
Abstract
We reviewed the incidence and management of complications after total wrist arthroplasty, as reported in the literature, with so-called fourth-generation implants and other recent designs. While early intraoperative and postoperative complications, including fractures, tendon lacerations, infection, nerve compression, tendonitis, stiffness and chronic regional pain syndrome, had an acceptable incidence, late complications, such as periprosthetic osteolysis and implant loosening, occurred more frequently. Implant survival at 10 years was in the range of 70%–80% in most publications. Several of the implants have been modified or withdrawn. Instability and dislocation were frequent after a pyrocarbon spacer. Failed arthroplasties can be salvaged by revision arthroplasty or total wrist arthrodesis. Revision arthroplasty has a lower survival rate than primary arthroplasty and does not clearly offer important significant advantages over total wrist arthrodesis in terms of patient-reported outcome measures. Further development of prosthetic design, new materials and more knowledge on patient-related risk factors are needed.
Introduction
Generational evolution
Total wrist arthroplasty (TWA) is an alternative to total wrist arthrodesis for the treatment of painful destroyed wrists. The first-generation implants, the hinged silicone spacers, gave promising early results in low-demand patients with rheumatoid arthritis (RA) but the long-term results were discouraging due to a high incidence of failure, mainly breakage of the implant (Brase and Millender, 1986). The next generations of TWA consisted of bulky multicomponent implants, requiring substantial bony resection. Long-term implant survival was unreliable and revision surgery to an arthrodesis was challenging due to the loss of bone stock (Cooney et al., 1984; Vogelin and Nagy, 2003). Subsequent changes in the designs of TWA led to the development of implants such as the Biax (DePuy Orthopedics, Warsaw, IN, USA), which required less bone resection but still extended fixation of the distal component into the middle finger metacarpal. Implant survival improved compared to the previous generation of implants, but implant loosening still remained a problem, especially the carpal component (Cobb and Beckenbaugh, 1996). This implant was withdrawn from the market for commercial reasons. In the late 1990s, the fourth generation of implants was introduced, requiring minimal bone resection, minimal fixation in the metacarpals and a more anatomic design (Menon, 1998). These fourth-generation implants included five metal-on-polyethylene prostheses: the Universal 1 (KMI, San Diego, CA, USA); the Universal 2 (Integra, Plainsboro, NJ, USA); the Freedom (Integra, Plainsboro, NJ, USA); the Remotion (Stryker, Kalamazoo, MI, USA); and the Maestro (Biomet, Warsaw, IN, USA). The initial Universal 1 design gave hopes to yield better results and fewer complications, especially with lower incidence of loosening of the carpal component, but carried a higher risk of dislocations and was later modified into the Universal 2. The Maestro has since been withdrawn from the market for commercial reasons and the Universal 2 further developed into the Freedom implant. Of these, only the Freedom and the Remotion are still available for use today.
For the purposes of this review, we have included the results of implants that have been withdrawn, since they teach us lessons on the problems that we currently deal with today, not least the long-term complications and how to address them. In addition, we also report on two more recent implants: the Motec (Swemac Orthopaedics AB, Linköping, Sweden) and the Amandys (Tornier SAS-Bioprofile, Grenoble, France). The Motec is a metal-on-metal prosthesis with a large screw fixation in the radius as well as in the middle finger metacarpal and a ball-and-socket articulation. The Amandys is a one-component radiocarpal interpositional pyrocarbon spacer without fixation to the bones.
TWA implant survival
Implant survival after any joint replacement is crucial. In comparison with total wrist arthrodesis, the benefit of keeping the wrist mobile using a TWA must be balanced against the risk of major revision surgery in case of prosthetic failure. Life expectancy is rising and thus long-term survivorship is increasingly relevant. For 60-year-old patients needing joint replacements, this ideally requires implants that survive for at least 25 years.
Survival of newer TWA implants is approximately 70%–80% at 10 years, with few reported exceptions (Table 1). This needs to be viewed in the context of survival rates of other major joint arthroplasties. According to the systematic review by Evans et al. (2019a), the 25-year pooled survival of hip replacements from case series is 78% and from joint replacement registries 58%. The 25-year survivorship of total knee replacement from registries is 82% (Evans et al., 2019b). The reported 10-year survival rate for shoulder arthroplasty is 92% (Evans et al., 2020), for linked total elbow replacement 92% (Evans et al., 2022) and for ankle replacement 66% (Perry et al., 2022). In comparison, the highest reported survival rate for fourth-generation TWA at 15-year follow-up is 78% (Gil et al., 2017). Twenty-five-year survival estimates are still not available for TWA for us to determine its long-term success.
Implant survival in series with long observation periods.
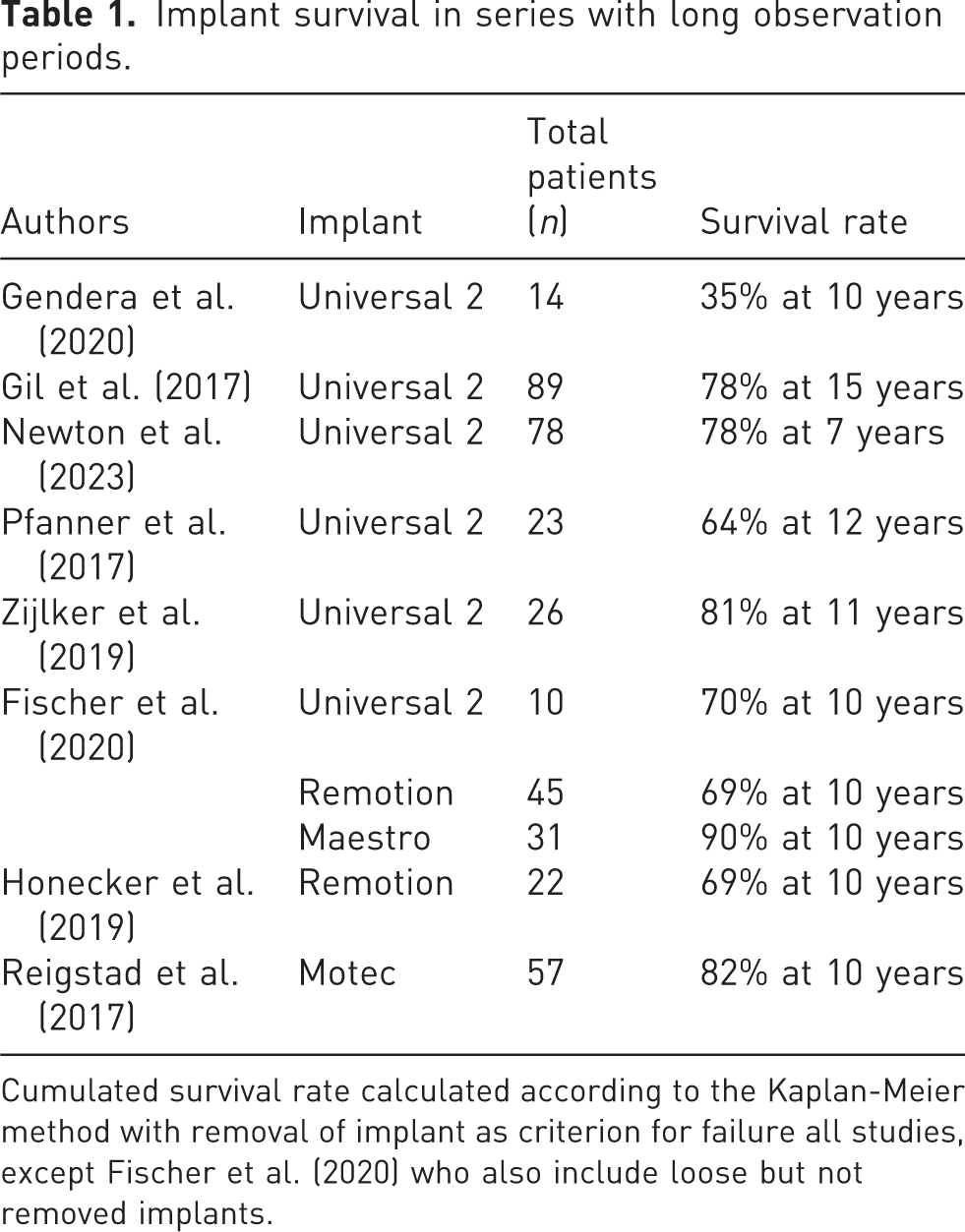
Cumulated survival rate calculated according to the Kaplan-Meier method with removal of implant as criterion for failure all studies, except Fischer et al. (2020) who also include loose but not removed implants.
The aim of this article was to report on the incidence and management of complications encountered with the latest TWA implants. A summary of the complications and their incidence is given in Table 2.
Reported incidence of complications after total wrist arthroplasty with recent prosthetic designs.
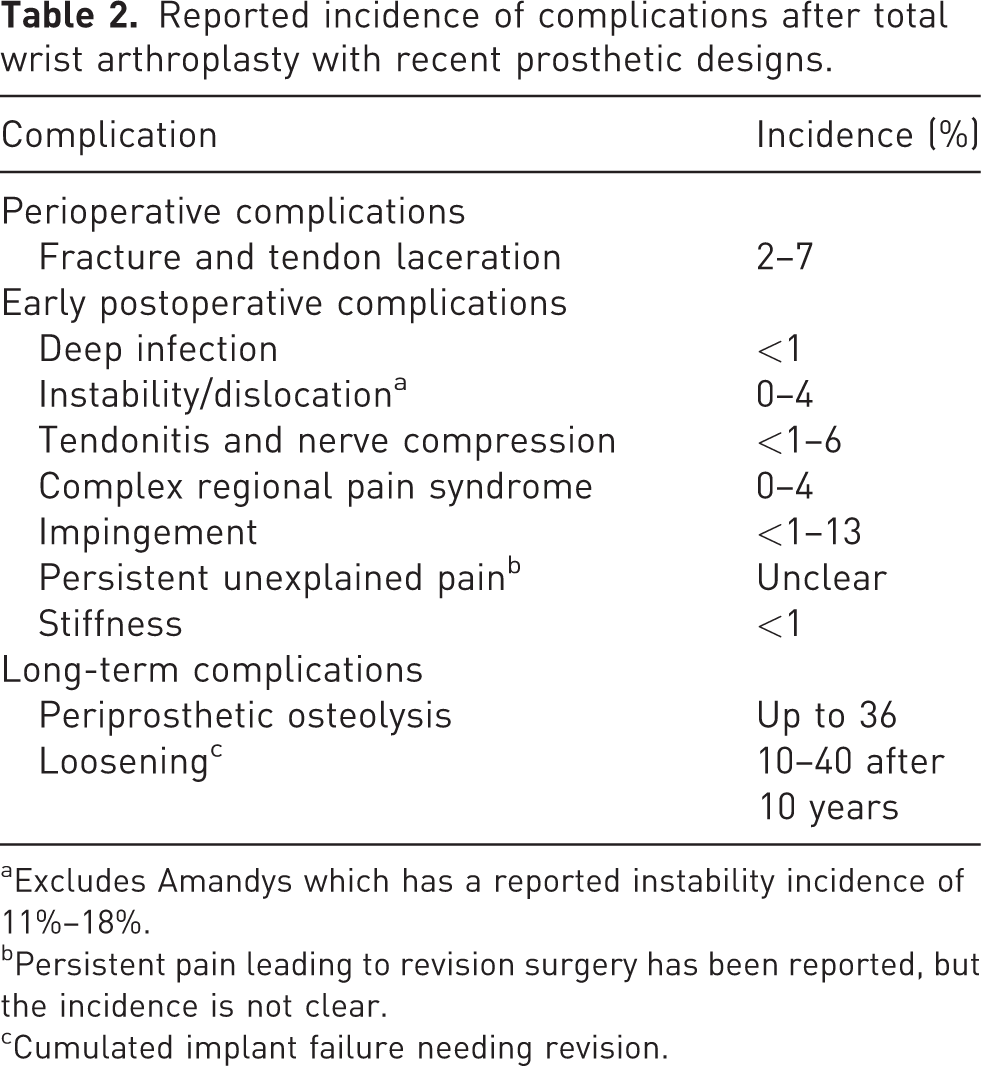
Excludes Amandys which has a reported instability incidence of 11%–18%.
Persistent pain leading to revision surgery has been reported, but the incidence is not clear.
Cumulated implant failure needing revision.
Specific complications and their management
Perioperative complications
Fractures and tendon injuries
The most common complications faced by the operating surgeon during a TWA include fractures and tendon injuries. Boeckstyns et al. (2013), reporting on a series of 65 wrist replacements using the Remotion implants, noted three fractures and two tendon lacerations. Wagner et al. (2017) analysed 445 cases of older and recent TWA designs, and found that perioperative fractures of the radius, metacarpals or capitate occurred in 2% of patients. The age of the patient was noted as a risk factor. However, implant survival does not seem to be affected. In a systematic review, Berber et al. (2018) found the incidence of fractures to be 0.2% and tendon problems 0.5% in 651 fourth-generation implants.
The principles of management of perioperative TWA fractures remain largely in line with treating intraoperative fractures during any joint replacement. These are usually amenable to be treated conservatively in a cast, with or without the addition of cerclage wiring. Any intraoperative tendon injuries identified during the procedure need immediate repair and protection, following the principles of any tendon repair.
Early postoperative complications
Prosthetic joint infection (PJI)
PJI is a rare event after TWA in the current day and age. Berber et al. (2018) calculated that its incidence was 0.1% in the latest generation. Herzberg et al. (2012) showed one case in 215 Remotion TWAs. Maintaining a high degree of suspicion and aggressive treatment may help to salvage the joint in the case of PJI in the early postoperative period. Pain, erythema, oedema, prolonged postoperative wound effusion or wound dehiscence during the early post operative period should lead to the suspicion of PJI. Serial blood tests looking for elevated C-reactive protein and white blood cell count should be undertaken to support the diagnosis. Multiple samples taken from the joint for microbiological investigation will help to confirm the diagnosis and the organism. However, conventional culture techniques have limitations in terms of identifying microorganisms in PJI. False-negative cultures are in the range of 5%–42%, as seen in a recent systematic review, due to sampling issues, prior antibiotics, insufficient culture time, chronic infections and probably other unknown causes (Kalbian et al., 2020). Molecular biology techniques, such as polymerase chain reaction (PCR)-based techniques, to detect traces of microorganism nucleic acids in periprosthetic biofilm are faster, more reliable and accurate for detection of PJI than traditional cultures (Qu et al., 2013), but require specialized laboratory facilities.
The principles of management of any PJI should be applied to TWA as well. Surgical resection of all infected tissue combined with exchange of polyethyelene spacer is required as soon as possible after diagnosis is confirmed. Patients should be started on broad-spectrum antimicrobial treatment as soon as appropriate joint samples are taken, followed by targeted therapy once the causative agent is identified. Implant retention could be considered in very early postoperative PJIs. However, depending on the extent of the infection and debridement, removal of the implant and cement, if this was used, may be required.
An antibiotic spacer can be inserted as the first stage if a second stage revision replacement is being considered. Revision TWA or conversion to a total wrist arthrodesis is performed when there is no longer evidence of active infection. Antibiotic treatment should be continued for at least a further 6 weeks in those situations.
Instability
Instability was a problem with the first design of the fourth-generation (Universal 1) implant. Menon (1998) reported a 14% dislocation and Ward et al. (2011) had four cases of recurrent prosthetic instability and one recurrent dislocation out of 24 Universal 1 TWAs. The problem was clearly related to the design of the prosthesis with the curvature of the articulation being too flat. After design modification, this problem became rare in the Universal 2 implant (Badge et al., 2016; Brinkhorst et al., 2018; Ferreres et al., 2011; Kennedy et al., 2018; Martinez Vilen and Rodriguez Nogue, 2021; Pfanner et al., 2017; Zijlker et al., 2022).
The most common reasons for instability are wrong perioperative tensioning of the construct (too much bone resection), poor ligamentous support (as in severe RA of Simmen type III), neurological disorders or trauma. In the multicentre series of 215 Remotion cases published by Herzberg et al. (2012), there was one dislocation in a patient with a neurological condition. Various authors have reported no dislocations in their series using Remotion implants (Bidwai et al., 2013; Fischer et al., 2020; Froschauer et al., 2019; Gupta, 2008; Holzbauer et al., 2022; Honecker et al., 2019). Gaspar et al. (2016) reported two cases of instability out of 47 Maestro prosthesis, while Nydick et al. (2012) noted one in their series of 23. Similar results have also been published using a Motec replacement, with Reigstad et al. (2017) reporting one dislocation out of 56 non-rheumatoid patients and Giwa et al. (2018) had one dislocation out of 25 patients.
Compared to the metal on polyethylene TWA implants, frequent instability and dislocation of the pyrocarbon interpositional wrist spacer (Amandys; Tornier SAS-Bioprofile Grenoble, France) has been reported. In a series of 28 reported by Lestienne et al. (2021), three had to be reoperated because of dislocation. A similar high dislocation rate has also been reported by other authors (Gvozdenovic and Vadstrup, 2022; Marie et al., 2021; Pierrart et al., 2012). Early postoperative dislocation after Amandys interposition is usually caused by improper implant placement, incorrect implant size or insufficient capsular reconstruction.
Early dislocation can usually be managed by closed reposition and immobilization for a few weeks. Recurrent instability, on the other hand, may require revision of the implant. The problem can sometimes be solved by exchanging the carpal polyethylene ball with a thicker one, if available, or with exchange of components and augmenting the radius or carpus with a structural bone graft. If this is not feasible or unsuccessful, conversion to a total wrist arthrodesis is the proper solution.
Tendonitis and nerve compression
Other complications of TWA include tendonitis and nerve compression in the carpal tunnel or Guyon’s canal. Wagner et al. (2017) counted three cases of tendonitis or nerve compression in 47 TWAs. Froschauer (2019) had one de Quervain’s tendinitis out of 39 TWA. Berber et al. (2018) found nerve-related problems in 0.2% of 651 latest-generation implants.
Nerve compressions are treated conventionally by nerve release. Tendonitis after TWA can also be addressed with peritendinous steroid infiltrations initially or tendon release if that fails.
Reflex sympathetic dystrophy/complex regional pain syndrome (CRPS)
In the systematic review by Berber et al. (2018), there were no cases of CRPS among the 651 TWAs. This is also reflected in more recent publications, where there is no mention of this complication (Gendera et al., 2020; Martinez Vilen and Rodriguez Nogue, 2021; Newton et al., 2023; Zijlker et al., 2019). However, in a multicentre study on Remotion implants, Herzberg et al. (2012) noted three patients with CRPS out of 129 rheumatoid patients and six patients out of 86 non-rheumatoid patients.
The principles of management of a patient with CRPS after TWA remains the same as with any causes of this condition with adequate pain management and aggressive physiotherapy, and an in-depth review of this is beyond the scope of this article.
Impingement
Impingement after TWA most frequently occurs on the radial side by collision between the radial component and the remaining scaphoid (Figure 1). The authors of the present article believe that impingement can be avoided by paying careful attention during the procedure, both visually and with using an image intensifier, and by resecting scaphoid bone as needed. It is probably asymptomatic and unrecognized in many cases. Berber et al. (2018) reported an impingement incidence of 0.1% in their series after TWA. Froschauer et al. (2019) reported on five cases of impingement between the scaphoid remnants and the radial prosthetic component in a series of 39 Remotion TWAs. They solved the problem by routinely excising the scaphoid completely. Impingement with the pisiform has also been reported (Johnson et al., 2007) and could be addressed by complete excision of the pisiform.
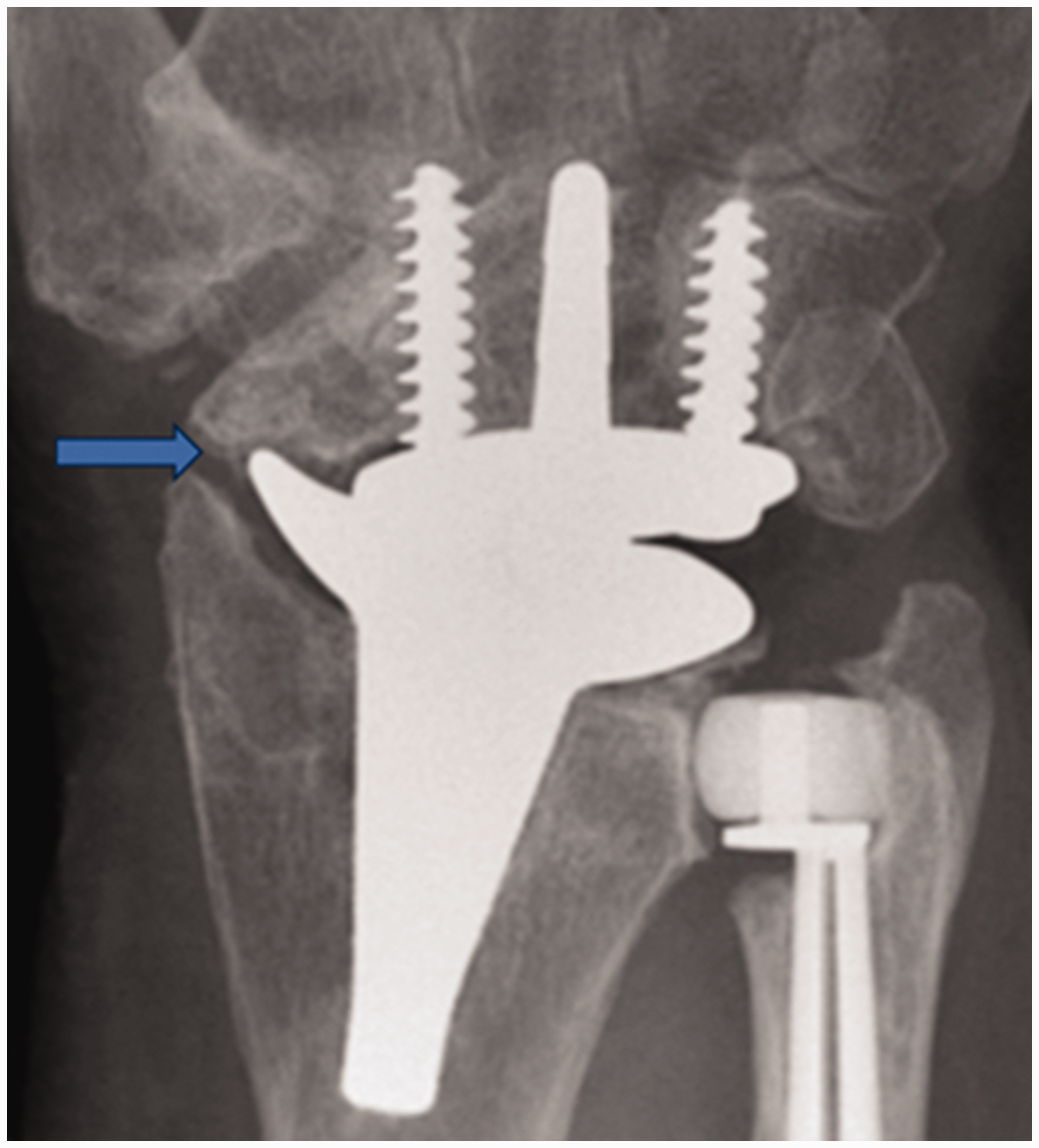
Impingement of the radial Remotion component and the distal scaphoid (arrow) caused by a slight varus malposition of the radial component and ulnar translation of the carpus. The problem could be solved by resection of excessive scaphoid bone.
Persistent pain
Generally, TWA with latest-generation implants results in significant pain relief (Badge et al., 2016; Boeckstyns et al., 2013; Cooney et al., 2012; Gil et al., 2017; Morapudi et al., 2012; Nydick et al., 2012; Reigstad et al., 2017; Sagerfors et al., 2015; Zijlker et al., 2022). However, persistent pain without an obvious underlying cause is well-known after any joint replacement. A study by Wylde et al. (2011) showed that the presence of major mental depression was a significant and independent postoperative determinant of persistent pain after total hip and total knee replacement. It is not clear whether persistent pain after a total joint replacement leads to mental depression or whether pre-existing depression contributes to the persistent pain. The presence of pain elsewhere in the body was also an independent determinant. It is possible that some patients develop persistent postoperative pain because of an underlying vulnerability to pain by pain sensitization. The problem has been casually reported in TWA patients (Adams et al., 2016; Berber et al., 2020) but has not been systematically investigated.
A patient with unclear persistent pain after a TWA needs to be examined thoroughly for any underlying condition that might be the cause of the pain. This includes neuropathic conditions, tendonitis, impingement, prosthetic loosening, complex regional pain syndrome, instability and so on. If no clear cause can be identified, temporary blockage of the anterior and posterior interosseous nerves can be performed in view of considering potential neurectomy (if this has not been done during previous operations). Ultimately, if the pain is severe, conversion to a total wrist arthrodesis may be indicated. If an underlying psychological association is suspected, one must be very careful in considering further surgery.
Stiffness of wrist
It is a common finding that wrist mobility will remain more or less unchanged after TWA (Boeckstyns et al., 2013). Poor preoperative mobility of the wrist cannot be expected to improve postoperatively, and patients should be counselled preoperatively regarding this to avoid high expectations. A spontaneously fused wrist in a rheumatic patient is likely to stiffen again after a TWA (Figure 2). According to the systematic review by Berber et al. (2018), stiffness is a very rare problem (1 in 651 cases). If the patient has a painful wrist with poor mobility after TWA, conversion to a total wrist arthrodesis may be the best solution.
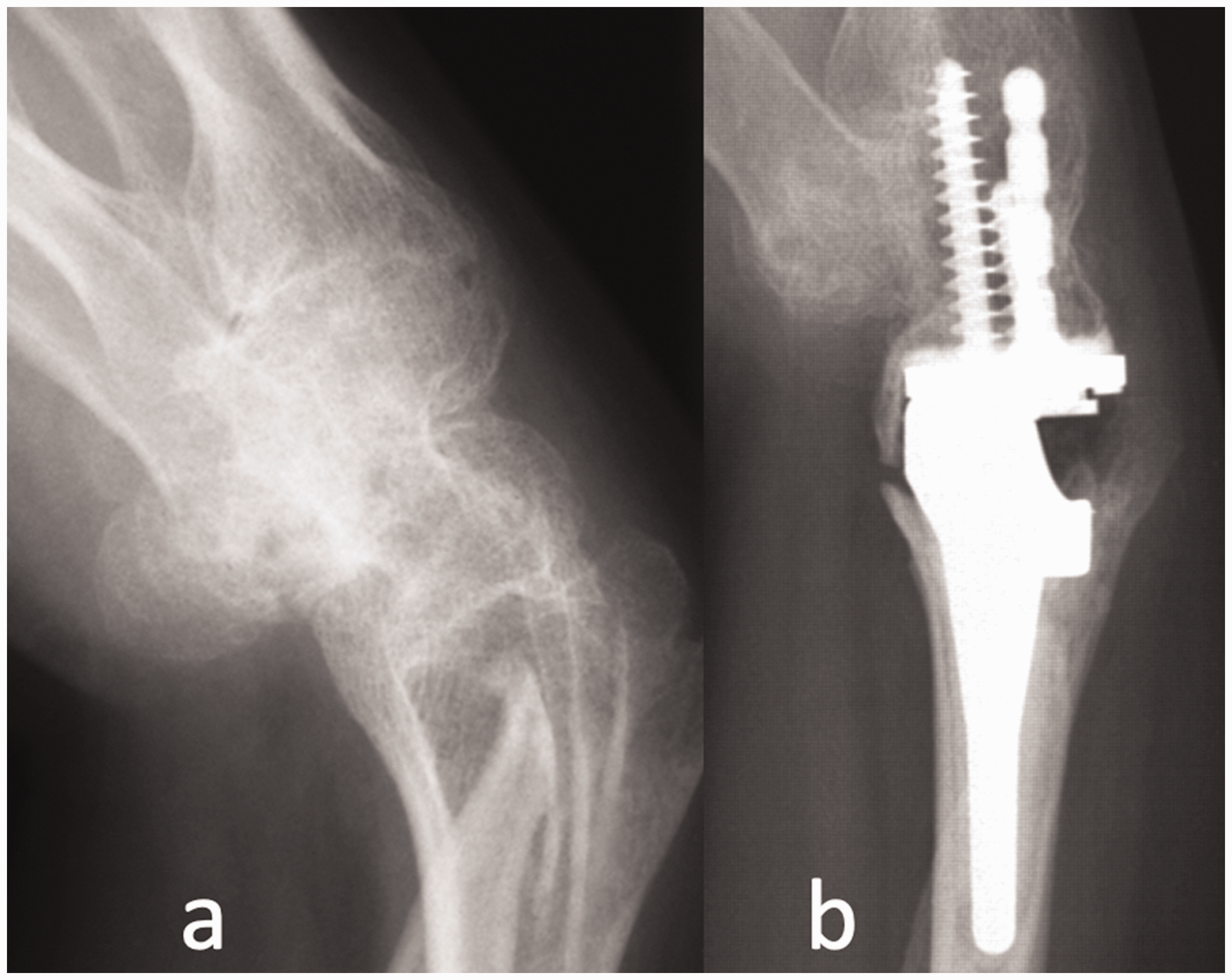
(a) Spontaneous wrist fusion with flexed deformity in a patient with rheumatoid arthritis and (b) Some mobility was restored initially after total wrist replacement, but periarticular calcification resulted in recurrence of wrist stiffness.
Late complications
Periprosthetic osteolysis
Periprosthetic osteolysis (PPO) is a well-described phenomenon after total joint replacement and is one of the most prominent reasons for revision surgeries (Gallo et al., 2008). PPO was systematically investigated for TWA in 1996 after a Biax replacement (Cobb and Beckenbaugh, 1996). Its occurrence, causes and consequences are increasingly reported and discussed. Boeckstyns and Herzberg (2014) analysed 44 consecutive patients with Remotion TWA with a mean follow-up of 3.7 years (minimum 2 years). There were 21 wrists with RA and 23 wrists without RA. Periprosthetic radiolucency of more than 2 mm in width at the radial component side was seen on plain radiographs in 16 patients and at the carpal component side in seven patients. The radiolucency developed gradually regardless of the primary diagnosis (RA or non-RA) and was located at the extremity of the components near the joint. It seemed to stabilize in most patients after a period of 1–3 years postoperatively. They found that the radiolucency was not related to obvious loosening of the implant components. Only five carpal components and one radial component subsided or tilted on follow-up. More recently, PPO has been reported with other implants, including the Universal 2 and Freedom (Martinez Villen et al., 2022), the Motec (Holm-Glad et al., 2022; Karjalainen et al., 2018) and the Maestro (Sagerfors et al., 2015), but not with the Amandys pyrocarbon spacer. Some degree of osteolysis was seen radiographically in as many as 20 out of 25 TWAs in a review of the Universal 2 and Freedom prostheses, but only five had to be reoperated; of these five, only three were found to be loose on the carpal side and none on the radial side (Martinez Villen et al., 2022). This is consistent with the findings of Boeckstyns et al. (2014) and with the findings after prosthetic replacements of other joints, especially total ankle replacements (Koivu et al., 2009).
A commonly proposed theory is that PPO is induced by wear particles and corrosion products that stimulate inflammatory biological response on the surrounding tissues (Gallo et al., 2008). The activation of macrophages by these wear particles lead to bone resorption and osteolysis, resulting in prosthesis failure. The proponents of this ‘particle disease’ claim that the ultrahigh molecular weight polyethylene is mainly responsible for the development of the lesions (Saadi et al., 2021). However, an investigation by Boeckstyns et al. (2014) on a consecutive series of Remotion TWA found no correlation between the number of polyethylene particles in biopsies of the implant-bone interphase and the magnitude of the osteolytic lesions. Moreover, there is evidence that PPO also occurs with metal-on-metal implants (Holm-Glad et al., 2022; Karjalainen et al., 2018). In a series of 130 consecutive ankle replacements, Koivu et al. (2009) found osteolytic lesions in 37% and the risk for osteolysis was three times higher with implants with titanium-hydroxyapatite porous coating; the authors suggest that titanium particles may be implicated. The findings of Martinez Villen and Rodriguez Nogue (2021) in a study of 25 TWAs, which included Universal 2 and Freedom implants, also point in that direction. Titanium was the main elevated serum metal ion in that study, with only infrequent elevated serum cobalt or chromium values seen. The risk of loosening was found to be higher with serum titanium values in the range of 26–31 mg/L.
Stress shielding may also play a role in the development of PPO, as indicated in a biomechanical study (Completo et al., 2017). In that study, finite element models were developed to assess the structural behaviour of cancellous–bone and bone–cement interfaces and these models were validated against experimentally measured cortex strains. There was a significant strain reduction in the measured cortex strains in radii with the Maestro prosthesis compared to intact radii, with a potential risk of bone atrophy around the distal region of the radius for loads in the range of daily wrist activities.
Narrow areas of radiolucency confined to the articulating surfaces of the implant components should not cause any concern. When faced with larger lesions, a treatment decision must be made. Observation, curettage and grafting, implant revision and arthrodesis are the broad options available in those situations. A broader but still limited radiolucency may look dramatic on radiographs and tempt the surgeon to revise and bone graft the osteolytic area, even if there is no pain. However, this strategy may have a high probability of failure. The procedure (using bone graft, bone cement or a mixture of these) has been well-described for total ankle replacement. Yoon et al. (2014) had very little recurrence in their 10 cases. However, most total wrist replacement series report rather high recurrence rates after the grafting of osteolytic lesions (Besse et al., 2013; Gross et al., 2016; Kohonen et al., 2017). The authors of the present article have some experience with bone grafting in the wrist (Figure 3). At present, we recommend close and continued observation of painless osteolysis until such time that the patient notices pain or there is evidence of implant loosening on radiographs. Painful osteolysis or loosened implant components require a revision of implants or arthrodesis.
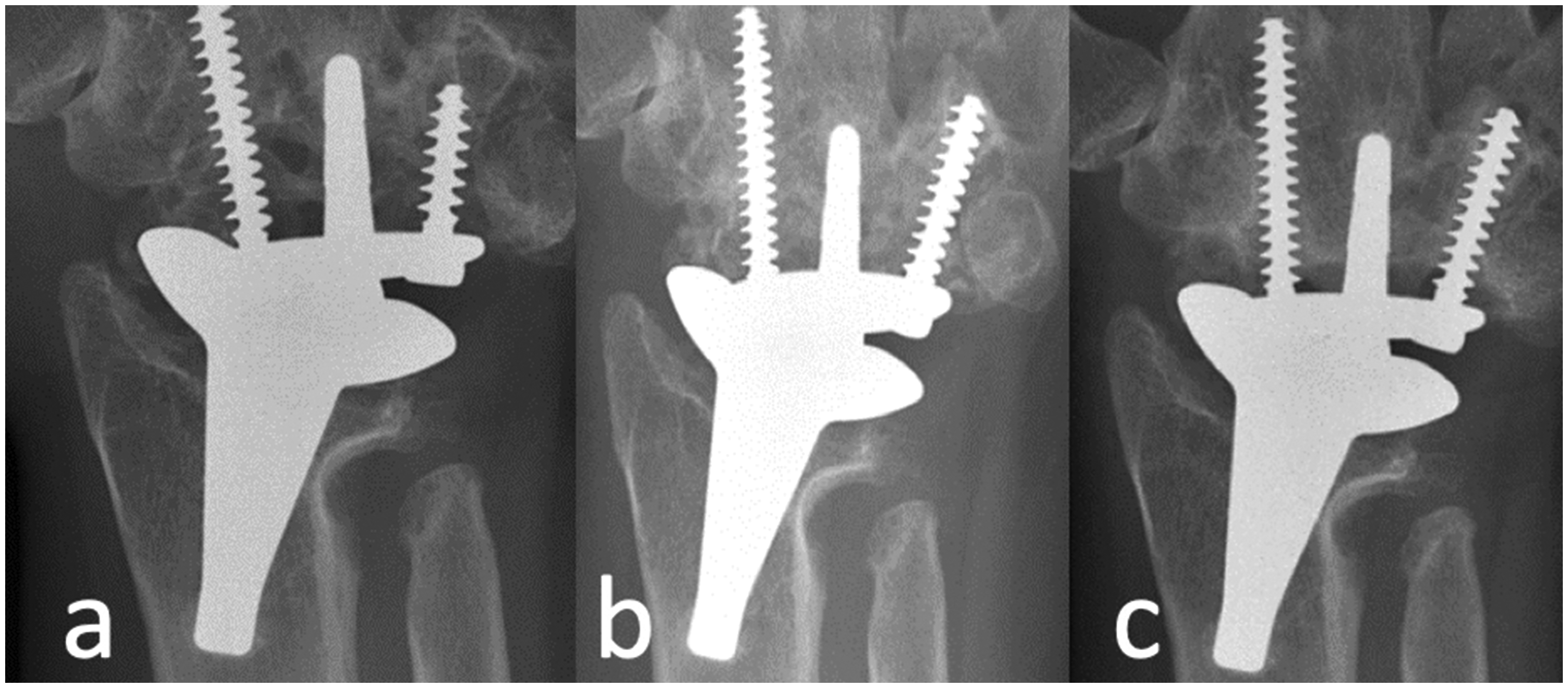
(a) Radiograph showing periprosthetic osteolysis. (b) Radiograph after curettage of the osteolytic area under the carpal plate and autologous iliac crest bone grafting and (c) Recurrence of osteolysis.
Prosthetic loosening
PPO may or may not lead to prosthetic loosening (Boeckstyns and Herzberg, 2014; Martinez Villen and Rodriguez Nogue, 2021). Loosening of the carpal component is more frequent than that on the radial side with the type of carpal fixation in the latest generation of implants as seen in the Universal and Remotion prostheses. The possible explanation of this is, although there is marked osteolysis around the radial implant, it remains confined and hence the radial component would still remain well fixed due to its relatively large stem. Conversely, the carpal component is held in place by a short peg only with the screws not being locked in the carpal plate, and thus more at risk of getting loose (Figure 4).
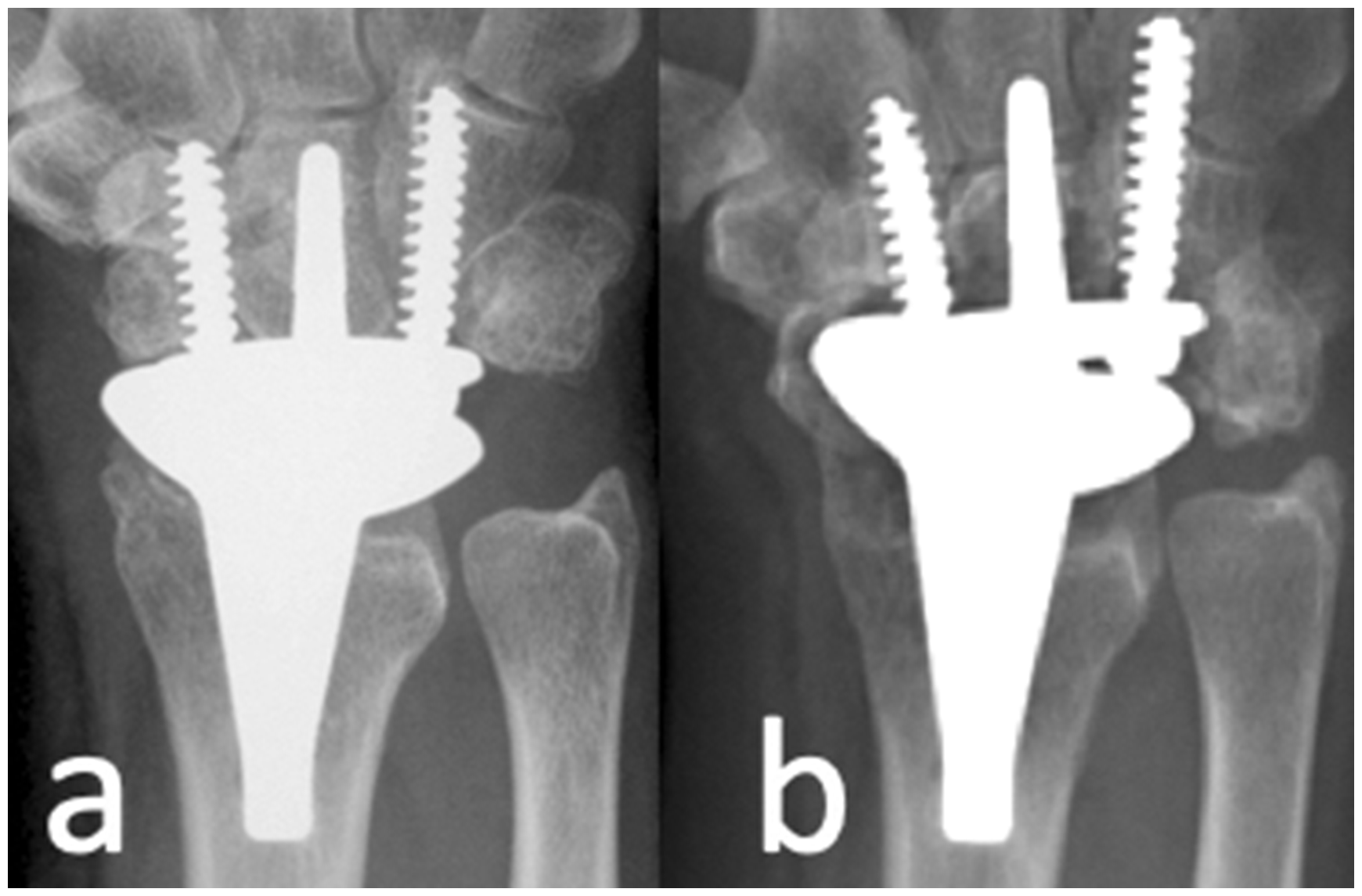
(a) Periprosthetic osteolysis under the carpal plate and under the near joint extremity of the radial component 2 years after a Remotion total wrist arthroplasty and (b) Six years after the arthroplasty the carpal component has subsided, but the radial component remains well fixed.
A TWA that is loose and failed will require a reoperation. Removal of the implant and either a revision arthroplasty or arthrodesis is a possible option. Arthrodesis after a failed older-generation TWA is challenging due to the large bone defects that result from the extraction of the bulky implants (Beer and Turner, 1997; Cooney et al., 1984; Menon, 1987; Vogelin and Nagy, 2003; Volz, 1984). Even after extraction of a fourth-generation implant, grafting of the residual bony defect with an iliac crest autograft or an allograft is usually required to restore carpal height and enable stable fixation. Extraction of osseointegrated components (typically the radial component) may also be problematic. The radius may need to be split to facilitate removal of the implant and cement, and cerclage wires may subsequently be needed to stabilize the radius.
Intramedullary Steinmann pins, in some cases supplemented with staples, have been the most common method for arthrodesis, but substantial complications and nonunion rates have been reported (Beer and Turner, 1997; Carlson and Simmons, 1998; Ferlic et al., 1992; Radmer et al., 2003; Rizzo et al., 2011). More recently, plate and screw fixation has become the preferred option for arthrodesis (Grandizio and Maschke, 2017) (Figure 5). Adams et al. (2016) published a series of 20 wrists, including 15 revisions of a fourth-generation TWA and five older-generation implants. All patients were treated with a dedicated wrist arthrodesis dorsal plate (Synthes, West Chester, PA, USA) and a contoured cancellous femoral head structural allograft. Of the 20 wrists, 19 fused at the first attempt at a median of 4 months. Proximal plate loosening occurred in one wrist, but the joint still fused at 6 months. Reigstad et al. (2017) published a series of 11 failed Motec or Elos wrist arthroplasties (Swemac Orthopaedics AB, Linköping, Sweden) for osteoarthritis, which were subsequently converted to arthrodesis using an arthrodesis plate in eight cases or a customized peg in three cases. Clinical and radiological bone union was achieved in all the operated wrists. Rizzo et al. (2011) reported on the functional results after TW arthrodesis for failed arthroplasty. Of 21 wrists, 14 had no pain. The group of patients with persistent nonunion of the arthrodesis had an average pain score of 3.3 (range 0–7) versus an average pain score of 2.1 (range 0–4) in the group that fused. The average overall Disability of the Arm Shoulder and Hand (DASH) score was 33 (range 11–59), with an average score of 29 (range 11–45) in the fused group and 36 (range 13–57) in the nonunion group. Return to work data were applicable in only 10 patients, of whom four were able to return to their previous level of work, four returned to work with some degree of restriction and two ceased work.
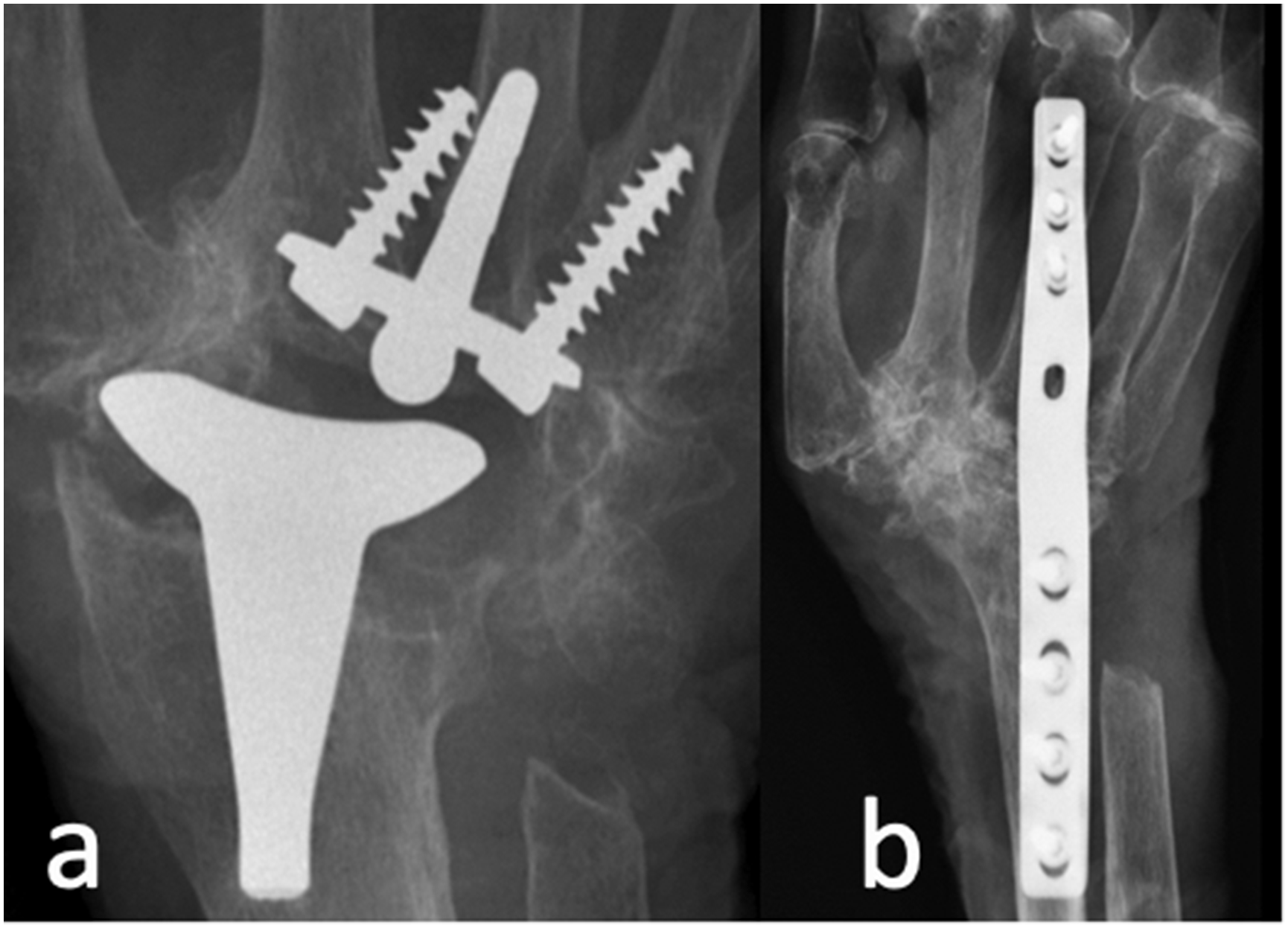
(a) Failed Remotion total wrist arthroplasty in a rheumatoid patient with subsidence of the carpal component while the radial component is still fixed and (b) Salvage by wrist arthrodesis after removal of all prosthetic components.
Revision arthroplasty is an alternative solution to arthrodesis. In the situation of aseptic loosening of the carpal component only, this component can be exchanged while preserving the radial component. When both components have loosened, and an acceptable bone stock still is present, total exchange may be indicated. Talwalkar et al. (2005) reported on 10 failed Biaxial implants, six of which underwent a revision to a second biaxial wrist replacement, with a follow-up of 28 months. None of the re-revisions required further surgery during this short follow-up period. Complications after revision arthroplasty were frequent in a series of 69 patients who underwent 76 revision procedures of various implants, mostly older generation implants from 1974 to 2013 (Wagner et al., 2021). They included distal loosening (n = 15), proximal loosening (n = 3), dislocation (n = 7), intraoperative fracture (n = 7), postoperative fracture (n = 2) and component fracture (n = 3). In a personal series of 10 cases by one of the authors of this article, half of the revised TWAs were ultimately converted to wrist arthrodesis within a mean follow-up period of 31 months (range 3–102) (Boeckstyns, 2021). All arthrodeses healed by first intention and the patient-reported outcome measures (PROMs) in the patient with fused wrists did not differ significantly from those in the patients with functional revision arthroplasties. The PROM scores were similar to those reported by Rizzo et al. (2011).
Discussion
TWA is a challenging surgery and is associated with relatively high complication rates. The aim of this review article was to report on the incidence and treatment of complications after TWA, and not to compare TWA with total wrist arthrodesis. While early intraoperative and early postoperative complications have an acceptable incidence, late complications, such as osteolysis and implant loosening, occur relatively frequently, even with the newer generation designs. Long-term survival is low when compared with the 10-year revision rates of 5% or lower for hip replacement as required by the National Institute for Heath and Care Excellence (NICE, 2014), and when compared to the shoulder or elbow replacements, but seems to be superior to total ankle replacement. Though young age, high physical demands, poor bone quality and concurrent medical conditions are generally considered to play a role, to our knowledge, no hard data are available to clearly identify risk factors associated with prosthetic failure. The main concern still is loosening of the distal component in the bi-component TWA. Efforts must be made to minimize the problem by improving distal fixation. The Freedom implant attempts a more stable fixation by using locking screws, which seems rational, but long-term results are not yet available to document the benefit. Other materials must be tested in view of avoiding wear of noxious particles. Hemiarthroplasty, using a radial component only, has been used for the salvage of irreparable intra-articular distal radial fractures in the elderly patient (Benedikt et al., 2022; Herzberg et al., 2015) and combined with proximal row carpectomy for other rheumatoid or degenerative conditions (Adams, 2013; Vance et al., 2012). Obviously, this approach excludes problems of carpal component loosening, but other problems may occur and only short-term results have been reported. Reverse hemiarthroplasty using a distal component only yielded unreliable results (Huish et al., 2017). The Amandys pyrocarbon bears its own postoperative instability problems requiring frequent reoperation, and no long-term results have yet been published. Much of our knowledge on the aetiology of osteolysis as well as the principles of management of an infected or a loose TWA can be transferred from what we have learned dealing with similar problems in bigger joint arthroplasty, such as hips, knees and shoulders.
Total wrist arthrodesis is the most used procedure for the salvage of failed TWA. Alternatively, failed implants could be salvaged by implant revision, but the reported implant survivals seem lower compared with the primarily implanted fourth-generation TWA. There is no doubt that the added costs, the difficulty and the risks of each supplemental revision procedures are high.
Only few articles report PROMs after revision arthroplasty. Pinder et al. (2018) had PROM data on six of the 18 patients with inflammatory disease in their series. The median Quick DASH score was 57 (range 9–89) and median Patient-Rated Wrist Evaluation (PRWE) score was 35 (range 13–90). Fischer et al. (2018) reported on 16 revision TWA after failure of primary TWAs of various designs in rheumatoid patients. The cumulative implant survival was 74%, and the median DASH and PRWE scores at 5 years were 60 and 37, respectively. In another series of 19 cases, the cumulative 5-year implant revision survival was 83% (Pinder et al., 2018). Zijlker et al. (2019) published a series of 40 wrists in 37 patients with a failed biaxial prosthesis that were converted to a Universal 2 total wrist arthroplasty. Of the 40 implants, 16 eventually failed. The cumulated 5-year survival was 87% and the 9-year survival was 60%. There was no significant difference between rheumatoid and non-rheumatoid patients in terms of implant failure. Patient-Rated Wrist and Hand Evaluation (PRWHE) and Quick DASH scores were 53 and 47, respectively, for the arthroplasties that remained functional. Rizzo et al. (2011) reported 21 wrists with a TWA for inflammatory disease that were revised to wrist arthrodesis. In the 13 wrists that ultimately fused, the mean DASH score was 29. Reigstad et al. (2017) also report a mean Quick DASH score of 32 (SD 20) and a mean PRWE score of 29 (SD 20) in 11 cases with osteoarthritis. The numbers in these series were very small and must consequently be assessed very carefully. However, they could indicate that, in terms of PROMs, revision arthroplasty is not superior to revision arthrodesis. It can also be questioned whether there are patient-related factors that caused the failure of the primary arthroplasty, which in turn can cause the failure of a revision implant if not identified and eliminated. For these reasons, total wrist arthrodesis should be the procedure of first choice for most failed TWAs and revision arthroplasty should be reserved for very carefully selected patients only. These could be relatively low-demand patients who especially need to maintain some wrist motion. Future studies must be carried out to identify which patients would most likely benefit from a revision TWA compared to a total wrist arthrodesis.
A weakness of this retrospective review is the paucity of unbiased long-term reports of the most recent implants that exists in the published literature. Several reports are authored or co-authored by surgeons who are closely involved in the development or production of total wrist implants and many series include only small numbers of patients with a rather short follow-up period. We believe the inclusion of the fourth-generation implants that are no longer available in the market was important to assess late complications and their treatment.
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.