
Abstract
Fractures of the phalanges encompass a wide range of injury patterns with variable articular and soft tissue involvement. The goals of treatment whether conservative or surgical are the restoration of function while limiting the risk of complications. An armamentarium of fixation options allows the surgeon to appropriately treat these fractures with the intention of initiating early postoperative mobilization. Previous publications report variable rates of complications following internal fixation of phalangeal fractures which represents an unsolved problem. It is incumbent on the surgeon to utilize meticulous surgical technique, achieve anatomic reduction with stable fixation and initiate early postoperative mobilization where indicated. In the following text, we review the management of most types of phalangeal fractures, except fracture-dislocations of the proximal interphalangeal joint. These injuries comprise a wide spectrum of presentation; thus, an understanding of anatomical and mechanical principles is integral to achieving a successful outcome.
Introduction
Phalangeal fractures may occur at any age; however, the majority occur in men in the fourth decade of life (Moura et al., 2022). Risk factors include behavioural decisions, occupational hazards and participation in sport. Previous publications disagree regarding the specific details of phalangeal fractures. The little finger has been described as the most vulnerable to fracture due to its unprotected outer location (Moura et al., 2022). Conversely, others say the length of the middle finger predispose it to a higher proportion of phalangeal fractures (Brown, 1967). Kremer et al. (2022) described finger length as being a predictor for phalanx fracture, noting that the ring finger was most frequently fractured in their series. The most common phalanx to be fractured also varied across the literature. Moura et al. (2022) and Kremer et al. (2022) reported the distal phalanx had the highest incidence of fracture across the index, middle and ring fingers, and the proximal phalanx had the highest incidence of fracture in the little finger. Van Oosterom et al. (2001) reported the proximal phalanx had the highest incidence of fracture for the index, middle and little fingers.
Fracture profile is highly dependent on the mechanism of injury, with crush and blunt trauma being the most common. Crush trauma often results in tuft fractures and blunt trauma can create a bending moment, which often results in shaft fractures. As force is transmitted proximally, the narrow diameter of the phalangeal shaft is unable to withstand additional load and yields. Moura et al. (2022) reported a transverse fracture of the shaft of the phalanx to be the most common fracture pattern and location. Distal phalanx tuft fractures and middle phalanx base fractures were the most common locations and fracture patterns according to Kremer et al. (2022).
Although the avoidance of surgical management is often intended to reduce the risk of complications, the functional detriment that results from immobility is demonstrable (Baaqeel et al., 2017; Neumeister et al., 2021). Importantly, conservative treatment is effective when coupled with immediate mobilization (Byrne et al., 2020; Rajesh et al., 2007). Oedema from the injury coupled with immobility results in physiologic changes which inhibit motion. Fibrosis, adhesions and contractures can be mitigated by immediate mobilization.
There is no standardized protocol for the surgical treatment of phalangeal fractures. This is due in part to the wide variation in case presentation including fracture pattern, concomitant fractures and soft tissue injury. The goals of treatment, whether conservative or surgical, are the restoration of function while limiting the risk of complications. The decision to manage a fracture surgically involves several variables, including but not limited to the radiographic presentation, the relevant anatomy and the patient’s functional status, occupation and ability to tolerate mobilization (Figure 1).
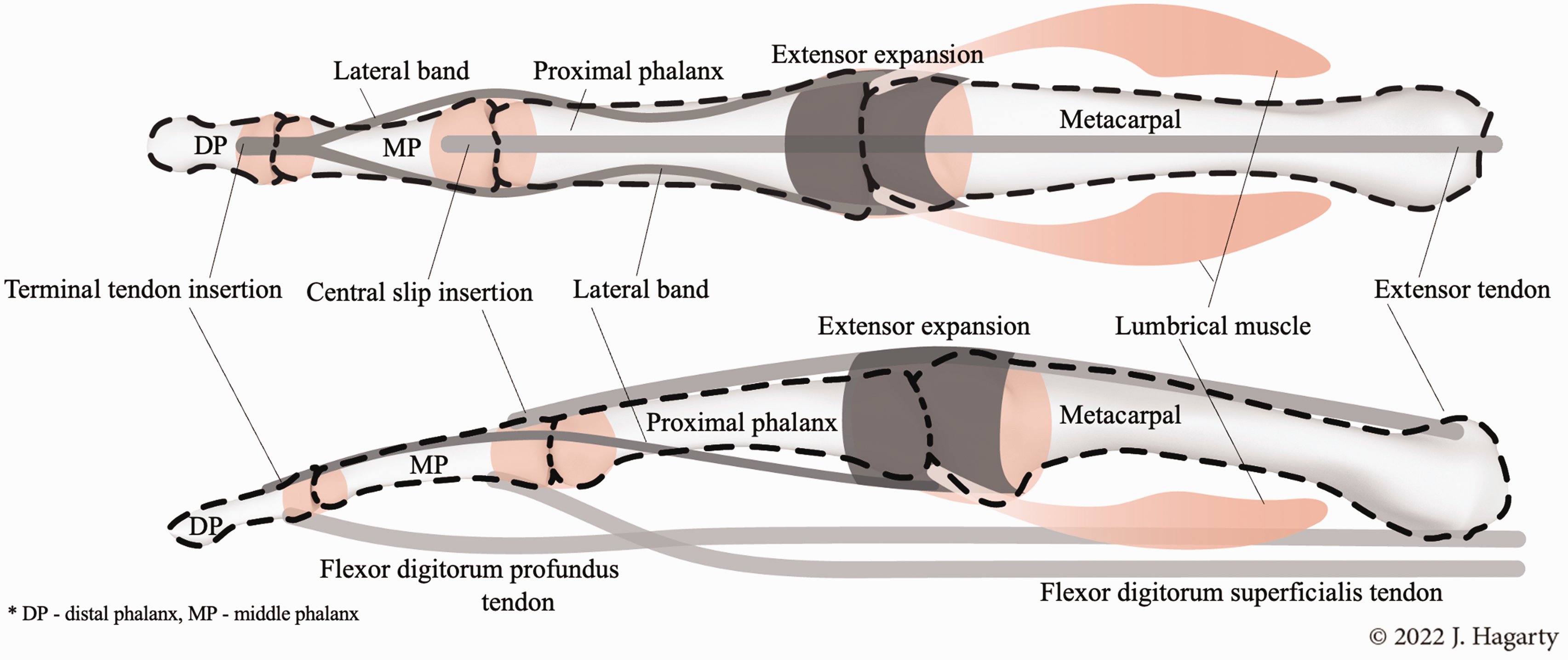
Graphic depiction of anatomical structures, including flexor or extensor tendons, surrounding the phalanges.
Fixation should provide the requisite stability to withstand the forces generated during postoperative mobilization. More stable constructs often require more extensive dissection for implantation. Page and Stern (1998) reported 64% of phalangeal fractures developed stiffness after surgical plate and screw fixation, with 20% requiring additional surgical procedures. Further, Ip et al. (1996) reported that 10% of digital fractures resulted in stiffness and 91% of those stiffness cases required surgical intervention. Thus, previous publications have demonstrated the high risk of stiffness and subsequent intervention after surgical management of phalangeal fractures. Attempts to attain complete visualization of fracture fragments through extensive dissection can be detrimental. Soft tissue and vascular disruption can result in fibrosis and scarring which inhibit motion.
Proximal phalangeal fractures
In this section, we discuss the general principles of management of proximal phalanx fractures with more detail on fractures of the shaft, metaphysis and base as well as condylar fractures of the distal end of the proximal phalanx.
Shaft fractures of the proximal phalanx are commonly oblique or spiral in orientation. The force vector of the intrinsic muscles contributes to malalignment of the phalanx. Unstable fractures are frequently dorsally angulated due to the line of action of the intrinsic muscles passing dorsal to the axis of rotation of the metacarpophalangeal (MCP) joint (Shewring et al., 2018). Surgical management is often needed to restore normal alignment. Further, it is likely that unstable cases treated conservatively will result in suboptimal kinematics that are quite difficult to reverse. In stable cases with acceptable alignment, splinting in MCP flexion and interphalangeal extension is preferred (Day and Stern, 2011). This position stabilizes the MCP joint by tensioning the collateral ligaments and reducing the deforming forces of the lumbrical muscles on the proximal fragment. Shewring et al. (2018) used a single K-wire for fixation of proximal phalanx fractures at the proximal meta-diaphyseal junction. In a series of 101 patients, there were two pin site infections, and all patients regained full range of motion at the MCP joint. Mobilization was initiated at the interphalangeal joints on day 1 postoperatively and the wire was removed at day 24. Recent biomechanical investigation demonstrated that a single transarticular wire had similar stability compared to crossed wires in an unstable shaft fracture model of the proximal phalanx (Nikci et al., 2023).
Generally accepted radiographic parameters that may indicate surgical treatment for non-articular fractures are more than 10° of angulation, more than 2 mm of shortening and rotational deformity. We usually have a lower threshold for angulation in the coronal plane due to cosmesis and risk of scissoring. In cases where surgical fixation is indicated, there is an increasing body of evidence for stable internal fixation. The most common methods of internal fixation for phalangeal fractures are Kirschner wires (K-wires), plate and screw constructs, and intramedullary screws. K-wire fixation is minimally invasive, financially attractive and widely available. Thus, K-wires are commonly utilized for internal fixation (Figure 2), but recent publications demonstrate mixed evidence. Reformat et al. (2018) reported that K-wire fixation had a significantly longer period of immobilization compared to plate fixation, but total active motion and time to return to work were not significantly different between these fixation methods. In contrast, Wang et al. (2020) reported superior clinical outcomes and lower rates of complication for plate fixation compared to K-wire fixation. Their meta-analysis, including more than 2000 patients, reported higher rates of excellent and good outcomes with lower pain scores and lower incidence of complications in the plate fixation group compared to the K-wire fixation group.
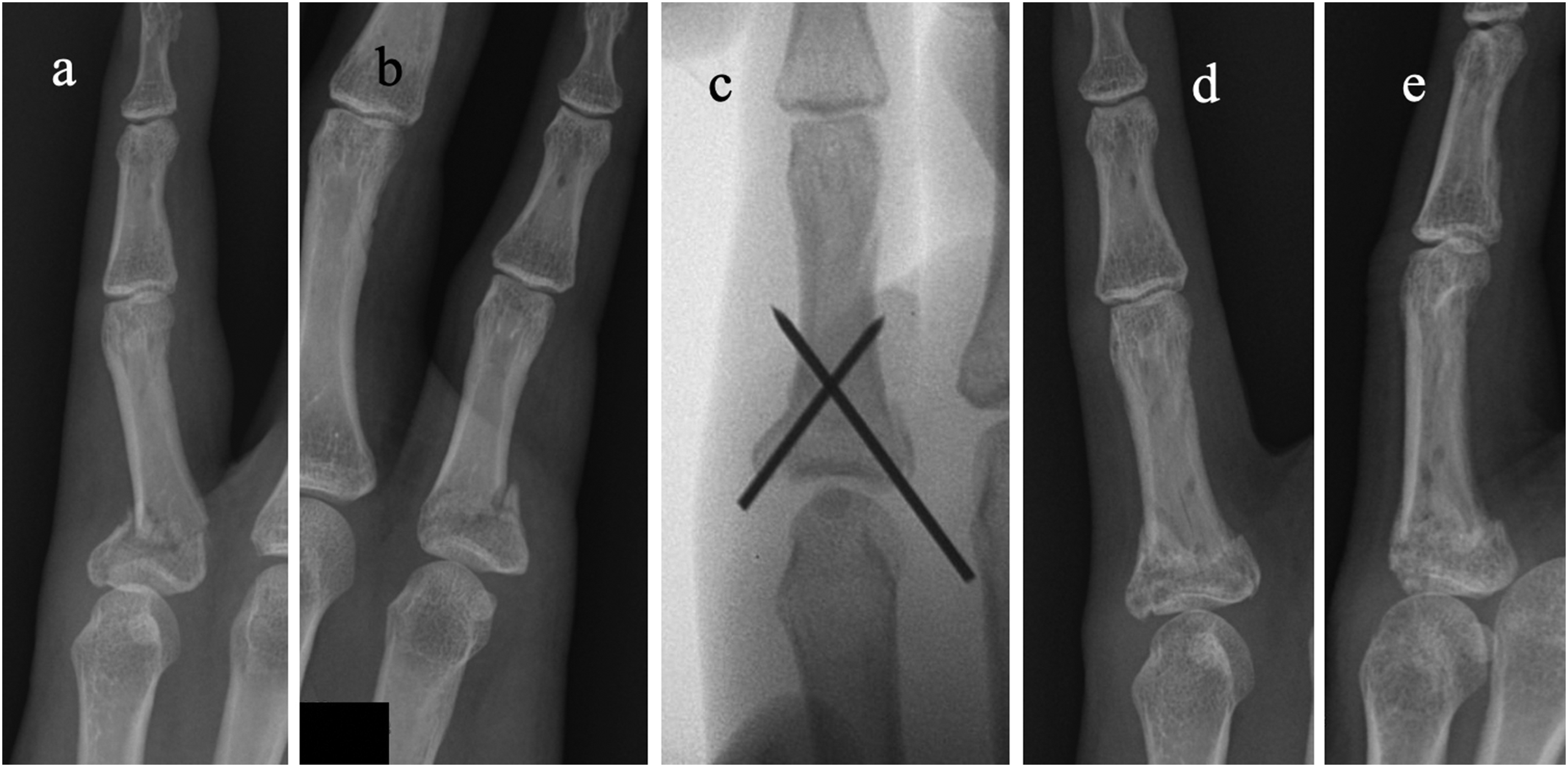
(a, b) Radiographs demonstrating an unstable fracture of the base of the proximal phalanx with angular deformity and rotational malalignment. (c) Intraoperative fluoroscopy of fracture fixation using crossed Kirschner wires. (d, e) Radiographs 10 weeks postoperatively after wire removal 4 weeks after surgery.
Closed reduction with percutaneous K-wire fixation becomes more difficult as the time from injury increases and callus formation ensues. In some cases, a percutaneous K-wire can be used as an instrument to take down early callus formation. This technique can be advantageous because the remaining non-disrupted callus often imparts some stability that maintains fracture alignment while adjustments to angulation and rotation are made. K-wires measuring 0.9 or 1.1 mm are suitable for fractures involving the base and shaft of the phalanx, and smaller diameter K-wires are reserved for comminuted periarticular fractures or single condylar fractures. Multiple K-wire passes through the same holes should be avoided, because the static friction between the wire and bone decreases with multiple passes. Importantly, if a deformity remains after reduction, the wire can be withdrawn from the far cortex, the alignment adjusted and the wire advanced into a new point in the far cortex. This method is useful in cases where removal of the entire pinning construct can create instability that is more technically difficult to correct than making minor adjustments.
If closed reduction with percutaneous K-wire fixation is not possible, open reduction internal fixation (ORIF) should be utilized. Depending on the location of the fracture, the surgeon must be cognizant of the neighbouring anatomical structures, including the relationship of the flexor and extensor mechanisms to the fracture. A limited open lateral approach through or just anterior to the lateral bands often provides adequate cortical access to assist in reduction with minimal disruption of the extensor mechanism.
Long oblique fractures may be fixed with interfragmentary screws, but for short oblique or transverse fractures, plate and screw fixation provides superior mechanical stability (Rausch et al., 2020). Stable fixation allows confident initiation of immediate postoperative mobilization, but the surgeon must evaluate the advantage of improved stability against the additional soft tissue dissection that may be required to properly implant plates. The insults from surgical exposure and implant prominence may lead to functional detriment. Despite satisfactory outcomes with functional motion, stiffness, fixed flexion contracture and extensor lag have been reported following plate and screw fixation (Katayama et al., 2020; Brei-Thoma et al., 2015; Kurzen et al., 2006). El-Saeed et al. (2019) reported that plate and screw fixation provided greater motion and fewer complications than K-wire fixation for unstable fractures of the proximal and middle phalanges. Notably, cases utilizing plate and screw fixation had a mean of over 30 minutes more operative time compared to K-wire fixation.
Intramedullary screw fixation
There is evidentiary momentum for intramedullary (IM) screw fixation due to its more minimally invasive approach and the favourable outcomes that have been reported across numerous techniques (del Pinal et al., 2015; Giesen et al., 2016; Gray et al., 2022). Single IM screw fixation may be indicated in simple fracture patterns; however, for comminuted or length unstable fractures, dual IM screw fixation is more appropriate (Figure 3). The addition of a second IM screw provides increased stability reducing the risk of failure during early mobilization and provides additional rotational control, which is especially important in phalangeal fractures (Henry, 2008). Various techniques for screw placement have been described including Y-type patterns (del Pinal et al., 2015) and converging patterns (Gray et al., 2022).
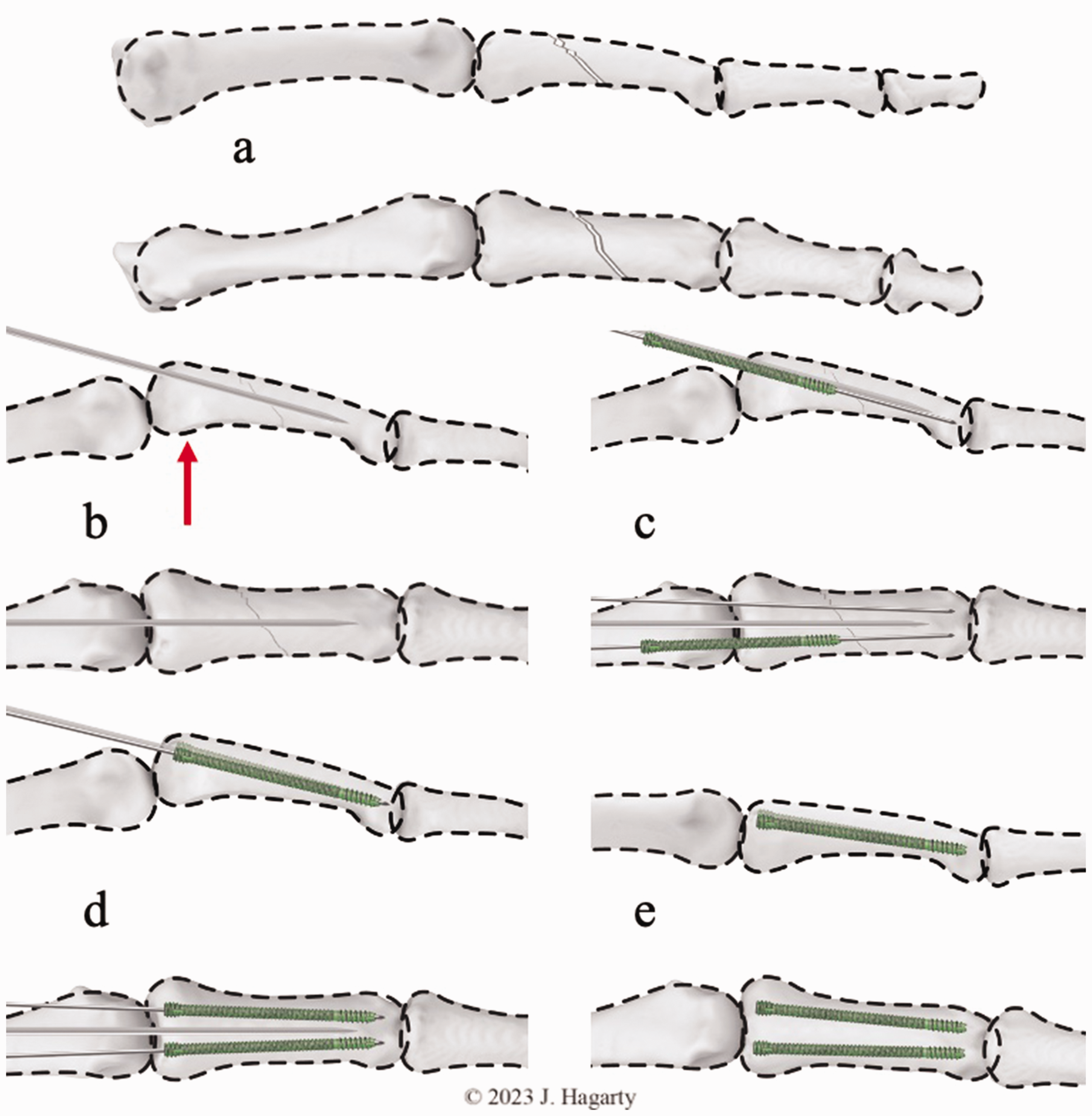
(a) Graphic sequence of the technique for dual screw fixation for fractures of the proximal phalanx. (b) A dorsally directed force (arrow) is applied to the base of the proximal phalanx to translate the bone in relation to the metacarpal head. Provisional fixation is provided by a K-wire inserted centrally in the coronal plane and in the dorsal third in the sagittal plane. (c) Guidewires are inserted on each side of the central wire to facilitate maintenance of reduction during screw insertion. If using cannulated screws, (d) the guidewires are retained during screw insertion, (e) then removed after dual screw insertion.
Our preferred technique is to use dual IM screws for shaft and non-articular or simple base fractures of the proximal phalanx (Figure 4). A block is placed under the MCP joints to maintain flexion throughout the procedure facilitating screw insertion. Manual force is applied to dorsally translate the base of the proximal phalanx relative to the metacarpal head, allowing placement of a 1.6 mm K-wire centrally in the coronal plane and dorsally in the sagittal plane.

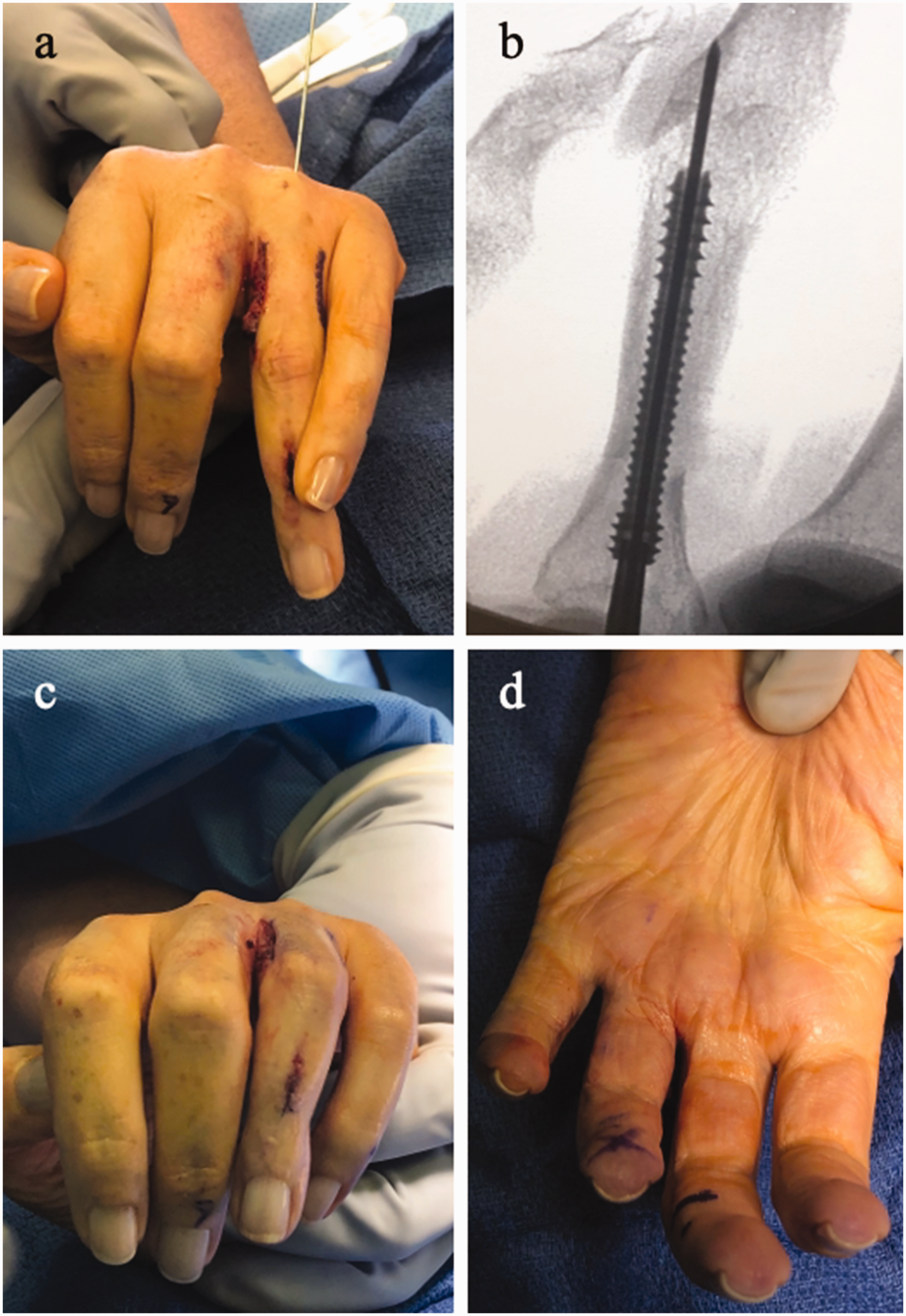
(a) Radiographs demonstrating a comminuted fracture of the proximal phalanx. (b, c) Fluoroscopy demonstrating guidewire insertion on both sides of a centrally placed larger K-wire, which is used for provisional fixation. (d, e) Dual 2.0 mm headless compressions screws were used for fixation.
After reduction, the wire is advanced anterograde across the fracture site. The larger diameter wire provides stability and maintains provisional reduction during subsequent guidewire placement and screw insertion. Cannulated screw guidewires are inserted on either side of the central wire, and if possible, driven into subchondral bone in the head of the phalanx. Appropriate screw diameter is dependent on intramedullary fit. The anteroposterior diameter of the phalangeal neck is usually the constraining dimension. Often a smaller diameter will allow a longer screw length, capable of extending into the phalangeal head. We prefer to drill manually to protect the surrounding tissues. When inserting the first screw, the central wire and the other peripheral guidewire maintain reduction. The peripheral guidewires are removed after screw insertion and the central wire may be removed if it interferes with insertion of the second screw. Throughout the procedure, care is taken to ensure wire or screw insertion does not damage the head of the metacarpal. Our results have been consistently satisfactory which we attribute to the reproducible nature of this technique.
Condylar fractures
Condylar fractures of the proximal phalanx are classified as follows: type I, which are stable and non-displaced; type II, which are unstable unicondylar; and type III, which are bicondylar (London, 1971). Weiss and Hastings (1993) classified unicondylar fractures as follows: class I, which have an oblique palmar split; class II, which have a long sagittal split; class III, which have a dorsal coronal split; and class IV, which have a palmar coronal split. Determination of treatment and fixation options is dependent on the amount of displacement, which is usually indicative of stability. If conservative treatment is chosen, continued monitoring is important as secondary displacement is likely even in stable patterns. These fractures can be managed with K-wire or screw fixation, typically pinning the fractured condyle to the intact condyle or to the intact shaft. A minimum of two wires should be placed whenever possible to confer stability. Dual wires placed in a parallel or crossing fashion have demonstrated satisfactory outcomes with few complications (Sadek, 2020). Oblique condylar splits with proximal propagation are amenable to fixation with multiple wires placed slightly divergent to each other. Short transverse screws can be placed as well with the advantage of stab incision percutaneous or limited open approaches that facilitate early mobilization. Shewring et al. (2015) demonstrated that single lag screw fixation through a mid-lateral approach for unicondylar fractures allowed early mobilization and yielded satisfactory outcomes. Bicondylar fractures were treated with one or more lag screws across the fracture line extending proximally, and a lag screw distally connecting both fragments. More complex fractures may require a plate positioned on the lateral aspect of the bone.
Fractures of the base of the proximal phalanx
Articular fractures of the base of the proximal phalanx include minimally displaced avulsions of the collateral ligaments and comminuted multi-fragment fractures. Due to the wide range of fracture presentation, treatment is dependent on the fracture characteristics and the extent of soft tissue disruption. Small fragments that are closely approximated may achieve a satisfactory outcome with conservative treatment. Larger single fragments may be amenable to K-wire or screw fixation, but multi-fragment fractures require more stable fixation. External fixation is an option for cases where internal fixation may be contraindicated, such as those with severe comminution or extensive soft tissue disruption.
Middle phalangeal fractures
Fractures of the base or shaft of the middle phalanx are often amenable to K-wire fixation. Single IM screw fixation may also be used for certain fracture patterns. Screw insertion can be anterograde through a flexed proximal interphalangeal (PIP) joint or retrograde through a flexed distal interphalangeal (DIP) joint. Comminuted articular fracture of the middle phalanx base with concomitant PIP joint instability is a particularly complex injury whose detailed management is beyond the scope of this review (See: Proximal interphalangeal joint dislocation and fracture dislocation, page number in this issue).
Midshaft fractures of the middle phalanx typically present with a dorsal angulation deformity and can be associated with a mallet deformity of the DIP joint if the angular deformity is not corrected. In these cases, if K-wire fixation is used, our preferred technique is to introduce the wires retrograde, reducing the fracture (Figure 5). A single wire maintains correction of the angular deformity and an oblique wire corrects the rotational deformity. As an alternative, an appropriately sized IM screw will typically reduce angulation and correct the extensor lag at the DIP joint.
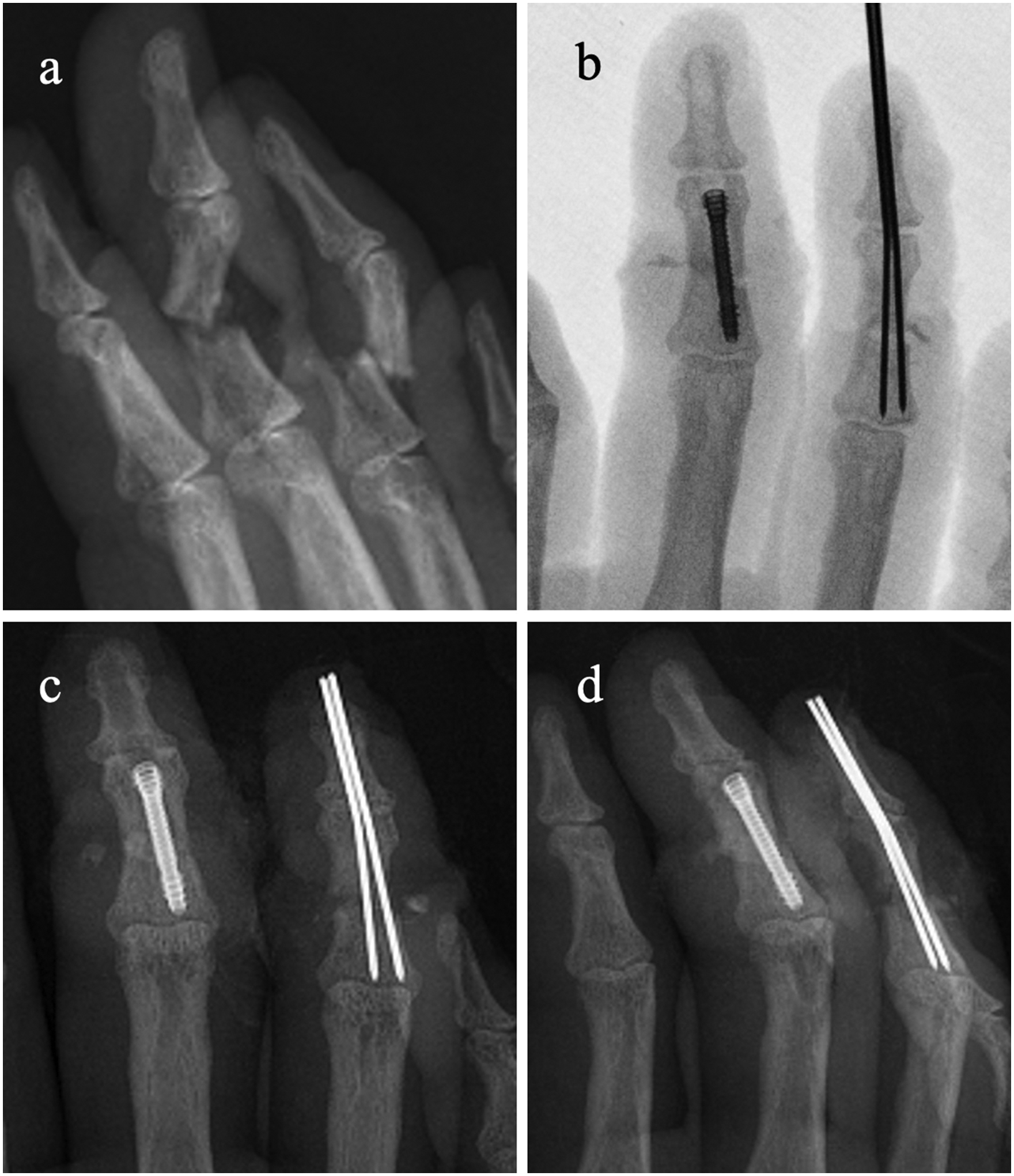
(a) Radiographs demonstrating comminuted and displaced fractures of the middle phalanges of the middle and ring fingers. (b) Intraoperative fluoroscopy and (c, d) postoperative radiographs demonstrating fixation of the middle finger with a retrograde screw, and the ring finger with K-wires that were trimmed to the level of the skin.
Neck fractures of the middle phalanx can be reduced and stabilized with K-wires or IM screws. Head fractures of the middle phalanx are usually amenable to K-wire fixation, as the small size of the head fragment may preclude screw fixation. Transverse K-wire fixation of the condyles with longitudinal retrograde pinning through the distal phalanx across the DIP joint is a useful method for fixation for condylar fractures and very distal neck fractures.
Distal phalangeal fractures
Fractures of the base of the distal phalanx include condylar splits, palmar base fractures, which may include avulsion of the flexor digitorum profundus, and dorsally displaced fractures, which may present with palmar instability of the phalanx shaft. Fracture-dislocations associated with a large dorsal fragment are amenable to dorsal block K-wire fixation coupled with longitudinal transarticular K-wire fixation of the distal phalanx. Conservative treatment is also a consideration as satisfactory outcomes have been reported for subluxed and congruent patterns of mallet fractures (Trickett et al., 2021). Our preferred technique for these fractures is to place the DIP joint in slight hyperextension while obtaining purchase into the palmar aspect of the neck of the middle phalanx with a retrograde K-wire. This is a more reliable method compared to longitudinal pinning along the shaft of the middle phalanx because the shaft can present with a gentle curvature, which places the DIP joint in slight flexion if a K-wire is centred in the canals of the distal and middle phalanx.
Avulsion fractures of the palmar aspect of the base of the distal phalanx typically require open reinsertion of the flexor tendon rather than K-wire fixation. This can be accomplished using suture anchors or small plate and screw constructs including modification of the most proximal plate hole into a hook to insert into the fracture fragment. Our preferred method of reinsertion uses a non-absorbable suture to capture the fragment, which is then passed antegrade through the shaft of the phalanx using straight Keith needles that exit the tuft. The skin bridge between the needles is incised down to the phalanx to minimize soft tissue impingement by the suture when it is tied down to the tuft cortex.
Shaft fractures of the distal phalanx are typically amenable to 1.1 mm K-wire fixation, except in the thumb where 1.6 mm K wires are the most commonly used due to the larger size of the medullary canal. Retrograde cannulated screw fixation can also be used for shaft fractures of the distal phalanx.
Shaft and tuft fractures of the distal phalanx commonly occur with fingertip crush injuries. The surgeon must be aware of overlying nailbed lacerations that can be associated with these fractures. Our preferred treatment method is to remove the nail plate, stabilize the fracture, then repair the nail bed, usually with an absorbable suture such as Chromic Gut (Medtronic, Minneapolis, MN, USA) or Vicryl Rapide (Ethicon, Inc, Somerville, NJ, USA). This treatment method typically results in anatomical fracture alignment with no persistent nail deformity. When there is extensive tuft comminution, we prefer to use a single 1.1 mm K-wire to capture the largest fragment, which is then fixed to the shaft. This wire is advanced retrograde into the base of the distal phalanx with care taken to obtain purchase at the base of the phalanx without entering the DIP joint, if possible.
The immobilization time for K-wire fixation of the distal phalanx is usually 4 weeks, at which point the wires are removed. Immediate motion is initiated at the more proximal unaffected joints using short arcs, if needed, to allow for tendon gliding. With more stable methods of fixation, such as plates and IM screws, mobilization can be initiated much earlier even when resting splints are used. Motion is usually limited after K-wire fixation due to soft tissue irritation from the K-wires. We routinely refer these patients to hand therapy for short arc tendon gliding exercises that mitigate the risk of stiffness. Our preferred method is to cut the K-wires below the level of skin. Once the K-wires are removed, therapy advances to a more aggressive range of motion protocol.
Malunion of the phalanges
The common malunion deformity of the base of the proximal phalanx is dorsal angulation due to the net forces of the soft tissue structures which attach to the bony fragments. The lumbricals flex the proximal fragment and the central slip extends the distal fragment, which produces a shortened, extended phalanx. This is a mechanical disadvantage for the extensor mechanism, which results in extensor lag at the PIP joint that is linear with the amount of shortening. A fixed flexion contracture can develop, which must be addressed to regain satisfactory function. Surgical treatment may be indicated to restore a native length tension relationship to the extensor mechanism if therapy fails to restore motion. A common option is a palmar-based closing wedge osteotomy fixed with a lateral plate which allows immediate motion. A dorsal opening wedge osteotomy may be performed in the presence of more severe deformity, with a readily accessible source of graft being the distal radius which is included in the surgical field. However, dorsal split of the extensor mechanism increases the risk of postoperative stiffness. For coronal plane malunions, opening wedge osteotomies with or without bone graft have produced satisfactory outcomes. In aggregate, reported results demonstrate efficacy for surgical intervention for phalangeal malunions (Gajendran et al., 2015).
Other angular deformities of the proximal and middle phalanges can be corrected with options such as closing wedge osteotomy, opening wedge osteotomy with or without intercalary grafting, and IM screw fixation, which will typically obtain acceptable angular correction (Figure 6). Although some translational deformity may result from screw fixation, the shortening is usually minimal, and placement of the fixation requires less invasive dissection.
(a) Intraoperative image of malunion of the middle phalanx with rotational deformity. (b) Treatment consisted of a transverse osteotomy of the proximal phalanx and fixation with a single intramedullary screw, (c, d) which restored anatomic alignment.
Rotational malunion can be corrected with a transverse osteotomy at the fracture site. The surgeon can then use their preferred method to obtain fixation and these corrections usually heal reliably. If a multiplanar correction is needed, an osteotomy can be planned to concurrently correct an angular and rotational deformity. There is commercially available planning software to assist the creation of the multi-planar osteotomies.
Nonunion of the phalanges
Although nonunion of phalangeal fractures is relatively rare, prolonged time to union has been associated with fracture location. Mid-shaft phalangeal fractures can require longer times to union due in part to the watershed perfusion at this region of the phalanx. Radiographic nonunion does not always portend clinical detriment, but when associated with adverse symptoms such as pain, repair is indicated. Surgical options include revision ORIF with bone graft, arthrodesis and amputation.
In cases of symptomatic nonunion that are managed surgically, meticulous technique is required to prepare the ends of the fracture. Fenestration drilling encourages endosteal circulation at the fracture site when utilizing adjuvant bone graft to restore the anatomy. Methods of fixation for nonunion are those that are utilized in primary fracture treatment. Non-surgical treatment has been described for the treatment of symptomatic nonunion, particularly of the distal phalanx. Abboudi et al. (2015) reported union of the distal phalanx after 2–4 months of treatment using a pulsed ultrasound bone stimulator.
Discussion
Phalangeal fractures encompass a wide range of injury patterns, including variable articular and soft tissue involvement. Basic anatomical and mechanical principles are integral components of the treatment decision. An armamentarium of fixation options allows the surgeon to appropriately treat these fractures with the intention of initiating early postoperative mobilization.
There are myriad factors that contribute to the wide variation of reported outcomes including fracture pattern, concomitant soft tissue injury and fixation techniques. It is important to remember that despite anatomic reduction and stable internal fixation, nonunion can still occur. Intrinsic patient factors, including the osteoprogenitor sequence and the immune mediated healing cascade, play a vital role in achieving bony union. Although faults within these physiologic mechanisms may predispose to nonunion despite effective surgical management, it is incumbent on the surgeon to utilize meticulous surgical technique, achieve anatomic reduction with stable fixation, and initiate early postoperative mobilization where indicated.
Footnotes
Acknowledgements
The authors appreciate the support and expertise of Abby Alaine Heifner.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This work received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.