
Abstract
Distal radial fractures represent the most common fractures of the upper extremity. Operative treatment is performed for approximately one-third of distal radial fractures in the adult population. Complications following operative treatment of distal radial fractures vary depending on the treatment modality and can be stratified into preoperative and postoperative complications. Complications can occur in the near, intermediate and long term. The most common complications seen are tendon irritation and rupture, chronic regional pain syndrome (CRPS), carpal tunnel syndrome, ulnar or radial neuropathy, compartment syndrome, malunion, inadequate fixation or loss of fixation, symptomatic hardware, post-traumatic arthritis, stiffness and infection. Careful planning, treatment and patient selection can help to mitigate these complications.
Keywords
Introduction
Epidemiology
Fractures of the distal radius account for 18% of fractures in the elderly population (patients >65 years of age) and are the most common injury in non-elderly adults (Court-Brown and Caesar, 2006; Karl et al., 2015; Nellans et al., 2012). Recent population-based and database studies demonstrate an increase in the incidence of distal radial fractures over time, particularly in women over the age of 55 years (de Putter et al., 2011; Kakar et al., 2022; Khosla et al., 2003; Melton et al., 1998; Nellans et al., 2012).
Treatment of distal radial fractures
Treatment of distal radial fractures includes closed reduction and splinting, closed reduction and percutaneous pinning (PP), external fixation and open reduction and internal fixation (ORIF). ORIF options include volar or dorsal plating, fragment-specific fixation, intramedullary devices and bridge plating (Johannes et al., 2012). While there has been no strong evidence to support a difference in radiographic or patient-reported outcomes between different fixation techniques, volar locking plates have been shown to lead to earlier recovery of function (American Academy of Orthopaedic Surgeons/American Society for Surgery of the Hand, 2020; Combined Randomised and Observational Study of Surgery for Fractures in the Distal Radius in the Elderly (CROSSFIRE) Study Group et al., 2021; Goehre et al., 2014; Hammer et al., 2019; Jakubietz et al., 2012; Marcheix et al., 2010; Rozental et al., 2009; Yazdanshenas et al., 2019). Eighteen per cent of elderly and 36% of all adult patients undergo operative treatment of distal radial fractures, with volar plate fixation being the most common fixation method (Chung et al., 2011; Kakar et al., 2022). Recent consensus guidelines by the American Academy of Orthopedic Surgeons (AAOS) recommended operative treatment for non-elderly patients in the setting of post-reduction radial shortening >3 mm, dorsal tilt >10°, intra-articular displacement or step off >2 mm (American Academy of Orthopaedic Surgeons/American Society for Surgery of the Hand, 2020). Other indications for operative treatment of adult distal radial fractures include an open fracture, fracture dislocation, displaced shear fractures, associated neurovascular injuries, compartment syndrome or polytrauma (Egol et al., 2010; Lafontaine et al., 1989). In elderly patients, the AAOS consensus committee had strong recommendations that operative treatment does not improve outcomes compared with non-operative treatment (American Academy of Orthopaedic Surgeons/American Society for Surgery of the Hand, 2020; Arora et al., 2011). Surgical decisions should be made with the individual patients' function and demands considered.
Complications before operative intervention
Before surgical fixation of a distal radius is performed, closed reduction of displaced fractures is common practice in the emergency department. Following closed reduction, immobilization in a flexion position can increase pressure in the carpal tunnel and lead to median neuropathy (Gelberman et al., 1984; Seigerman et al., 2019). Surgical timing and a fixation strategy must be established if operative intervention is indicated. Failure to adequately recognize fracture patterns (intra-articular, proximal extension, ulnar fractures) and associated injuries (nerve, carpal, interosseous membrane, distal radioulnar joint (DRUJ), Essex-Lopresti, etc.) will affect the operative outcomes. For closed fractures, equivalent complication rates and patient outcomes have been found in patients who received surgery within 2 weeks and after 2 weeks from the time of injury (Howard et al., 2021; Yu et al., 2011). For open distal radial fractures, no difference in infection was seen based on time to debridement of greater or less than 6 hours (Kurylo et al., 2011).
Overview of operative complications
The overall rate of complications of all operative treatment methods in patients over 65 years of age is estimated to be 29%. Surgical or pin site infection was the most common complication in 12% of operatively treated patients. Other complications included median neuropathy (8%), tendon rupture (3.8%), complex regional pain syndrome (CRPS) (3%), tendon adhesions/scarring (2.3%), ulnar nerve compression (2.3%), DRUJ complications (1.5%), carpal instability (<1%), radial sensory nerve branch irritation (<1%) and delayed union (<1%) (Lutz et al., 2014). Complications associated with volar plate fixation most commonly include tendon issues (3.4%), CRPS (2.2%), acute carpal tunnel syndrome (2%), hardware complications (1.9%), displacement or inadequate reduction (1.5%) and infection (<1%) (Johnson et al., 2014). This review aims to detail distal radius complications over time.
Early complications (<90 days after surgery)
Nerve
Acute median neuropathy may occur after operative and non-operative distal radial fracture treatment. Carpal tunnel syndrome is estimated to occur in 2–14% of patients after volar plate fixation (Berglund and Messer, 2009; Drobetz and Kutscha-Lissberg, 2003; Hove et al., 1997). Carpal tunnel release during volar plate fixation should be considered in patients with pre-existing carpal tunnel syndrome, symptoms of median neuropathy secondary to the trauma (Berglund and Messer, 2009; Lattmann et al., 2008) and for patients who may be at increased risk for carpal tunnel syndrome postoperatively, such as those with an ipsilateral upper extremity injury and fracture translation greater than 35% (Seigerman et al., 2019). Carpal tunnel release can be performed simultaneously with volar plate fixation through an extended flexor carpi radialis (FCR) approach or a separate incision. To reduce the risk of median nerve injury during volar plate fixation, avoiding excessive traction on the median nerve and palmarly flexing the wrist during the distal ulnar screw placement has been recommended (Berglund and Messer, 2009) . Careful dissection should be performed as the palmar cutaneous branch of the median nerve, which lies just deep to the ulnar border of the FCR, can be damaged during the surgical approach for volar plate fixation (Berglund and Messer, 2009; Seigerman et al., 2019). Carpal tunnel syndrome may also present as a late complication of volar plate fixation, occurring in 2.1% of patients at a mean of 7 months after surgery (Peter et al., 2012). If non-operative measures fail to resolve the symptoms, carpal tunnel release, median nerve neurolysis and hardware removal can be performed (Peter et al., 2012).
The superficial branch of the radial nerve (SBRN) has a variable course and is at risk for injury during operative treatment of distal radial fractures. Although paraesthesias are rare following volar plate fixation, neuropraxia can occur due to traction on the nerve during reduction manoeuvres and injury can occur from penetration with K-wire utilized for maintaining fracture reduction or during pin insertion for external fixation (Berglund and Messer, 2009; Hove et al., 1997; Peter et al., 2012). A limited open technique during pin or wire fixation and the use of wire driver oscillation has been suggested to minimize the risk to the SBRN (Korcek and Wongworawat, 2011).
Compared with median and radial nerve injury, ulnar nerve injury is rare and may occur at the time of injury or during surgical treatment of an associated ulnar fracture. Discussion of ulnar nerve palsy following distal radial fracture are mostly limited to case reports. Soong and Ring (2007) described five patients who developed complete motor and sensory ulnar nerve palsy following distal radial fracture, all of which were high energy injuries with significant displacement. They noted that these injuries were typically neuropraxic and complete or near-complete recovery was common. Additionally, they recommended exploration when associated with an open injury or acute carpal tunnel syndrome, but observation when occurring alone.
Compartment syndrome
Compartment syndrome of the forearm can occur following isolated distal radial fracture but more commonly occurs in combination with other injuries. It is 50 times more likely to develop in the setting of an unstable ipsilateral elbow fracture than in isolated distal radial fractures (Hwang et al., 2009). Hwang et al. (2009) identified 59 patients with an operatively treated distal radial fracture and an ipsilateral elbow injury, nine of whom developed forearm compartment syndrome with three of those being after volar plate fixation. When compartment syndrome developed after surgery, it developed at 18, 22 and 40 hours postoperatively (Hwang et al., 2009). Other studies note compartment syndrome rates of 0.1–5% after ORIF, depending on the injury severity (Hove et al., 1997; Hwang et al., 2009). Careful consideration should be given to using long-acting regional anaesthesia when concern exists for compartment syndrome or peripheral neuropathy. Return to the operating room for fasciotomy is recommended.
Wound complications/infection
The overall incidence of infection after operative treatment of distal radial fracture is 0.9%, with rates of 1.3% after percutaneous treatment compared with 0.8% with open treatment in a large database study of 87,169 patients (Constantine et al., 2022). Infection rates are lower in buried wires compared with percutaneously inserted wires and in wires removed prior to 8 weeks after insertion (Hargreaves et al., 2004). Risk factors for infection include male gender, open fracture, lung disease, chronic kidney disease, diabetes, hypertension, liver disease, tobacco use and obesity (Constantine et al., 2022). After propensity matching the cohorts, tobacco use was the only condition that significantly increased the risk of infection at an odds ratio of 1.31 (1.05–1.64, p value 0.17), while open fracture was the strongest predictor of postoperative infection (Constantine et al., 2022). Infection led to a significantly increased cost of care, with infection costing $5543 more than treatment without infection (Constantine et al., 2022). Deep infection after distal radial fracture volar plate fixation presents anywhere from 5 days to 5 months following surgery and can be successfully eradicated with debridement, removal of hardware and antibiotics, but patient-reported outcomes are negatively affected (Henry et al., 2021).
In the setting of open distal radial fractures, initial wound severity and contamination have been associated with reported postoperative complications and infection incidence. Rozental et al. (2002) found that increasing wound severity was associated with a higher number of surgeries after initial treatment and reported on three patients who required flap coverage of their wound. No increased wound complications are seen if multiple incisions are needed during distal radial fracture reconstruction and fixation (Meaike et al., 2021).
Failure of reduction
The failure of reduction as a complication is a delicate subject, as it relates to what the surgeon accepted or failed to recognize. Acceptable intraoperative reduction of distal radial fractures should meet the following criteria: radial shortening <5 mm, radial inclination >15°, sagittal tilt on lateral projection between 15° dorsal tilt and 20° volar tilt, intra-articular step off <2 mm in the radiocarpal joint and articular congruity <2 mm of the sigmoid notch of the distal radius (Nana et al., 2005). Inadequate fracture visualization is the most common reason for failure to achieve reduction (Berglund and Messer, 2009).
Progressive loss of reduction can occur secondary to dorsal collapse, loss of radial length or loss of lunate facet reduction and can lead to malunion, nonunion or post-traumatic arthritis (Berglund and Messer, 2009). As described by Medoff, understanding and recognizing common fracture fragments present in distal radial fractures is important in achieving adequate reduction (Medoff, 2005; Peter et al., 2012) (Figure 1
Schematic demonstrating fragments of intra-articular distal radial fracture including volar rim, dorsal ulnar corner, dorsal wall and radial column. (From Figure 2. Rhee PC, Medoff RJ, Shin AY. Complex distal radius fractures: an anatomic algorithm for surgical management. JAAOS. 2017, 25: 77–88.)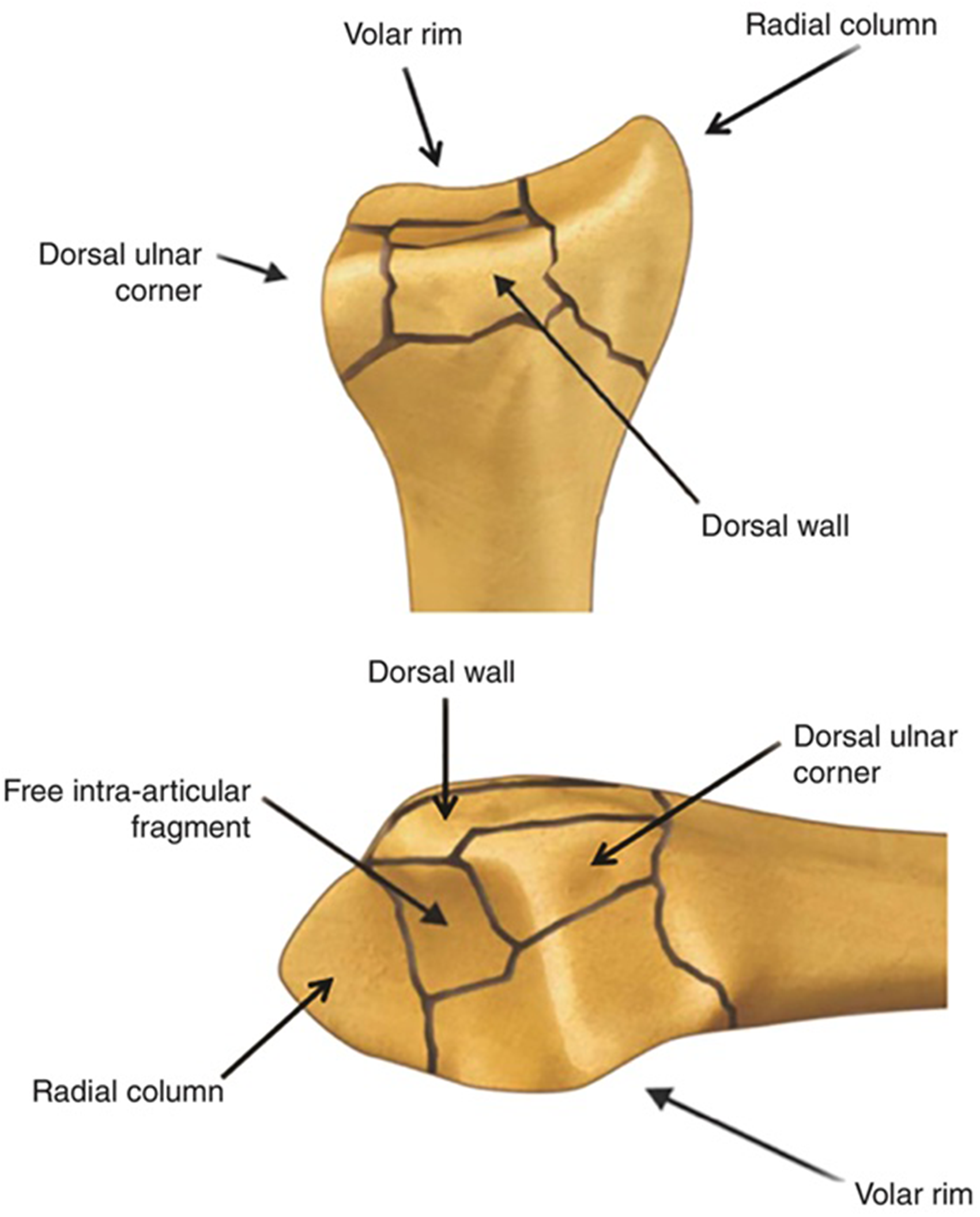

(a) CT scan appearance of volar lunate facet piece. (b) and (c) Postoperative CT scan images demonstrating malreduction of intra-articular volar rim fragment.
(a) Anteroposterior and (b) lateral radiographs of volar carpal collapse after volar plate fixation.
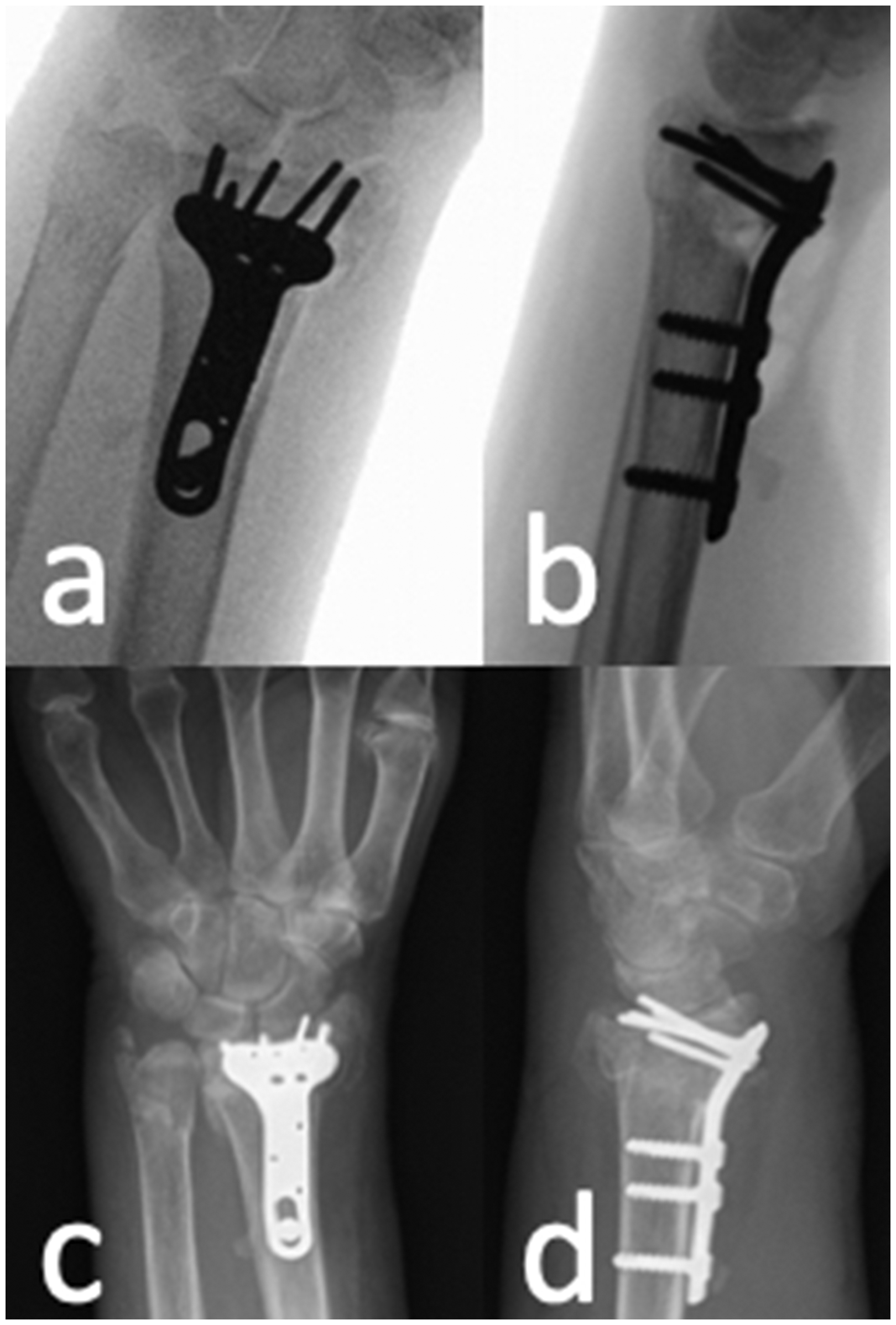
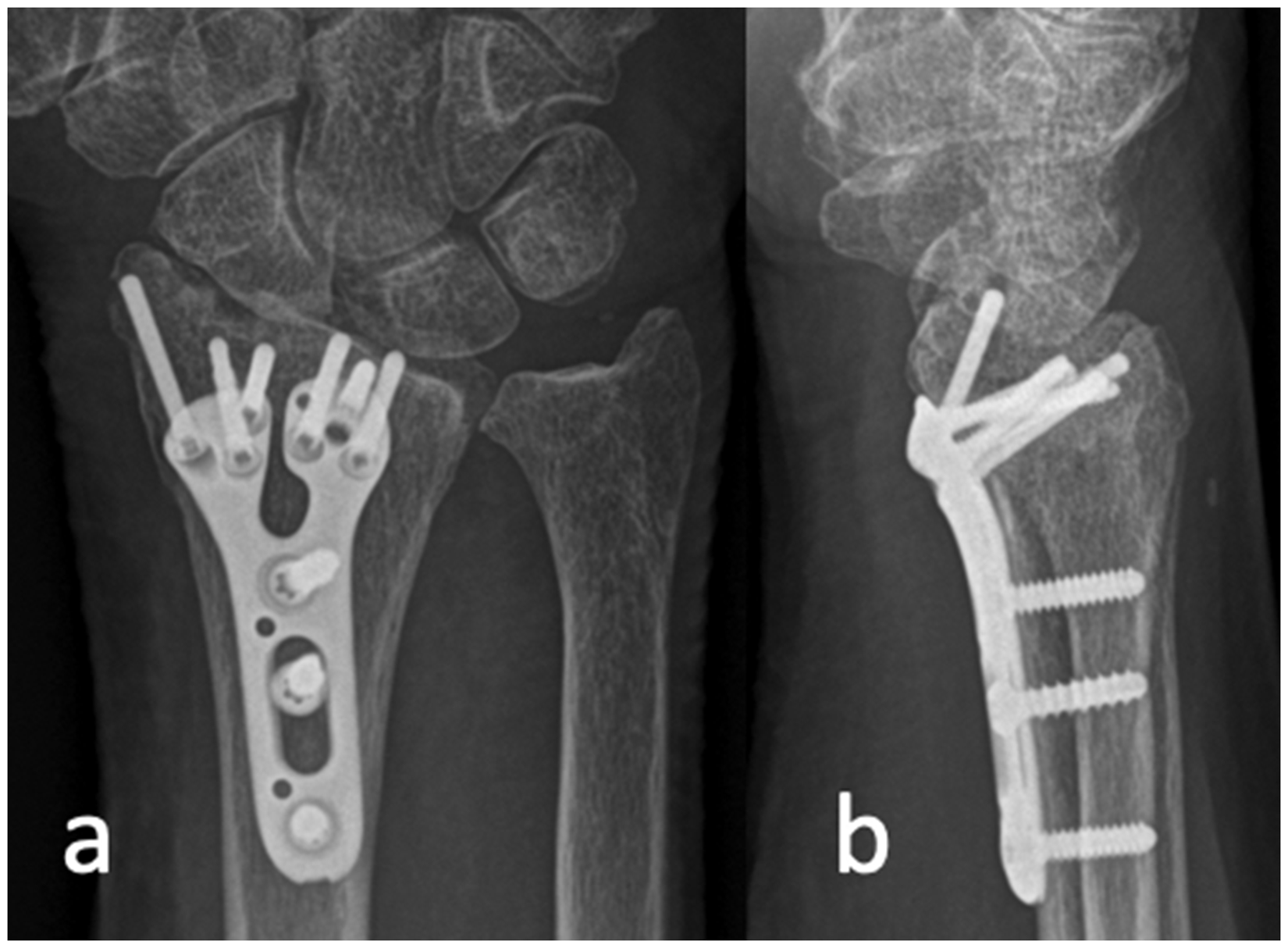
(a) Anteroposterior and (b) lateral intraoperative fluoroscopic images of distal radial fracture fixed with volar locking plate. (c) and (d) Radiographs 2 weeks postoperatively demonstrating intra-articular screw penetration secondary to dorsal collapse.
The dorsal ulnar corner of the intra-articular fracture should be approximated congruously to prevent destabilizing of the DRUJ. Incongruous reduction of this fragment can lead to prominence of the distal ulna during forearm pronation due to volar ulnar translation of the distal radius (Hozack and Tosti, 2019). Failure to apply adequate fixation to a radial styloid fragment can lead to the displacement of this fragment and may require revision surgery with a radial styloid plate (Johnson et al., 2014). Coronal malalignment (radial translation of the radius) can result in DRUJ instability and should be corrected (Dy et al., 2014). Dorsal rim fractures can usually be treated successfully with volar plating if displacement is <2 mm (Kim et al., 2016).
Articular impaction is also an important component of the intra-articular distal radial fracture. Failure to recognize this and restore a congruous joint surface increases the risk of post-traumatic arthritis and decreased range of motion (Erhart et al., 2013). Residual intra-articular displacement with gaps of 2 mm or a step off of 1 mm or greater is associated with a higher rate of postoperative complications (Berglund and Messer, 2009; Johnson et al., 2014). Fragment specific fixation, in which implants or techniques designed to capture each of these fragments, can be used alone or with other standard techniques to help reduce and stabilize complex intra-articular distal radial fractures (Hozack and Tosti, 2019). The most common complication following fragment specific fixation is tendon irritation related to hardware (Hozack and Tosti, 2019; O'Shaughnessy et al., 2016).
Hardware complications
Hardware complications can occur in 0–1.9% of patients treated with volar locking plates and can include symptomatic hardware or intra-articular screws in the radiocarpal or DRUJ (Johnson et al., 2014). Intra-articular screw placement has been reported in 1.3% of volar plate fixation (Soong et al., 2011b). Several intra-operative imaging techniques can be used to assess for intra-articular screw placement including the tilted lateral image, a 45° pronated oblique image or continuous, rotational intraoperative fluoroscopy (Peter et al., 2012). Soong et al. (2008) suggested placing the ulnar most screws first as the styloid screw may interfere with subsequent lateral views. Soong et al. (2011b) reported four of 594 (0.7%) patients experienced symptomatic, prominent hardware that most commonly presented as prominent screws, treated by screw or hardware removal after fracture healing if desired by the patient. Immunologically active metals used in orthopaedic hardware can cause metal hypersensitivity (MHS) reactions, most commonly presenting as allergic contact dermatitis, delayed wound healing and/or recurrent wound problems (Baumann and Crist, 2020). While no case reports have been written for this phenomenon following distal radial fracture fixation, suspected MHS have been described following other forearm implants, resulting in chronic pain at the site of the implant 1 year following surgery that resolved on implant removal (Dmochowski et al., 2019).
Early tendon complications
Extensor pollicis tendon (EPL) rupture is reported to occur in up to 5% of non-displaced distal radial fractures (Roth et al., 2012) (Figure 5). EPL rupture is estimated to occur in 1.7% of patients treated with volar plate fixation at an average of 49.8 days from surgery (Johnson et al., 2014; Zenke et al., 2013). Proposed mechanisms for EPL rupture in this setting include prominent screws (Figure 6), prominent bone spurs and dorsal gapping at the fracture site (Benson et al., 2006). Extensor tenosynovitis occurred in four out of 141 patients treated with volar plating (Arora et al., 2011). Precise drilling without plunging, drilling to but not through the dorsal cortex and unicortical screw placement is suggested to help prevent these complications. Locked unicortical screws of 75% or more length have similar construct stiffness to bicortical screws in osteoporotic fractures and can be used to help prevent extensor tendon irritation during volar plate fixation (Wall et al., 2012). When percutaneous pins are used to stabilize distal radial fracture, the estimated incidence of extensor tendon rupture is 0.7%. Several strategies have been recommended to mitigate this risk, including avoiding K-wire placement 5 mm ulnar to Lister’s tubercle and entering the radial styloid through a small incision (Seigerman et al., 2019).
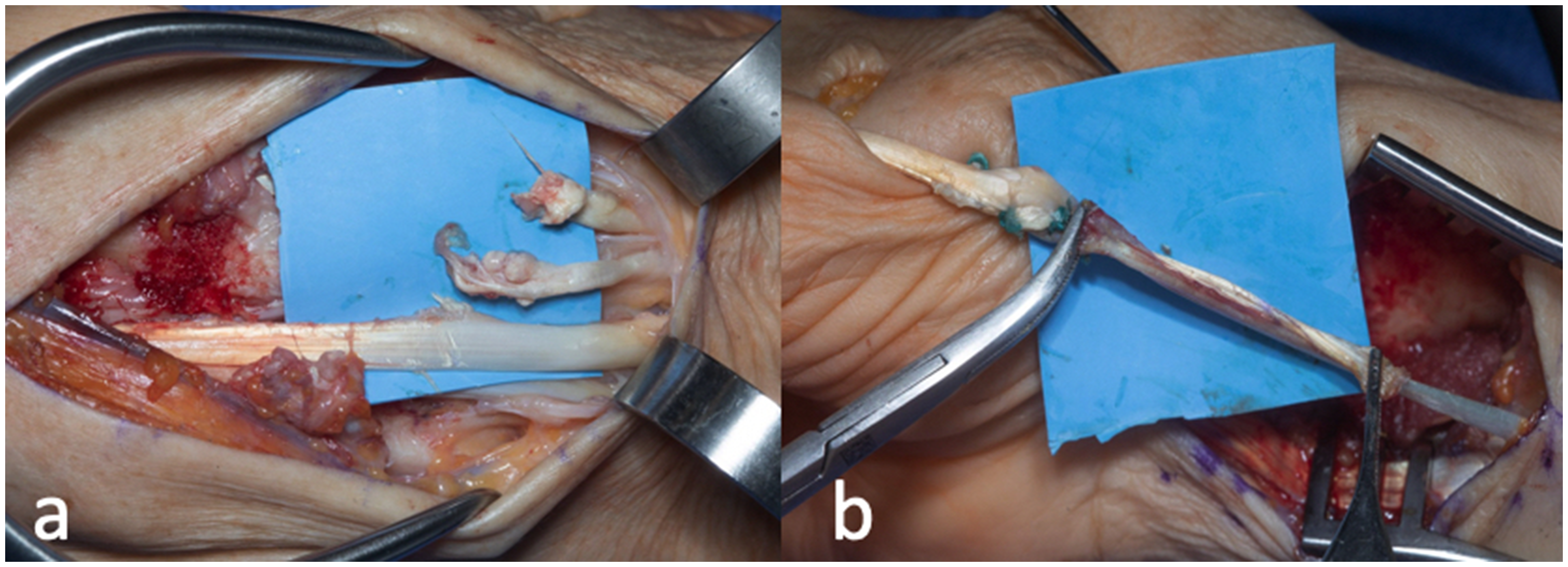
(a) Ruptures of extensor pollicis longus (EPL) and extensor digitorum communis and extensor indicis proprius to the index finger and (b) EPL reconstruction with palmaris longus rerouted with extensor carpi radialis brevis.
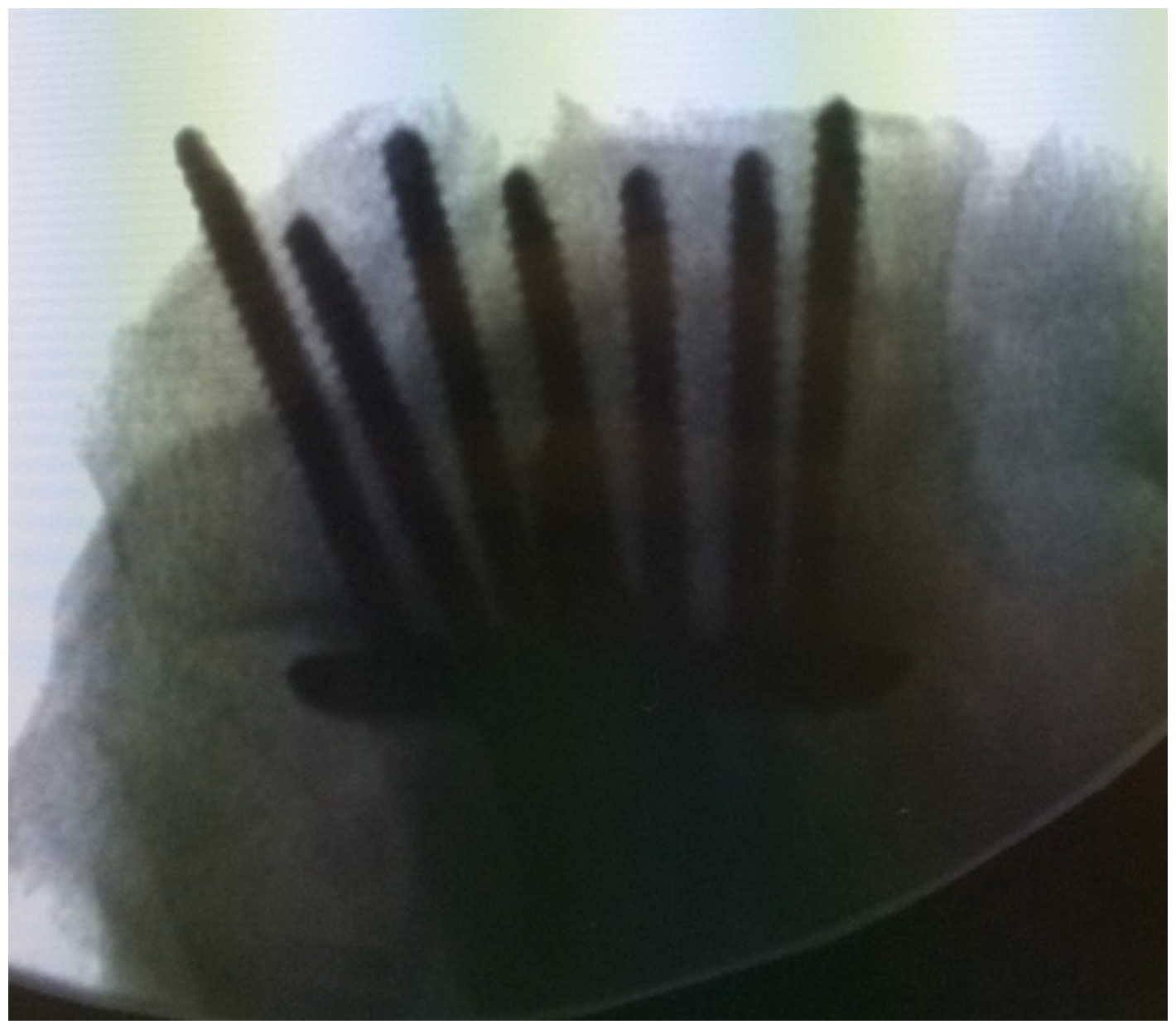
Prominent dorsal screws visualized intraoperatively.
CRPS
CRPS type 1 can develop after operative and non-operative treatment of distal radial fractures and is estimated to occur in 2.2–6% of distal radial fractures treated with volar locking plate (Johnson et al., 2014; Lattmann et al., 2008). A population-based study of 172,194 operatively treated distal radial fractures demonstrated an incidence rate of 0.65%. This was diagnosed at an average of 97 days SD 84 following surgery (Jo et al., 2019). Compared with patients without CRPS, patients who develop CRPS are more likely to have been treated with surgery, mostly underwent open reduction, have rheumatoid arthritis, be female, have accompanying ulnar fracture or sustained an open fracture (Dutton and Rhee, 2021; Jo et al., 2019). Treatment and prevention of CRPS continues to be controversial. A recent double-blind, placebo-controlled randomized trial did not support earlier evidence that suggested vitamin C administration can reduce the prevalence of CRPS (Aïm et al., 2017). Proposed treatments include early aggressive treatment with physical therapy, pain management and oedema control to prevent the long-term complications of CRPS (Dutton and Rhee, 2021).
Midterm complications (>90 days)
Stiffness
Kong et al. (2020) examined a group of 119 patients who underwent volar plate fixation for distal radial fracture and found radiocarpal joint stiffness present in 35% of patients. Factors associated with increased risk of stiffness included severe preoperative swelling, intra-articular fracture, non-participation in prescribed rehabilitation exercises and postoperative volar tilt (Kong et al., 2020). Rozental et al. (2002) found that all patients developed some stiffness after open distal radial fracture, with an average flexion–extension arc of motion of 81°. Stiffness can also occur in supination and pronation. Soong et al. (2011b) examined late complications (>6 months) in 321 patients treated with volar plate fixation and found three patients with severe forearm stiffness, two of whom required resection of the distal ulna. Despite an increased risk of swelling of the fingers in the early postoperative period (Aïm et al., 2017) for Arbeitsgemeinschaft fur Osteosynthesefragen (AO) type B and C distal radial fractures, a better range of motion and grip strength is observed in patients treated with volar plate fixation compared with non-operative treatment (Sharma et al., 2014). Early participation in a therapy programme to work on digit and wrist range of motion may be helpful to reduce these complications (Ikpeze et al., 2016).
Delayed tendon complications
Flexor tenosynovitis and tendon ruptures are recognized complications of volar locked plating systems, with flexor pollicis longus (FPL) being the most commonly affected (Figure 7). Flexor tenosynovitis is estimated to occur in 7.9% of patients. FPL rupture is estimated to occur in 2–12% of patients (Arora et al., 2011; Drobetz and Kutscha-Lissberg, 2003; Johnson et al., 2014). Soong et al. (2011a) developed a volar plate prominence classification system and found that patients with more volarly prominent plates were at higher risk for flexor tendon rupture. DeGeorge et al. (2020) found that the Soong grade correlated with the adequacy of fracture reduction, with Soong Grade 1 being associated with the most adequate fracture reduction and plate positioning. They noted that the adequacy of the fracture reduction rather than the position of the plate was the driver of tendon complications following volar plate fixation. If tendon irritation is encountered, volar plates can be removed (Peter et al., 2012).
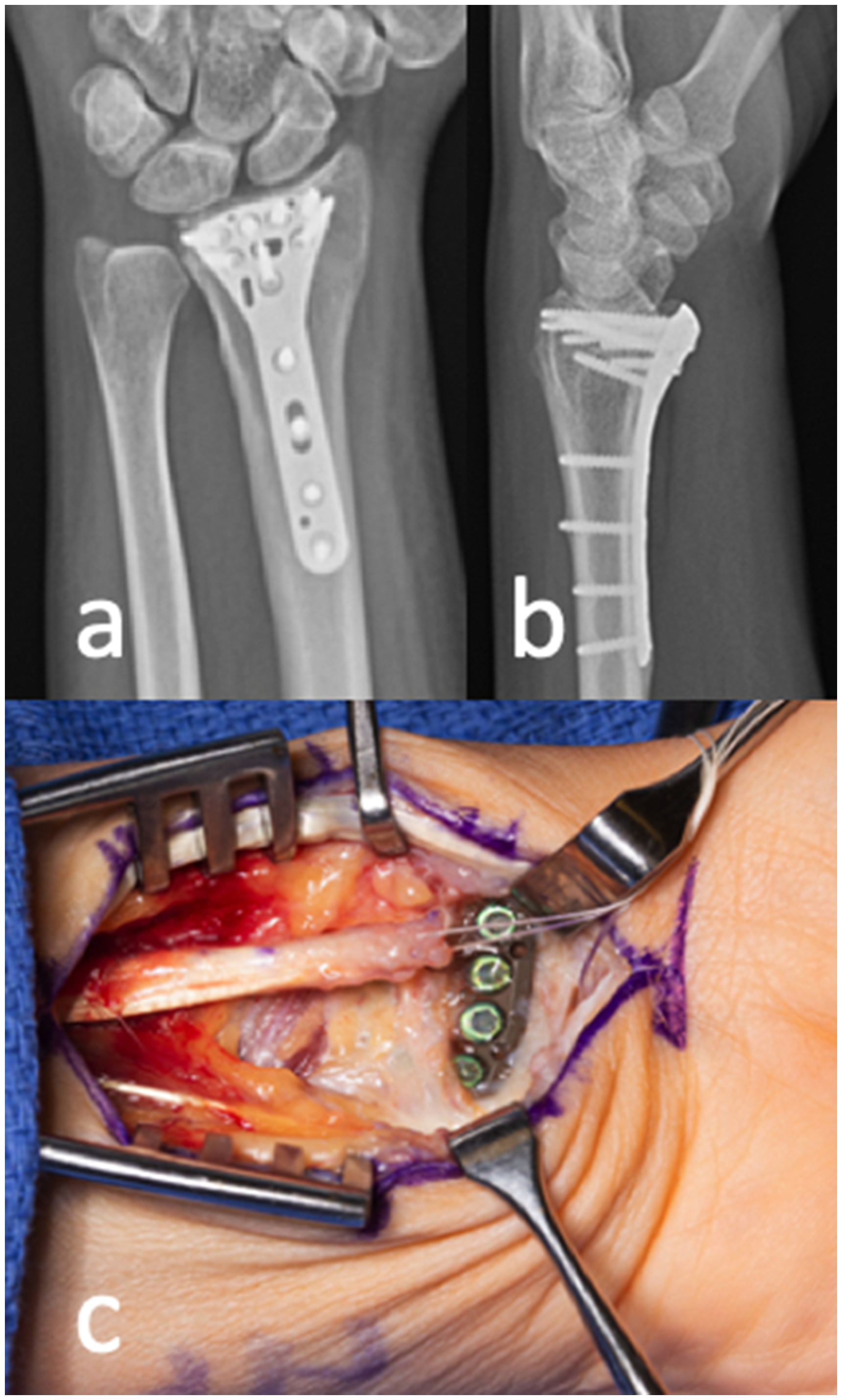
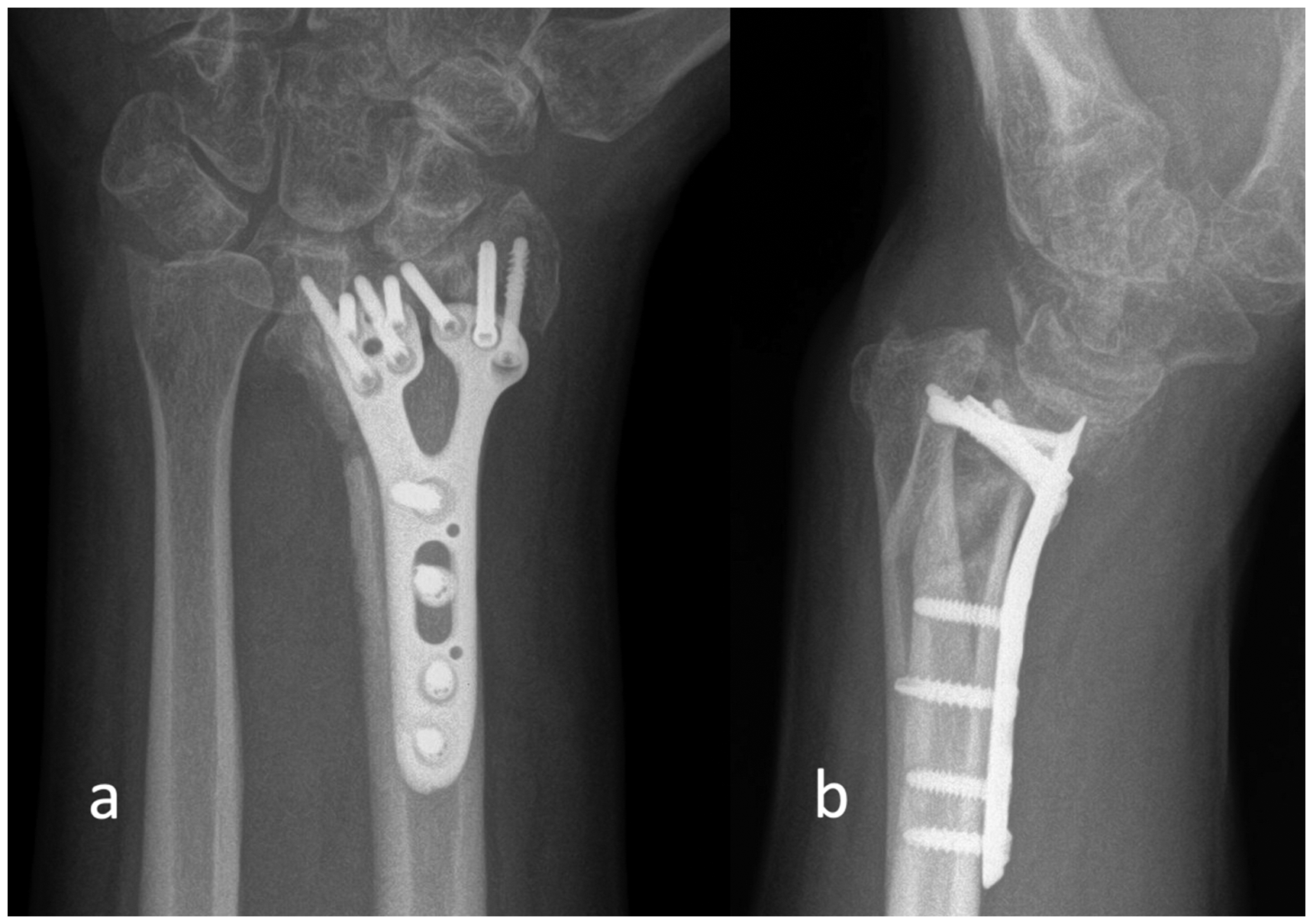
(a) Anteroposterior and (b) lateral radiographs and intraoperative photograph of a patient who sustained a rupture of their flexor pollicis longus tendon 5 years following volar plate fixation for distal radial fracture.
After dorsal plating, there is an estimated 14–25% rate of extensor tendon irritation and up to 1.3% rate of extensor tendon rupture, which occurs at an average of 6 months after surgery (Axelrod and McMurtry, 1990; Rein et al., 2007; Ring et al., 1997; Sánchez et al., 2005). Hardware removal for extensor tendon irritation is also common, occurring in 8–25% of patients (Carter et al., 1998). Some recommend routine plate removal 4 to 6 months after dorsal plating to minimize extensor tendon irritations (Rein et al., 2007). However, many of the extensor tendon irritations, ruptures and hardware removal were seen with thicker plates (2 mm) and more recent studies have demonstrated no tendon irritation or rupture after dorsal plating with low-profile, anatomically pre-contoured plates (Simic et al., 2006).
Additional injuries
Fractures of the adjacent ulna and the surrounding carpal bones can occur along with distal radial fractures. Ulna fractures are reported to occur in combination with 6% of fractures of distal radius (Dennison, 2007). Several recent studies have shown no difference in patient-reported outcomes, range of motion, complication rates or secondary procedures between operative and non-operative treatment of associated distal ulnar fractures when operative treatment of the distal radial fracture is performed (Glogovac et al., 2022; Kurozumi et al., 2021).
Additional soft tissue injuries include disruption to the scapholunate (SL) ligament (16–40%), luntotriquetral (LT) ligament (9–15%) and triangular fibrocartilage complex (TFCC) (39–43%) (Shahabpour et al., 2021). Differences in functional outcomes between patients with and without SL ligament injuries who do not undergo repair for their SL injury have not been demonstrated (Klifto et al., 2021; Mrkonjic et al., 2015). TFCC injuries are common in distal radial fracture, usually caused by displacement or shortening of the distal radial fracture component causing either disruption of the TFCC or ulnar styloid, and occurs concomitantly in up to 84% of cases and can be associated with DRUJ instability (Nuelle, 2022). Consideration should be given to examination of the DRUJ stability under anaesthesia during surgical treatment of a distal radial fracture. Persistent DRUJ instability can lead to ulnar-sided wrist pain, and treatment can include a trial of non-operative management followed by surgical management if non-operative treatment fails (Nuelle, 2022).
Long-term complications
Arthritis
Post-traumatic arthritis is more common in intra-articular fractures or those that heal in a malunited position. In patients who sustained intra-articular distal radial fractures and were treated with ORIF, post-traumatic arthritis was 76% at 7 years and 81% at 15 years (Catalano et al., 1997). When looking at elderly patients, the prevalence of post-traumatic osteoarthritis at 12 months was 34% in the operative group compared with 80% in the non-operative group (Egol et al., 2010). There is a significant risk of arthrosis in fractures that heal with an incongruous radiocarpal joint (91%) compared with radiocarpal congruity (11%), indicating that restoration of the articular surface is the most important factor for decreasing the risk of arthritis (Knirk and Jupiter, 1986) (Figure 8).
(a) Anteroposterior and (b) lateral radiographs demonstrating malreduction of the intra-articular fracture fragments leading to radiocarpal arthritis that was treated with total wrist arthrodesis.
DRUJ instability/arthritis/malunion
DRUJ arthritis after distal radial fracture has been reported to occur at rates of 11–19%. Several mechanisms of injury can lead to disruption of the DRUJ mechanics leading to instability or arthritis after distal radial fracture, including fracture extension into the sigmoid fossa, shortening of the distal radius relative to the ulna, TFCC injury, fracture of the ulnar styloid base and >2 mm displacement of an ulnar styloid fracture (Nana et al., 2005). Malunion can also contribute to DRUJ incongruity or ulnar impaction leading to decreased grip strength, decreased range of motion and increased pain (Mathews and Chung, 2015). Lutz et al. (2014) found that malunion following distal radial fracture treatment in the elderly is less common in operatively treated patients (29%) than non-operatively treated patients (69%). Chung et al. (2021) found malunion to occur in 8% of patients who underwent volar locking plate compared with 9.8% who underwent CRPP, 17% who underwent external fixation and 59% who were treated with casting. Malunion was associated with non-significantly worse functional scores and range of motion, and did not vary in employment or physical activity at 24 months (Chung et al., 2021). In the event of malunion, corrective osteotomy can be considered to restore alignment and improve biomechanics of the wrist. Several surgical techniques are available for management of DRUJ instability and arthritis.
Hardware complications
Removal of plates following distal radial fracture fixation occurs in 3–18% of patients and is more common in younger age groups (18–47 years) (Palola et al., 2021). Mean time after surgery for plate removal was 367 days (Palola et al., 2021). Most common reasons for hardware removal were tenosynovitis, tendon rupture, pain and prominent hardware or presence of intra-articular hardware (Gyuricza et al., 2011). Pain was found to be the only significant predictor of hardware removal in a cohort evaluated by Snoddy et al. (2015). In a study by Gyuricza et al. (2011), complications occurred during two plate removals; one screw was cross-threaded and had to be removed as a unit with the plate and another screw was stripped and the plate was cut and removed with the screw. In general, technical difficulties that can be encountered during hardware removal include stripped screw heads, cross-threaded screws and bony or fibrous overgrowth into the screw recess (Ehlinger et al., 2009). While hardware failure is uncommon, it can occur in instances of delayed union or improper reduction (Berglund and Messer, 2009). Nonunion is an uncommon complication following surgical treatment for distal radial fractures (Seigerman et al., 2019).
Conclusion
When operative treatment is indicated in the treatment of distal radial fracture, it is important to be aware of the preoperative and postoperative complications and their predicted time course so that prompt attention and treatment can be given. Thorough initial evaluation is important to ensure that the appropriate surgical treatment is selected to reduce the risk of inadequate initial reduction, reduce the risk of missed associated injuries or persistent nerve symptoms following surgery. Immediately after surgery, surgeons should be aware of complications, such as compartment syndrome, neuropathy, wound complications/infection, intra-articular hardware and failed reduction. Within the first 90 days after surgery, patients should be monitored for tendon irritation/rupture, stiffness and CRPS. After 90 days, symptomatic hardware, additional tendon complications and sequela from additional injuries should be monitored. Over the longer term, post-injury complications, such as radiocarpal or DRUJ arthritis and carpal adaptations to malunion may or may not be symptomatic.
While surgical treatment of distal radial fractures is more commonplace, hand and upper extremity surgeons must anticipate and prepare for the complications accompanying this increased prevalence of surgical fixation.
Footnotes
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Shin: (1) Editor in Chief, Techniques in Hand and Upper Extremity; (2) Royalties: Trimed orthopedics/Mayo medical ventures. Dr Pulos and Dr Townsley have no conflicting interests for this article.
Ethical approval declaration/IRB
No IRB required for this work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Consent was obtained from all study participants prior to inclusion in this study.