale has eight questions (scores 1 to 5, ranging from 1 – no difficulty to 5 – difficult).
The postoperative satisfaction level of patients in the study was assessed using the PEM scale at their 3-month postoperative visit. The PEM scale was developed by Burke in 1995 and has subsequently been validated as an outcome measure for CTS (Hobby et al., 2005a). The questionnaire is easy for patients to complete because of its visual analogue format with a total of 18 items, which are each scored using a seven-point scale (the lower the score the better), and consists of three domains: opinion on delivery of care (five questions), hand health (ten questions) and overall assessment (three questions).
Operative technique
All surgical procedures were performed by the same surgeon (MK) with regional intravenous anaesthesia (RIVA) and under tourniquet control. An open surgical technique with an extended ulnar incision was performed as previously described (Bilgin, 2011). A soft bulky bandage was applied postoperatively and the patients discharged on the same day but recalled for dressing change after 24 hours. Patients were encouraged to perform minimal hand and wrist exercises starting 7 days after surgery with full use of their hands starting between 15 and 21 days after surgery, depending upon the level of tolerance.
Statistical methods
Shapiro–Wilk testing was used to demonstrate the non-parametric distributions of the BCTQ scores including preoperative to postoperative score changes. Wilcoxon Signed Ranks Test was used to compare preoperative with postoperative BCTQ scores for each group. A p-value <0.05 was considered statistically significant.
Results
A total of 171 patients were included in the study. Of these, 30 (18%) were male and 141 (82%) females. The mean age was 49.6 years (range 20 to 75). The mean preoperative duration of symptoms was 32.4 months (range 15 to 120), and the mean follow-up was 14.1 months (range 6 to 24). The right hand was the dominant hand in 155 (90%) patients, and CTS occurred in the dominant hand in 150 (87%) of the patients. The most common comorbidities were hypothyroidism with hormone replacement in 12 (7%) patients and diabetes mellitus without peripheral neuropathy in 10 (6%) patients. The proportion of different temperaments of the patients are as shown in Table 1–3.
Preoperative and postoperative symptom severity based on Boston Carpal Tunnel Questionnaire (BCTQ) scores of 171 patients before and after carpal tunnel surgery, by dominant temperament type.
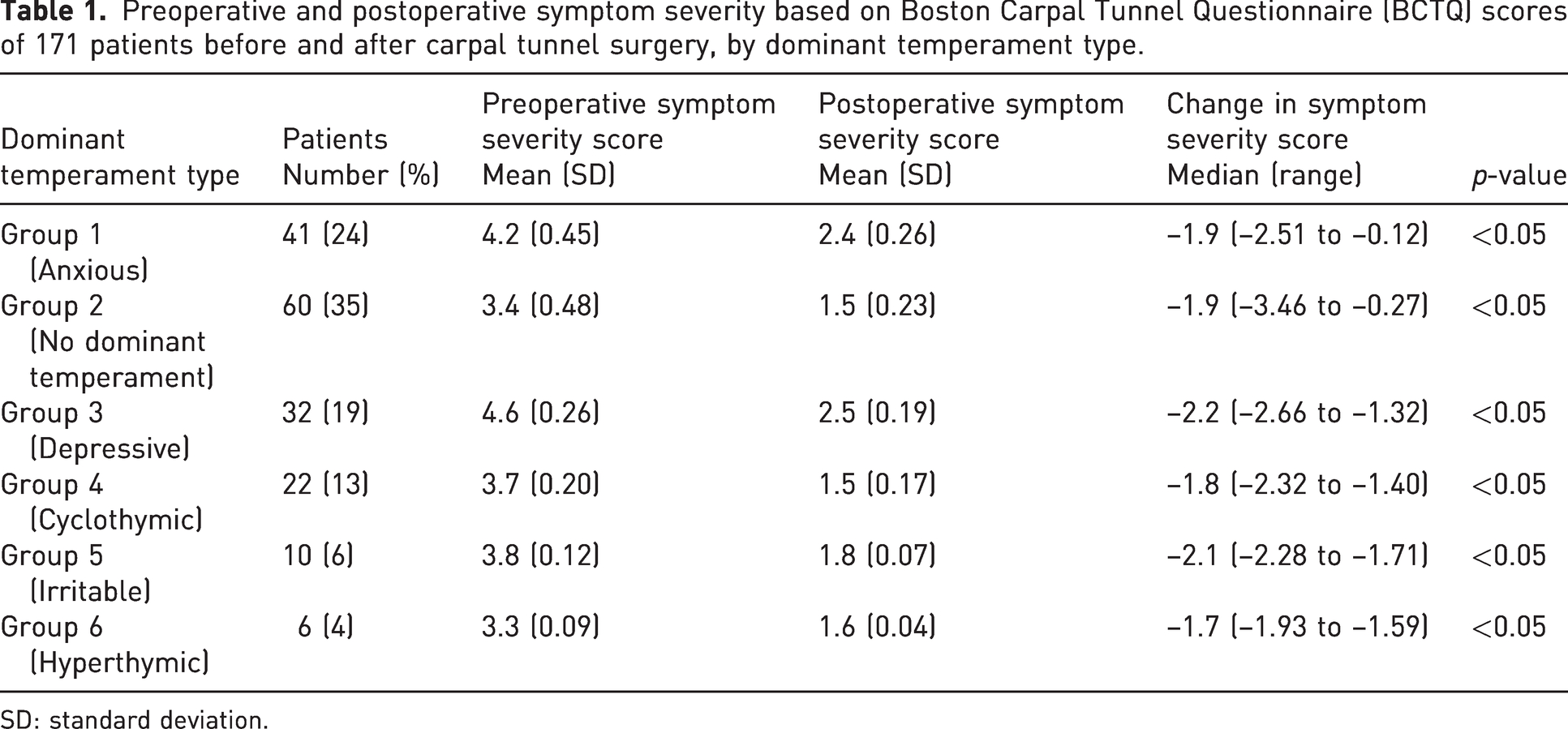
SD: standard deviation.
Preoperative and postoperative functional capacity based on Boston Carpal Tunnel Questionnaire (BCTQ) scores of 171 patients before and after carpal tunnel surgery, by dominant temperament type.
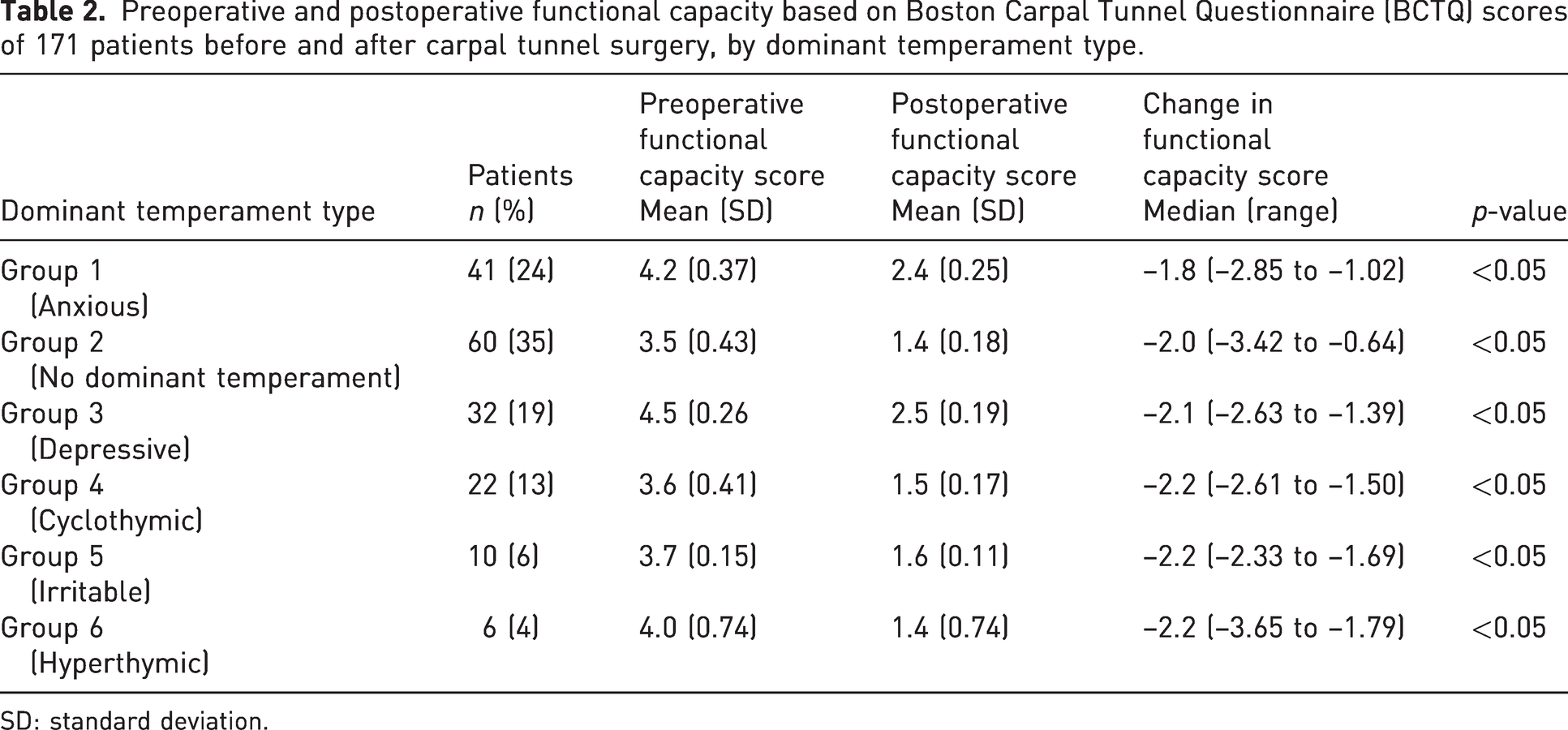
SD: standard deviation.
Postoperative Patient Evaluation Measure (PEM) scores of 171 patients after carpal tunnel surgery, by dominant temperament type.
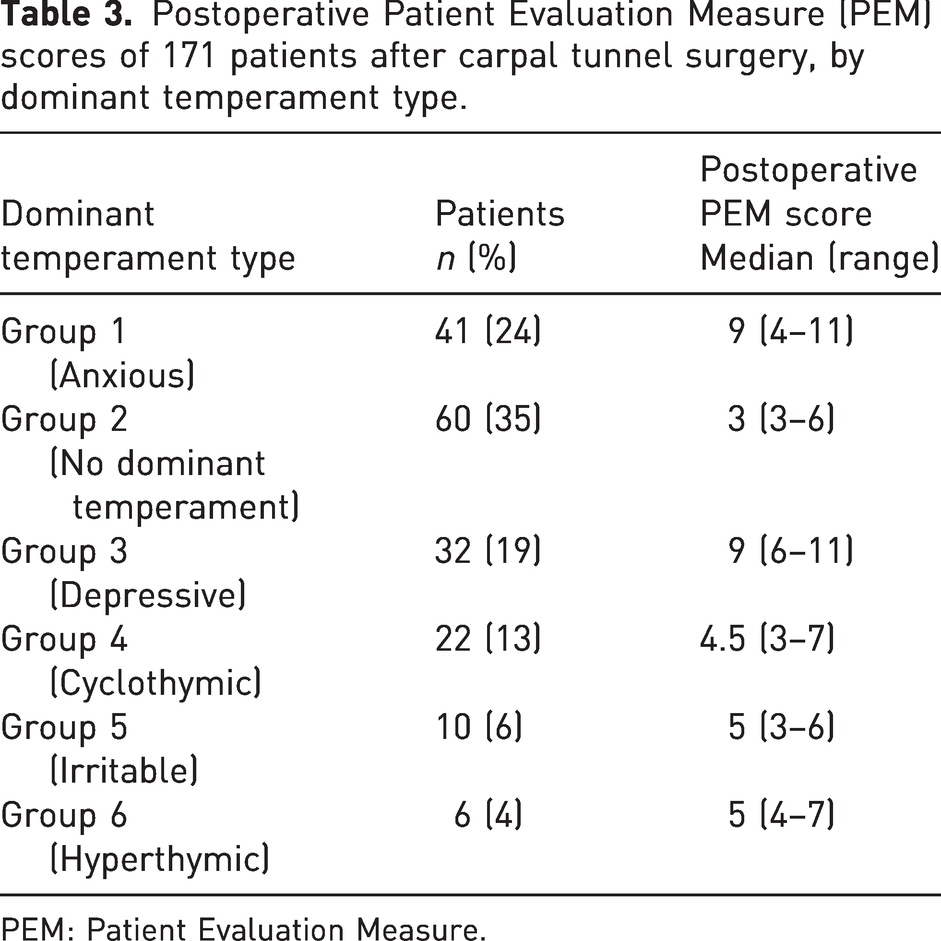
PEM: Patient Evaluation Measure.
Outcomes
The BCTQ symptom severity improved significantly from preoperative to postoperative for patients in all temperament groups (Table 1). The largest median change score was seen in the depressive group, the irritable group and the anxious group, while the smallest median change was seen in the hyperthymic group.
The BCTQ functional capacity also improved significantly from preoperative to postoperative for patients in all temperament groups (Table 2). The largest median change was seen in the depressive, irritable and hyperthymic group, and the smallest seen in the anxious group.
The poorest postoperative median PEM score of satisfaction was seen in both the anxious and depressive groups. The best median score was seen in the group with no dominant temperament (Table 3). In addition, significant differences in satisfaction were identified individually between the group with no dominant temperament and the other groups (i.e. anxious, depressive, irritable and hyperthymic all p < 0.001; cyclothymic p = 0.01).
Discussion
In this study we studied the impact of temperament on patients undergoing carpal tunnel decompression and found that BCTQ symptom severity improved significantly after surgery compared with pre-surgery for patients in all temperament groups. We also found that although patients in the depressive group had the greatest improvement in symptoms as well as a significant improvement in function, their postoperative satisfaction was lowest together with the anxious group, as compared with the other groups.
Identifying dominant temperament types in patients may help with choosing the most appropriate treatments as well as managing patient expectations and recovery. Psychological comorbidities, such as depression and pain catastrophizing, correlate with reduced function and higher levels of pain in orthopaedic patients (Giannini et al., 2002).
Our study hypothesis was that patients with CTS undergoing surgery who had anxious, irritable or depressive temperaments would have the lowest levels of postoperative satisfaction despite having good symptomatic and functional relief after the surgery. We found that although the patients in these three groups experienced significant improvements in symptoms and function, patients in the anxious group had the smallest improvement in functional capacity of any patients in the study. At the same time, patients in the anxious and depressive (but not irritable) temperament groups had poorer satisfaction scores as compared with patients in the other groups. Ironically, patients in the depressive group had the largest improvement in symptoms as well as a significant improvement in function, yet reported the lowest postoperative satisfaction of any patients in the study. These findings support part of our hypothesis and suggest that despite successful CTS surgery, patients who have a depressive or anxious temperament may ultimately be less satisfied after surgery.
Patient satisfaction is an important criterion in determining success following carpal tunnel surgery, however, the factors that affect patient satisfaction are not fully understood. An effective assessment of patient satisfaction should go beyond the variables traditionally covered in the surgical literature and explore the patient's psychosocial aspects and decision-making. From our study, it may appear that patient temperament plays a role in predicting outcomes after CTS surgery, but it is important to note that like many other procedures, outcomes after carpal tunnel surgery can also be affected by age, gender, race, socioeconomic status and education level (Hobby et al., 2005b) and temperament is just one of the multifactorial considerations.
All patient groups in the study demonstrated significant preoperative to postoperative improvements in symptom severity and functional capacity scores. At the same time, the best absolute scores for both symptom severity and functional capacity at the 3-month postoperative visit occurred in the group with no dominant temperament type. One possible explanation for this is that these patients also started preoperatively with some of the best absolute BCTQ scores. It is known that psychological distress affects CTS symptoms, diagnosis and treatment programme. The more symptomatic patients are, the higher they score on anxiety and depression scales, even before they are diagnosed with CTS. Therefore, it is unsurprising that patients with less symptomatic and better functional scores have a non-dominant temperament (McCallum et al., 2019). In addition, patients with no dominant temperament type had higher absolute postoperative scores for satisfaction than all of the other patients in the study. We are unable to compare our findings with other reports in the literature, however, we hypothesize that patients without a dominant temperament type may be more likely to perceive better postoperative symptoms, function and satisfaction than patients who do have a dominant temperament type, particularly anxious or depressive. Further large-scale prospective studies are required to validate our hypothesis.
Although others have reported positive outcomes of open carpal tunnel surgery using the BCTQ (Ettema et al., 2006; Ollivere et al., 2009; Pfeffer et al., 1988), the extent of improvement in symptom severity and functional capacity have been less than what we observed from our study. We do not have a clear reason for this difference but postulated that the process of evaluating the patient’s temperament itself may have contributed to better outcomes, perhaps by creating more biopsychosocial awareness. The biopsychosocial model was first conceptualized by George Engel in 1977, and it theorizes that the understanding of a patient’s medical condition involves considering not only biological factors, but also psychological and social factors (Engel, 1977). In this model, both the mind and the body impact each other. Temperament is a psychological factor that fits with thoughts, emotions and behaviours in playing an intermediary role between the mind and body. This study further provides findings that support the use of a biopsychosocial approach in providing clinical care to patients. Additional study of the correlations between affective temperaments and patient outcomes is warranted.
This study has several limitations. First, because the study was focused on only patients with CTS, the findings would not necessarily be generalizable to other orthopaedic or even hand disorders. Second, the results were not analysed with regards to severity of CTS, which may have an impact of the symptomatic, functional and satisfaction score. Third, the actual numerical differences between groups and changes in BCTQ and PEM results were small even though there were statistically significant changes.
In conclusion, our findings support the notion that temperament may play a part in outcomes after CTS. Scoring an individual patient with an instrument like the TEMPS-A before surgery could contribute to predicting the level of postoperative satisfaction, which may in turn help guide preoperative communication and expectation-setting.
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all patients before surgery. Informed consent was sought for the present study.
Ethical approval
Ethical approval for this study was obtained from Ankara University Faculty of Medicine Clinical Research Ethics Committee.