
Abstract
The aim of this single-centre retrospective study was to evaluate the outcomes of carpal tunnel release surgery in patients with hereditary neuropathy with pressure palsies (HNPP). The secondary aims were to identify prognostic factors for the outcome of carpal tunnel release and to assess the outcome of cubital tunnel release. Our primary hypothesis was postoperative improvement. In total, 18 patients (26 carpal tunnel releases) with at least one symptomatic carpal tunnel syndrome were included. At a median follow-up of 8.5 years, more than 73% of the patients were satisfied with the results. The visual analogue scale (0 to 10) for discomfort decreased by 2.2 points (p < 0.001). The Boston Carpal Tunnel Questionnaire symptom severity scale decreased by 1.3 points (p < 0.001). The decrease in the Functional Status Scale was not significant. No significant prognostic factor for outcome was identified. A total of 12 patients also underwent cubital tunnel release, and three patients underwent just this procedure (23 procedures). Despite the lack of preoperative data, cubital tunnel release provided encouraging results.
Keywords
Introduction
Hereditary neuropathy with liability to pressure palsies (HNPP) is an autosomal dominant condition caused by mutations in the PMP22 gene. Chronic, transient sensorimotor nerve palsies caused by nerve stretching or compression are typical, but the chronic clinical presentation is highly variable. Management focuses on postural prevention. Electromyography (EMG) often reveals multiple entrapment neuropathies, including carpal and cubital tunnel syndromes (CTS and CUTS, respectively), which may remain asymptomatic for long periods or become severely disabling at any age (Chance, 2006, 1999; Farrar et al., 2014; Guo et al., 2014; Takahashi et al., 2017), to the point of axonal degeneration (Moss et al., 2021). The standard of care for the latter is splinting, as the place of surgery in HNPP is debated due to the many case reports of neurological complications after various surgical procedures. Positive results after carpal or cubital tunnel release (CTR and CUTR, respectively) in patients with HNPP (Celik et al., 2008; Grossman et al., 2007; Lazar et al., 2007; Taggart and Allen, 2001) and remyelination on postoperative EMG (Earle and Zochodne, 2013) were described. However, none of these case reports either used specific scores or considered prognostic factors related to the surgery or the patients. A recent study reported postoperative clinical and EMG improvement after CTR, but poor results after CUTR (Chompoopong et al., 2022). The primary aim of our study was to evaluate the outcome of CTR using a specific score in patients with symptomatic HNPP. The secondary aims of the study were to identify prognostic factors for CTR outcomes and complications and to assess CUTR outcomes. Our main hypotheses were that specific scores would improve after CTR and that prognostic factors for poor postoperative outcomes could be identified.
Methods
This single-centre retrospective study was conducted between September 2021 and February 2022. We reviewed eligible patients with HNPP who had regular follow-ups at our referral centre. The inclusion criteria consisted of patients with a diagnosis of HNPP confirmed by genetic testing who underwent surgery for symptomatic CTS and/or CUTS confirmed by EMG (whose intensity was clearly distinguishable from any neuropathic background and resistant to medical treatment). The minimum follow-up was 1 year after surgery. The exclusion criteria consisted of any history of congenital anomalies, previous trauma or surgery to the operated area, and any other type of neuropathy. All patients had regular follow-ups for their HNPP at the Neuromuscular Diseases Unit. For this retrospective study, they were given a clear explanation of the aims of the study and gave informed consent before inclusion. Refusal or inability to give written consent and age under 18 years at the time of surgery were also exclusion criteria.
Surgical technique
Data on surgical techniques and clinical outcomes were available from medical records and operative reports. All procedures were standardized and performed by specialist hand surgeons, levels 3 and 4 (Tang and Giddins, 2016), in a nationally accredited hand surgery unit. Patients underwent surgery after failure of conservative management, including splinting for at least 6 months. The delay could be shortened in the case of severe clinical and electromyographic findings (motor deficit, clear axonal degeneration on EMG). No patient received corticosteroid injections. All surgeries were performed in the operating room under regional or general anaesthesia with a tourniquet set at 220–250 mmHg. The mini-open technique was used for each CTR (Gannon et al., 2011). A standard direct approach (Merle et al., 2017) was used for CUTR, and transposition was performed if ulnar nerve instability was identified intraoperatively (Matzon et al., 2016). Temporary analgesic sling immobilization was allowed with immediate finger mobilization.
Clinical assessment
Participants were assessed in person by a single independent assessor during their usual follow-up between September 2021 and February 2022. The following preoperative data were collected from medical records: age; sex; weight; tobacco use; medical history (diabetes, renal disease and musculoskeletal disorders); pain medication for neuropathy; occupation; medical history; and diagnosis of HNPP. The Boston Carpal Tunnel Questionnaire (BCTQ) (Levine et al., 1993) and a visual analogue scale (VAS) score (0 to 10) are commonly used in our department to assess CTS. Both were used to assess preoperative severity and as the main outcome measure to determine whether surgery was successful. The BCTQ is a self-administered questionnaire with one section focusing on symptoms, the Symptom Severity Scale (SSS), and another section focusing on function, the Functional Status Scale (FSS). The total score for the SSS and FSS is the sum of the individual scores divided by the number of items, with each response rated from 1 to 5. The SSS had also been identified as the best perioperative follow-up tool in a study on the management of CTS, which included more than 10 patients with HNPP among 309 patients with other inherited neuropathies (Panosyan et al., 2018).
At the last follow-up, the BCTQ and the VAS were repeated. We also collected patients’ satisfaction using a 5-point Likert scale and the Quick-DASH score (Gummesson et al., 2006; Hudak et al., 1996). Patients’ case histories and medical records were reviewed for any worsening of HNPP since surgery (onset of new chronic neurological symptoms, such as other entrapment neuropathies, gait abnormalities and deterioration in overall function). Finally, all intra- and postoperative complications were recorded: haematoma; nerve injury; postoperative infection; or acute mononeuropathy (tourniquet-related compression). Failed operations and their risk factors were analysed. Thresholds for failed surgery were based on a general population study with the BCTQ (Jarvik et al., 2009) and defined as follows: improvement in SSS of less than 30% and improvement in FSS of less than 10%, both compared with the preoperative score. Any ‘indifferent’, ‘mostly dissatisfied’ or ‘very dissatisfied’ patient was also counted as a failed surgery. Factors analysed for possible influence on surgical outcome were those commonly associated with peripheral neuropathies (tobacco, diabetes and renal disease), manual work (any work involving lifting, gripping, repetitive motion or exposure to vibration/percussion), preoperative neuropathic pain except entrapment neuropathies, preoperative signs of chronic polyneuropathy, surgery before the diagnosis of HNPP and type of anaesthesia.
For CUTS, a clinical assessment was made using the VAS of discomfort and the Patient Rated Ulnar Nerve Evaluation Questionnaire (PRUNE). This is a specific score, similar in design to the BCTQ, with two subscores: symptoms and function. Each subscore is calculated by summing the responses to 10 items rated 0 to 10 (0 to 100 points for each subscore) (MacDermid and Grewal, 2013). Due to its recent development, preoperative PRUNE scores were only available for a limited number of patients. Therefore, a relevant assessment of CUTR efficacy using this score was not possible. At revision, any ‘indifferent’, ‘mostly dissatisfied’ or ‘very dissatisfied’ patient was counted as a failed procedure.
Statistical analysis
Categorical variables are expressed as numbers (percentages). Quantitative variables are expressed as mean (standard deviation [SD]) or median (interquartile range [IQR]) for non-normal distributions. Normality of distributions was assessed using histograms and the Shapiro–Wilk test. Surgical outcome is assessed by the change in BCTQ and VAS from pre- to postoperative. This change is assessed by an analysis of variance for a repeated measures model using the mixed linear model to account for the patient effect and to adjust for follow-up time. The search for prognostic factors for failure was performed using generalized linear mixed models to adjust for the patient effect. The normality of the residuals of the models was checked. Statistical tests were performed at the two-tailed α level of 0.05.
Results
Study population
In total, 114 patients with HNPP were followed at our hospital centre between 1998 and 2020. Among them, 18 patients had 26 CTRs (bilateral in six patients) and were reviewed at a median of 8.5 years (IQR 4–13). None of the patients met our exclusion criteria. Most patients were referred to our hand surgery unit from the neuromuscular referral centre for resistant and disabling CTS/CUTS with a confirmed diagnosis of HNPP. Three patients were diagnosed through family screening of a known patient with HNPP and eight after they developed typical manifestations, such as acute sensorimotor palsies. However, CTS was the initial symptom leading to the diagnosis of HNPP in seven patients, three of whom had been referred for severe CTS with a highly suspicious EMG presentation but had not yet been diagnosed with HNPP. In these three patients, the CTR occurred before the genetic diagnosis of HNPP. Of the 26 CTRs, 20 were performed under local anaesthesia.
A total of 23 CUTRs in 15 patients were also included: 12 patients were already included for at least one CTR procedure, while three others underwent at least one CUTR exclusively. The mean follow-up was 11.4 years (SD 7.2).
Demographic and preoperative clinical data are shown in Table 1. The distribution of CTR and CUTR in the participants is described in Table 2.
Preoperative data: CTR and CUTR patients.
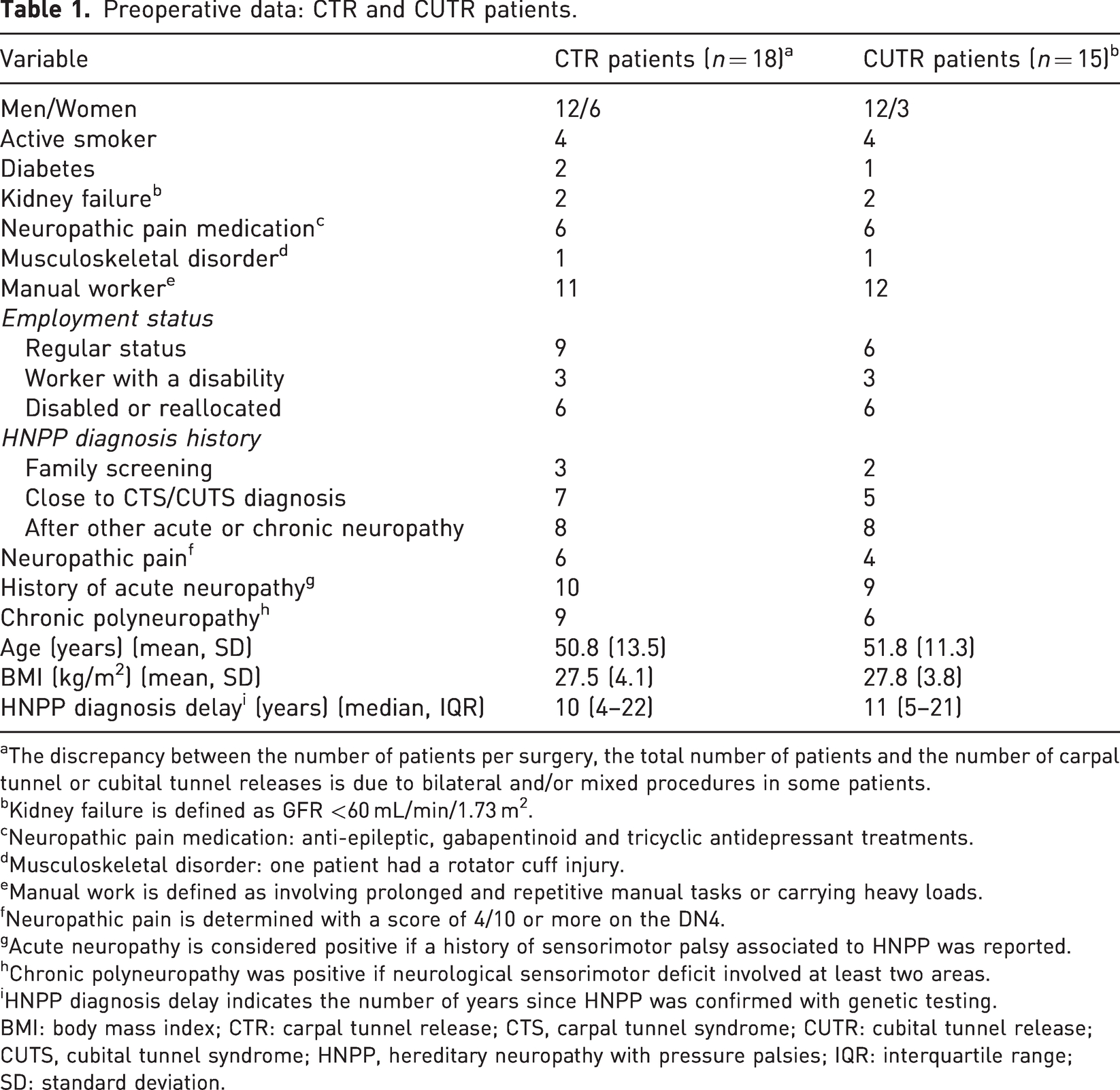
The discrepancy between the number of patients per surgery, the total number of patients and the number of carpal tunnel or cubital tunnel releases is due to bilateral and/or mixed procedures in some patients.
Kidney failure is defined as GFR <60 mL/min/1.73 m2.
Neuropathic pain medication: anti-epileptic, gabapentinoid and tricyclic antidepressant treatments.
Musculoskeletal disorder: one patient had a rotator cuff injury.
Manual work is defined as involving prolonged and repetitive manual tasks or carrying heavy loads.
Neuropathic pain is determined with a score of 4/10 or more on the DN4.
Acute neuropathy is considered positive if a history of sensorimotor palsy associated to HNPP was reported.
Chronic polyneuropathy was positive if neurological sensorimotor deficit involved at least two areas.
HNPP diagnosis delay indicates the number of years since HNPP was confirmed with genetic testing.
BMI: body mass index; CTR: carpal tunnel release; CTS, carpal tunnel syndrome; CUTR: cubital tunnel release; CUTS, cubital tunnel syndrome; HNPP, hereditary neuropathy with pressure palsies; IQR: interquartile range; SD: standard deviation.
Time distribution of the 49 surgical procedures in 21 patients.
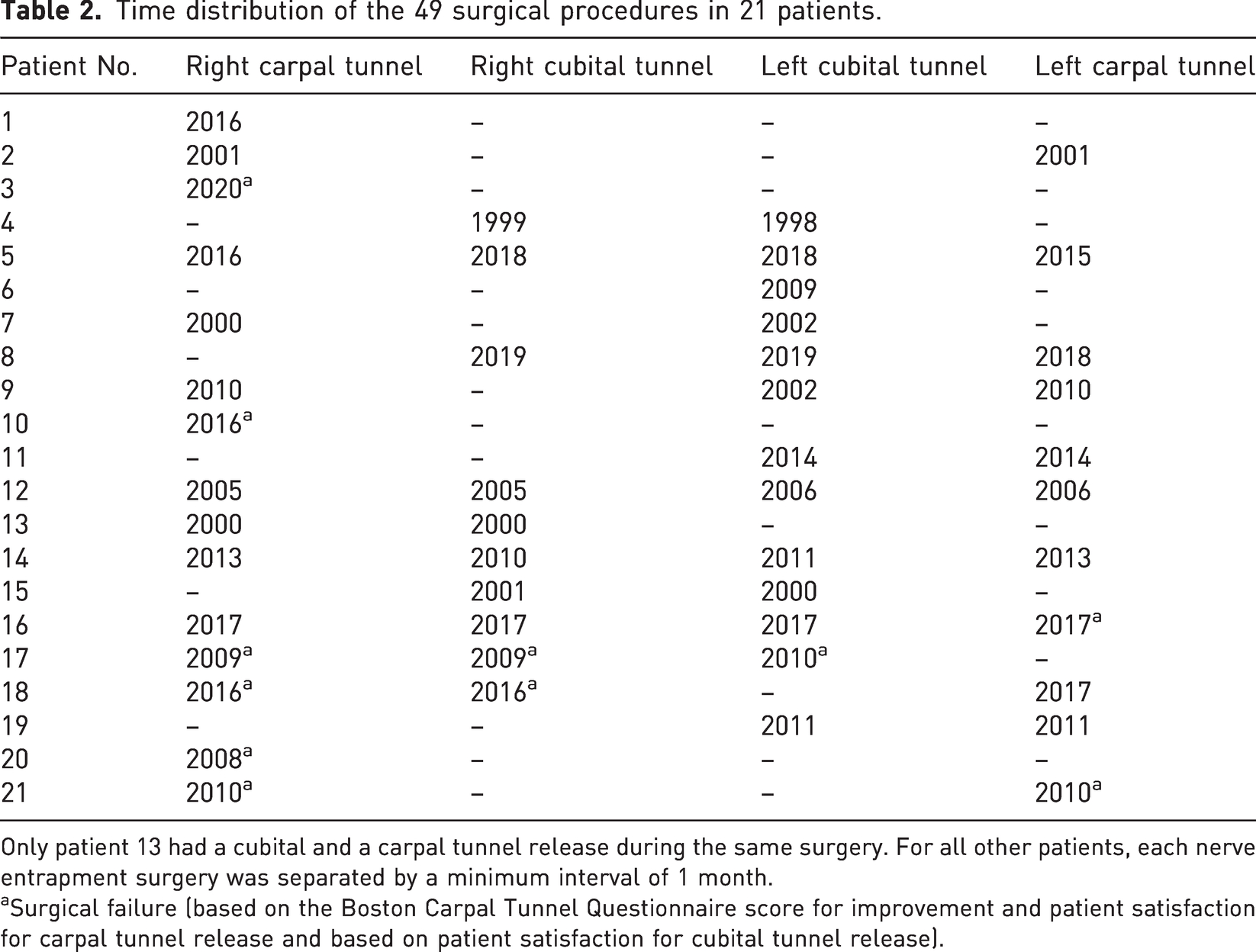
Only patient 13 had a cubital and a carpal tunnel release during the same surgery. For all other patients, each nerve entrapment surgery was separated by a minimum interval of 1 month.
Surgical failure (based on the Boston Carpal Tunnel Questionnaire score for improvement and patient satisfaction for carpal tunnel release and based on patient satisfaction for cubital tunnel release).
Outcomes
There was a significant improvement in the SSS subscore of the BCTQ questionnaire after CTR (1.3 points lower; p < 0.001); however, this was not statistically significant for the FSS (p = 0.14). There was a significant improvement in the patient discomfort VAS after CTR, with a mean decrease of 2.2 points (p < 0.001) (Table 3). Patients reported being satisfied or very satisfied with the results in 19 of 26 CTRs (Table 4). At the last follow-up in the CTR group, HNPP had worsened since surgery in 10 of 26 patients. The mean Quick-DASH score was 29 (SD 19.4). Eight CTRs were classified as failures according to our criteria (Table 2). None of the risk factors examined were significantly associated with CTR failure (Table 5).
Assessment of 26 carpal tunnel release outcome measures.
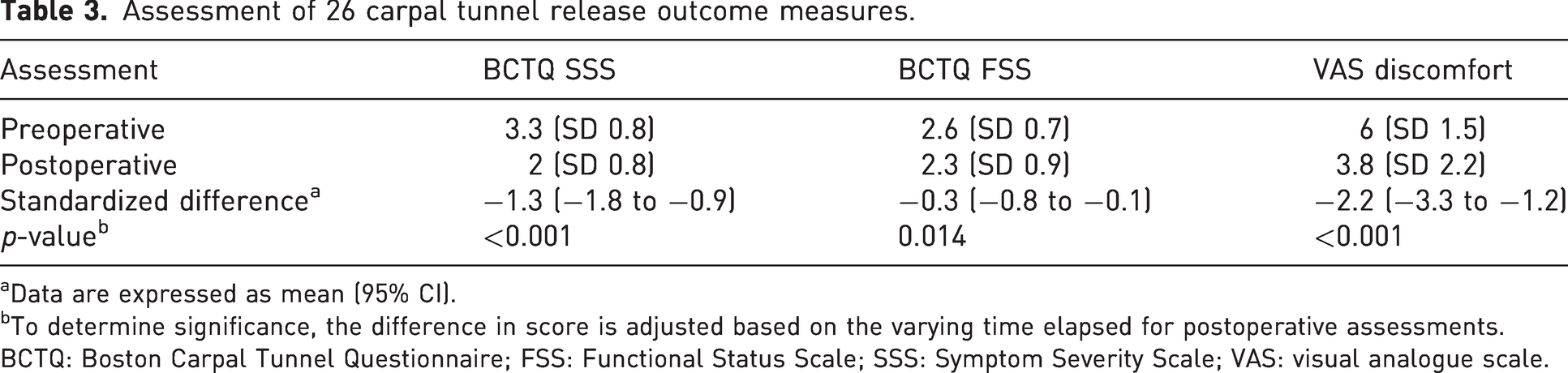
Data are expressed as mean (95% CI).
To determine significance, the difference in score is adjusted based on the varying time elapsed for postoperative assessments.
BCTQ: Boston Carpal Tunnel Questionnaire; FSS: Functional Status Scale; SSS: Symptom Severity Scale; VAS: visual analogue scale.
Satisfaction with surgical outcomes at postoperative assessment.
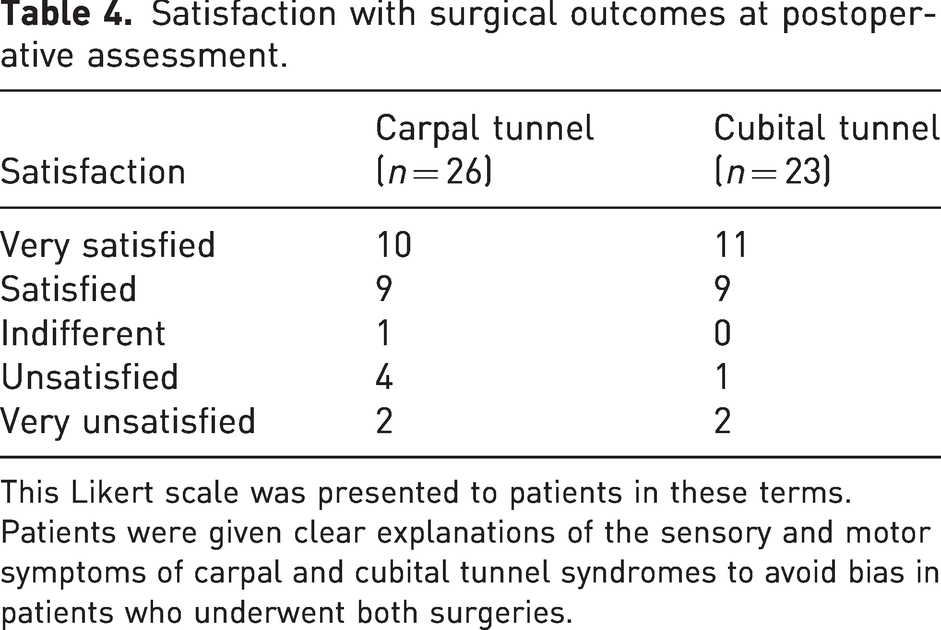
This Likert scale was presented to patients in these terms. Patients were given clear explanations of the sensory and motor symptoms of carpal and cubital tunnel syndromes to avoid bias in patients who underwent both surgeries.
Risk factors of carpal tunnel release failure.
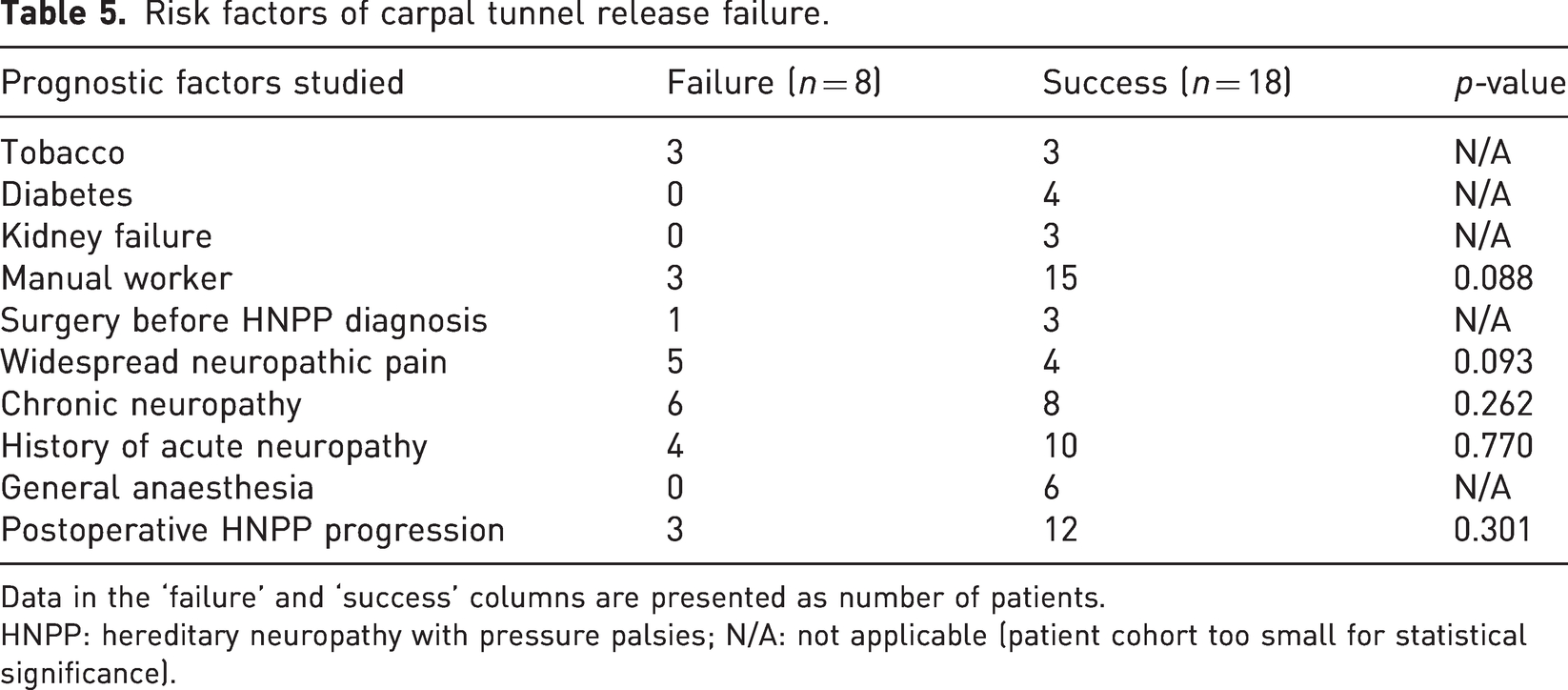
Data in the ‘failure’ and ‘success’ columns are presented as number of patients.
HNPP: hereditary neuropathy with pressure palsies; N/A: not applicable (patient cohort too small for statistical significance).
The preoperative PRUNE score was available for eight CUTRs in five patients, whose results are shown in Table 6. At the last follow-up, 20 of 23 patients were satisfied or very satisfied with the CUTR (Table 4), the mean Quick-DASH was 30 (SD 21.5) and the mean discomfort VAS decreased significantly from preoperative 6.1 (SD 1.6) to 4.2 (SD 2.4) (p = 0.002). Three procedures were classified as failures (Table 2).
PRUNE questionnaire regarding perioperative evolution in CUTR.
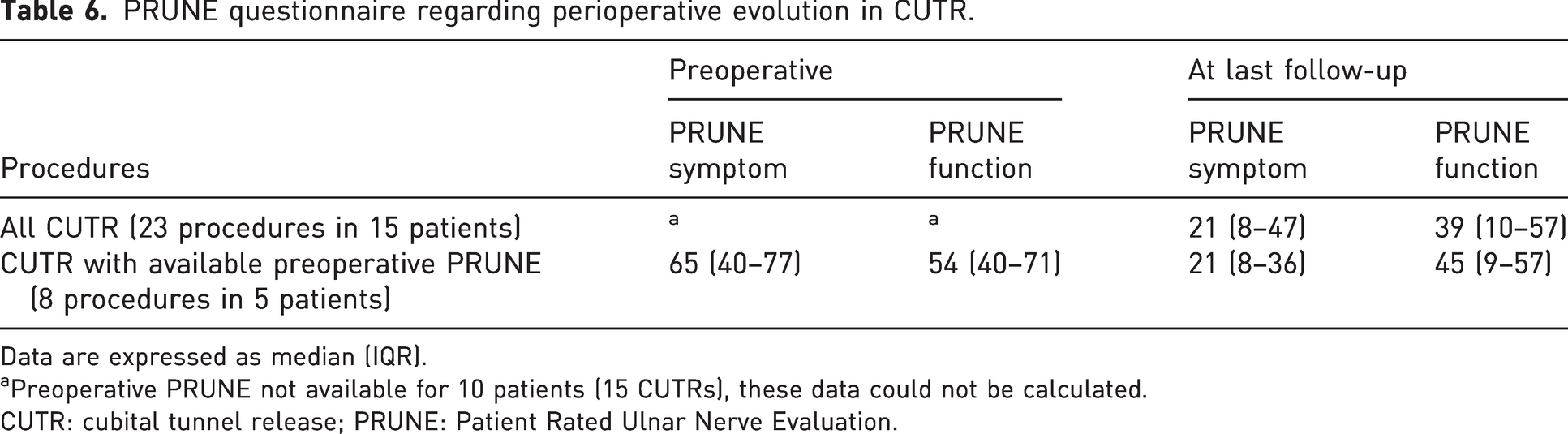
Data are expressed as median (IQR).
Preoperative PRUNE not available for 10 patients (15 CUTRs), these data could not be calculated.
CUTR: cubital tunnel release; PRUNE: Patient Rated Ulnar Nerve Evaluation.
There were no intra- or postoperative complications, including acute neuropathy for either CTR or CUTR.
Discussion
At a median follow-up of 8.5 years, CTR improved symptoms as assessed by a validated specific score in our study population with HNPP but did not significantly improve the function subscore. The satisfaction rate was 73%, and the VAS of discomfort decreased significantly by 2.2 points. Almost one-third of CTRs failed, but no prognostic factor was significantly associated with these failures.
Previous data on the surgical outcomes of CTR or CUTR release in patients with HNPP consist mainly of various case reports (Celik et al., 2008; Earle and Zochodne, 2013; Lazar et al., 2007; Magistris and Roth, 1985; Taggart and Allen, 2001). Only two studies analysing CTR outcomes included more than 10 patients with HNPP. The first, in a cohort of 309 patients with various inherited neuropathies (Panosyan et al., 2018), did not find a significant improvement in postoperative SSS scores in their small HNPP subgroup. The second and most recent study also reported clinical improvement after CTR in patients with HNPP (Chompoopong et al., 2022). The latter showed disappointing results of CUTS in a smaller population but with more reliable preoperative data and perioperative EMG.
We had no complications, despite the inherent risks of the anaesthetic modalities or the systematic use of a tourniquet. This contradicts the case reports that theorize that any surgery in HNPP carries a risk of poor outcome or neurological complications (Kramer et al., 2016; Logroscino et al., 2016; Ragois et al., 2013). The authors advised against nerve surgery or use of a tourniquet in HNPP. This discrepancy in outcomes may be explained by the short operative time of both procedures and the careful monitoring of the tourniquet, which is placed away from common entrapment sites. In addition, CUTR and CTR may be less risky than lower limb arthroplasty or trauma reported in some cases. Both procedures achieved good satisfaction rates, although one-third of CTRs were classified as failures. This discrepancy may also be due to our criteria for failed surgery. We used the most stringent criteria defined by Jarvik et al. (2009) in a general population study and applied them to a population with HNPP with more severe disabilities (preoperative SSS was 2.95 in Jarvik et al. vs. 3.3 in our study). In addition, HNPP progressed in several of our patients after surgery, which may have reduced the benefit of surgery at the long-term follow-up. However, we adjusted the statistical analysis of the scores based on the length of follow-up to ensure the validity of our main outcome measures.
Low statistical power probably explains why none of the factors studied reached significance for failure. Preoperative neuropathic pain seemed close to significance, and further analysis in a larger population might be interesting, especially as it has been noted that HNPP may only manifest as pain in some patients. Unexpectedly, non-manual occupation was close to significance for failure of surgical peripheral nerve release. This might indicate a specific benefit for manual workers, which cannot be explained by our data. We could not perform a relevant statistical analysis of CUTR results due to the lack of preoperative PRUNE scores. However, the VAS of discomfort was significantly reduced, and patients reported a satisfaction rate of 85% after this procedure, which is encouraging.
The limitations of our study include its retrospective nature and a long and variable postoperative delay between surgery and last follow-up. Despite statistical adjustment, readers should remain cautious about interpreting these results. The study sample was small in absolute numbers, but it is a large cohort of patients with HNPP with entrapment neuropathies considering that the condition is rare. Unfortunately, perioperative EMG was sometimes unavailable.
Perioperative EMGs should be performed systematically before CTR or CUTR in patients with HNPP. In line with published studies and because of the many asymptomatic EMG abnormalities in HNPP, we recommend that this surgery be restricted to a referral centre that allows collaboration between neuromuscular genetic disorder specialists and hand surgeons. Candidates for surgery are symptomatic patients who are not relieved by splints and who have previously been warned of potential disappointing results or progressive changes. Further studies are needed to confirm these findings and establish a clear indication for surgery. HNPP causes nerve enlargement where compression usually occurs, whether or not patients are symptomatic (Ginanneschi et al., 2012; Goedee et al., 2015; Hooper et al., 2011). In one CTR case report, the authors found a decrease in nerve size after surgery in a patient with a particularly thick nerve (Kim and Kim, 2020), raising the possibility of using ultrasound to determine prognostic thresholds.
Footnotes
Acknowledgements
The authors thank Dr. Céline Tard, CHU Lille, Clinique de Neurologie, Centre de Référence des Maladies Neuromusculaires de Lille Hôpital Roger Salengro, Lille, France. The authors are also grateful to Joanne Archambault, PhD for English language assistance.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was given by our facility’s local Ethics Committee based on the retrospective nature of the study, as all the procedures being performed were part of the routine care and follow-up of patients.
Informed consent
Oral and written informed consent was obtained from all individual participants included in the study.