
Abstract
Patients have attended our clinics with various hand pathologies after contracting COVID-19 or receiving vaccination. We postulate the virus stimulates a systemic inflammatory response that triggers these pathologies and conducted a search of the literature for associated conditions. Twenty publications were included for this review. Three studies identified skeletal muscle inflammation, and several identified reactive arthritis post-infection. Rheumatoid arthritis post-infection was also recognized, along with crystalline arthropathy. Carpal tunnel syndrome was seen in two cases. There is a current paucity in published scientific material regarding COVID-19 sequalae in the hand. This review aims to stimulate discussion in how a virus can induce pathological processes causing common hand pathologies.
Introduction
The SARS-CoV-2 infection commonly presents with generalized malaise, dyspnoea after minor exertions and more severely, acute respiratory distress syndrome (ARDS) and pulmonary fibrosis. We propose that the same inflammatory response and eventual fibrosis can occur in the hands and wrists, an explanation to the increase in patients presenting with benign hand pathologies who have either suffered with COVID-19 or post-COVID-19 vaccination. The aim of this literature review is to explore whether there is a causal link between SARS-CoV-2 infection or vaccination with benign hand pathology.
Methods
This review was performed using the preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines where a search of the literature was conducted through Ovid, MEDLINE, EMBASE Central, Google scholar and Trip databases between 2017 and 2022. This timeframe was used to identify studies with chronic sequelae from other Coronavirus family infections. The search string included ‘COVID-19’, ‘SARS-CoV-2’, ‘Coronavirus’, ‘Rheumatoid arthritis’, ‘inflammatory arthritis’, ‘reactive arthritis’, ‘trigger finger’, ‘trigger thumb’, ‘Dupuytrens contracture’, ‘tenosynovitis’, ‘Intersection syndrome’, ‘Carpal tunnel syndrome’, ‘Ulnar tunnel syndrome’, ‘Cubital tunnel syndrome’.
Inclusion criteria consisted of studies reporting hand pathologies in patients with active or previously confirmed COVID-19 infection. Only full text English language articles were included for analysis. Articles published in non‐peer reviewed publications were excluded.
All studies were analysed by a single observer. Other citations were identified through manual searches and cross-referencing citations of the included articles.
Results
We identified 622 articles, with 39 meeting the initial inclusion criteria. After further analysis, 16 articles were considered relevant to this review, with a further four articles found manually and a total of 20 studies were finally included (Figure 1). Thirteen of these studies were case reports, four were case series/observational studies, two were systematic reviews of the case and one was a review article (Table 1). All articles analysed in this review were Level 4 and 5 evidence only.
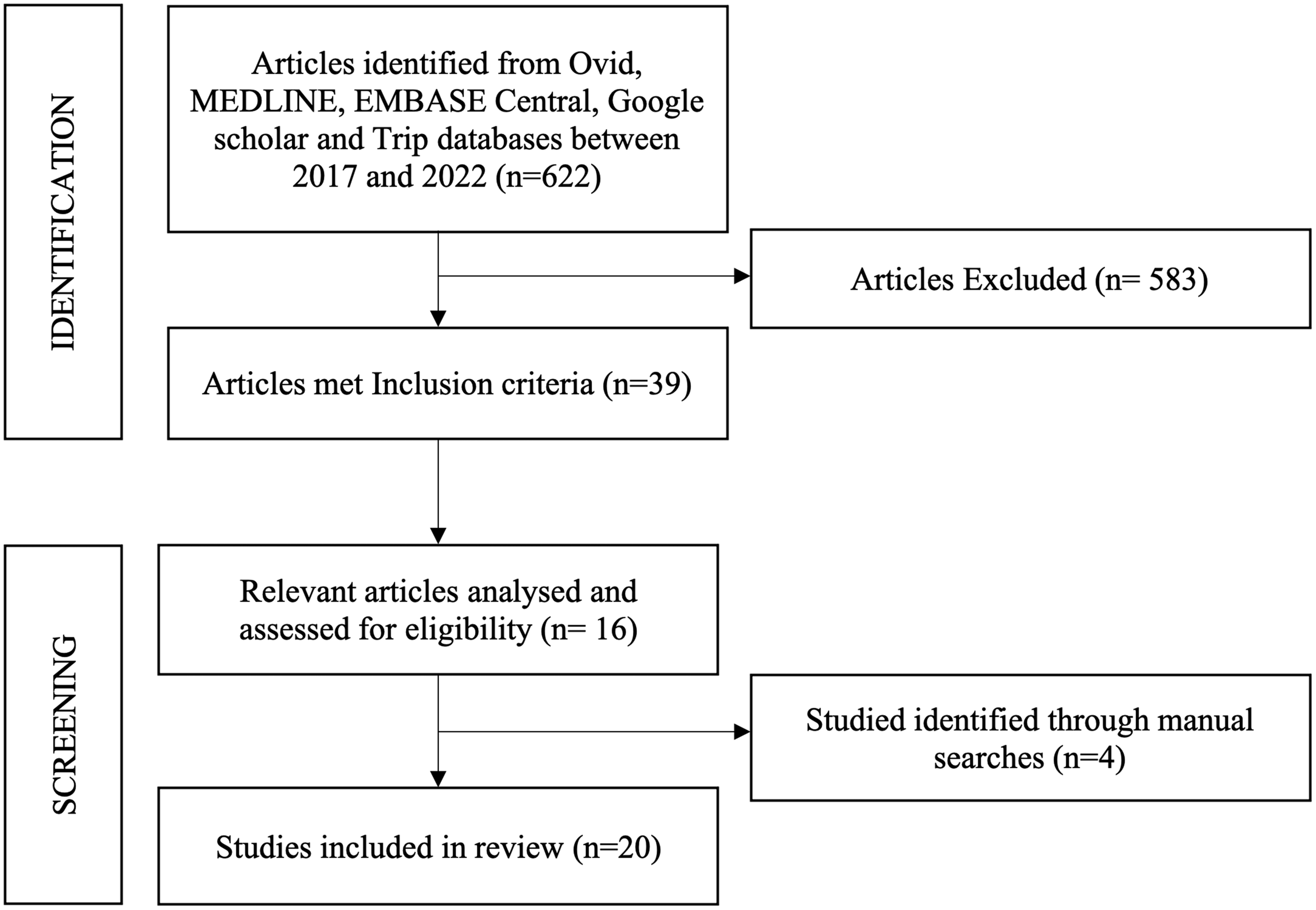
Preferred reporting items for systematic reviews and meta-analyses (PRISMA) flow diagram of search results.
Summary of the 20 articles included for analysis.
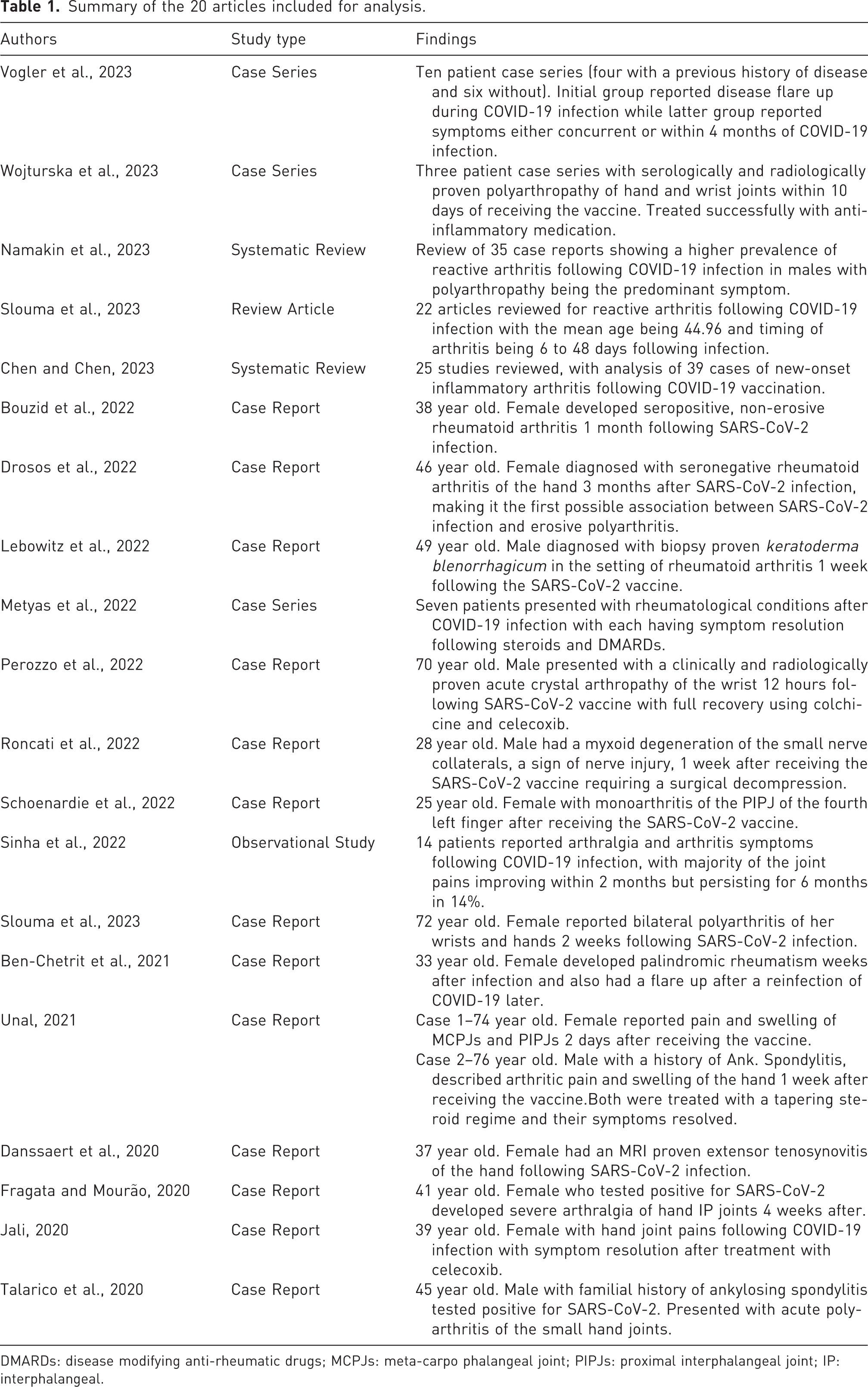
DMARDs: disease modifying anti-rheumatic drugs; MCPJs: meta-carpo phalangeal joint; PIPJs: proximal interphalangeal joint; IP: interphalangeal.
COVID-19 and arthritis
Reactive arthritis is a seronegative inflammatory arthropathy that causes an asymmetric mono-/oligoarticular arthritis occurring weeks after infection from bacterial pathogens, such as respiratory bacteria (Chlamydia pneumoniae, Staphylococcus aureus and Streptococcus pneumoniae) and viral infections (human immunodeficiency virus) (García-Kutzbach et al., 2018; Slouma et al., 2023; Varache et al., 2011). Our searches had identified four studies and two review articles, where the onset of reactive arthritis occurred from 12 to 16 days following SARS-CoV-2 infection with full resolution of symptoms after treatment (Danssaert et al., 2020; Fragata and Mourão, 2020; Jali, 2020; Vogler et al., 2023). Namakin et al. (2023) and Slouma et al. (2023) had suggested that the reactive arthritis caused by COVID-19 resolves quicker than bacterial triggers, with full recovery occurring after 16 days SD 57. It would be interesting to see whether a quicker resolution of symptoms is due specifically to the SARS-CoV-2 virus or whether other viral triggers resolve quicker than bacterial pathogens. Peripheral arthropathies, enthesitis and sacroiliitis were also commonly experienced after COVID-19 infection (Kim et al., 2009; Leirisalo-Repo, 2005; Ozgül et al., 2006; Selmi and Gershwin, 2014).
At present no causal evidence has been established between COVID-19 infection and reactive arthritis, but several immunological mechanisms post-infection have been suggested. The presence of HLA B27 antigen (Apaydin et al., 2021; Leirisalo-Repo, 2005; Ono et al., 2020), antigen-immune complex deposition in joints (Kim et al., 2009), dysregulation of toll-like receptors (TLR’s) (Cincinelli et al., 2021) and increased immunoglobulin levels (Sinaei et al., 2021) have all been implicated following COVID-19 infection. The presence of these antigens and immunoglobulins can then induce an autoimmune response to host synovium, via the mechanism of molecular mimicry. However, reactive arthritis in the hand and wrist is rare and difficult to diagnose compared with other forms of arthritis (Bekaryssova et al., 2022; Namakin et al., 2023; Vogler et al., 2023). It would be interesting to identify whether patients presenting with reactive arthritis had synovitis or tenosynovitis previously, where the virus could reactivate a fibrotic synovium rather than inducing the inflammation natively. Our review had also identified four reports of rheumatoid arthritis (RA) presenting 1 to 3 months following COVID-19 infection (Bouzid et al., 2022; Drosos et al., 2022; Metyas et al., 2022; Talarico et al., 2020). Two studies (Bouzid et al., 2022; Metyas et al., 2022) had diagnosed a new-onset RA post-COVID-19 infection in the hand and wrist. The other two studies had postulated that COVID-19 could lead to immune-mediated diseases, such as RA, due to the role pathogens play in colonizing joints (Mathew and Ravindran, 2014; Sun et al., 2020).
A reactive arthritis was seen between 1 and 10 days following vaccination in four articles analysed in our review (Chen and Chen, 2023; Lebowitz et al., 2022; Unal Enginar, 2021; Wojturska et al., 2023). Chen and Chen (2023) also identified a new onset of inflammatory arthritis following COVID-19 vaccination. As the vaccine is an attenuated strain of SARS-CoV-2, similar immune responses would occur as with the viral infection. However, what is not known is whether the reaction is due to the attenuated virus or from other components within the vaccine.
Our searches had also found a case report describing a flare up of crystalline arthropathy (CA) in the wrist post vaccination, secondary to the non-aluminium adjuvants within the vaccine (Perozzo et al., 2022). These contents have also been shown to cause reactions seen with the respiratory syncitial virus (RSV) vaccine (Eisenbarth et al., 2008). The flare ups of CA following COVID-19 were shown to have comparable morbidity and management as with other autoimmune rheumatic diseases, therefore CA occurring independent of COVID-19 cannot be excluded (D'Silva et al., 2020; Gianfrancesco et al., 2020; Hyrich and Machado, 2021).
COVID-19 and peripheral neuropathies
This review had found one case of cubital tunnel syndrome occurring 1 week following vaccination that was treated with a decompression (Roncati et al., 2022). Histological samples from the decompression had shown a myxoid degeneration of nerve branches, suggestive of an intrinsic nerve injury.
Peripheral nerve injuries were also commonly seen post-COVID-19 infection, with symptoms of anosmia, ageusia and facial nerve palsies reported, excluding prone positioning plexopathies (Lima et al., 2020; Namavarian et al., 2023). Other coronavirus family members, (SARS-CoV-1 and MERS-CoV) have been reported to cause an axonopathic polyneuropathy secondary to ischaemic damage to the vasa nervorum leading to symptoms of paralysis and myopathies (Gholami et al., 2021). Indeed, it has been documented that 8.9% of 214 hospitalized COVID-19 patients in China, had peripheral nerve symptoms (Mao et al., 2020). There have also been documented cases of Guillain–Barré syndrome and facial nerve involvement with COVID-19 and vaccines (Ellul et al., 2020). We suggest that the SARS-CoV-2 virus can cause peripheral neuropathies through the same mechanisms, with further neuronal damage from a secondary severe immune response described with other viral infections (Brizzi and Lyons, 2014; Castelli et al., 2020; Lima et al., 2020; Mangus et al., 2014; Namavarian et al., 2022; Pardo et al., 2001; Spiegel et al., 2006). We also propose that irritation, inflammation and scarring of surrounding soft tissues can cause extrinsic nerve compression, therefore surgical decompression can successfully relieve symptoms. However, surgical decompression may not improve symptoms if an intrinsic nerve injury has occurred. It would be interesting to see whether patients suffering from carpal or cubital tunnel syndrome post-COVID-19 infection have a relief of symptoms following surgical decompression.
COVID-19 and myositis
Our searches did not highlight any studies linking COVID-19 to myositis, however, myalgia was a common complaint with one study noting a rise in creatinine kinase (CK) levels (Suh et al., 2021). In some initial presentations of COVID-19, rhabdomyolysis has been diagnosed in some studies, suggesting that a more severe inflammatory insult occurs with COVID-19 than previous viruses (Jin and Tong, 2020; Suwanwongse and Shabarek, 2020; Valente-Acosta et al., 2020). The authors suggest that the myositis and rhabdomyolysis could be related to the presence of ACE-2 receptors on skeletal muscles cells, the same receptor found in the pulmonary epithelium (Lu et al., 2020; Zhou et al., 2020). Biopsies of the iliopsoas in patients with COVID-19 had demonstrated an inflammatory response that was not found in patients without COVID-19 (Suh et al., 2021). This finding supports our suggestion that SARS-CoV-2 causes direct muscular inflammation.
Tendinopathies in the hand and wrist result from chronic inflammatory changes that cause angiofibroblastic hyperplasia before resulting in fibrosis and calcification (Cooper, 2014). We propose that the SARS-CoV-2 virus could be the trigger that induces tendinopathies of the hand.
Conclusion
This review has found that the association of the virus or the vaccine with benign pathologies in the hand and wrist are increasingly reported in the literature. Despite public knowledge of COVID-19 only beginning in 2019, the basic scientific theories associated with COVID-19 are similarly seen with other viral infections from the coronavirus family. This review highlights that other viral infections have shown to induce the same systemic responses that could lead to common benign hand pathologies being a sequela of COVID-19.
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.