
Abstract
This study investigated the use of an upper limb hybrid assistive limb for elbow flexion biofeedback training in recovery from brachial plexus injury in both the postoperative and chronic phases. No adverse events were observed in any patient.
Keywords
Traumatic brachial plexus injury (BPI) causes severe peripheral nerve palsy resulting in upper limb dysfunction. Intercostal nerve-to-musculocutaneous nerve (ICN-MCN) transfer represents one method of elbow flexor reconstruction and allows more than half of patients with BPI to actively flex their elbow against gravity postoperatively (Ochiai et al., 1993). However, some patients present with poor voluntary elbow flexion postoperatively. Although several risk factors play a role in poor recovery, including age, duration between injury and surgery, and surgical technique, extended rehabilitation after surgery is also an important factor to consider (Doi et al., 2022). The upper limb hybrid assistive limb (HAL) (Figure 1) is a wearable motor-assisted robot that detects the muscle action potential (bioelectric signal) on the skin of the upper arm, and controls or activates an actuator located lateral to the elbow joint to support elbow flexion and extension (Sankai and Sakurai, 2018). The HAL detects muscle action potentials from surface electrodes attached to the biceps brachii and triceps brachii. These fine bioelectric signals are not strong enough to induce joint movement of the Medical Research Council (MRC) grade 1 or 2. The HAL enables and assists voluntary elbow flexion and extension in real time. The aim of the present study was to examine the feasibility of using a newly developed upper limb HAL during elbow flexion biofeedback training for BPI.
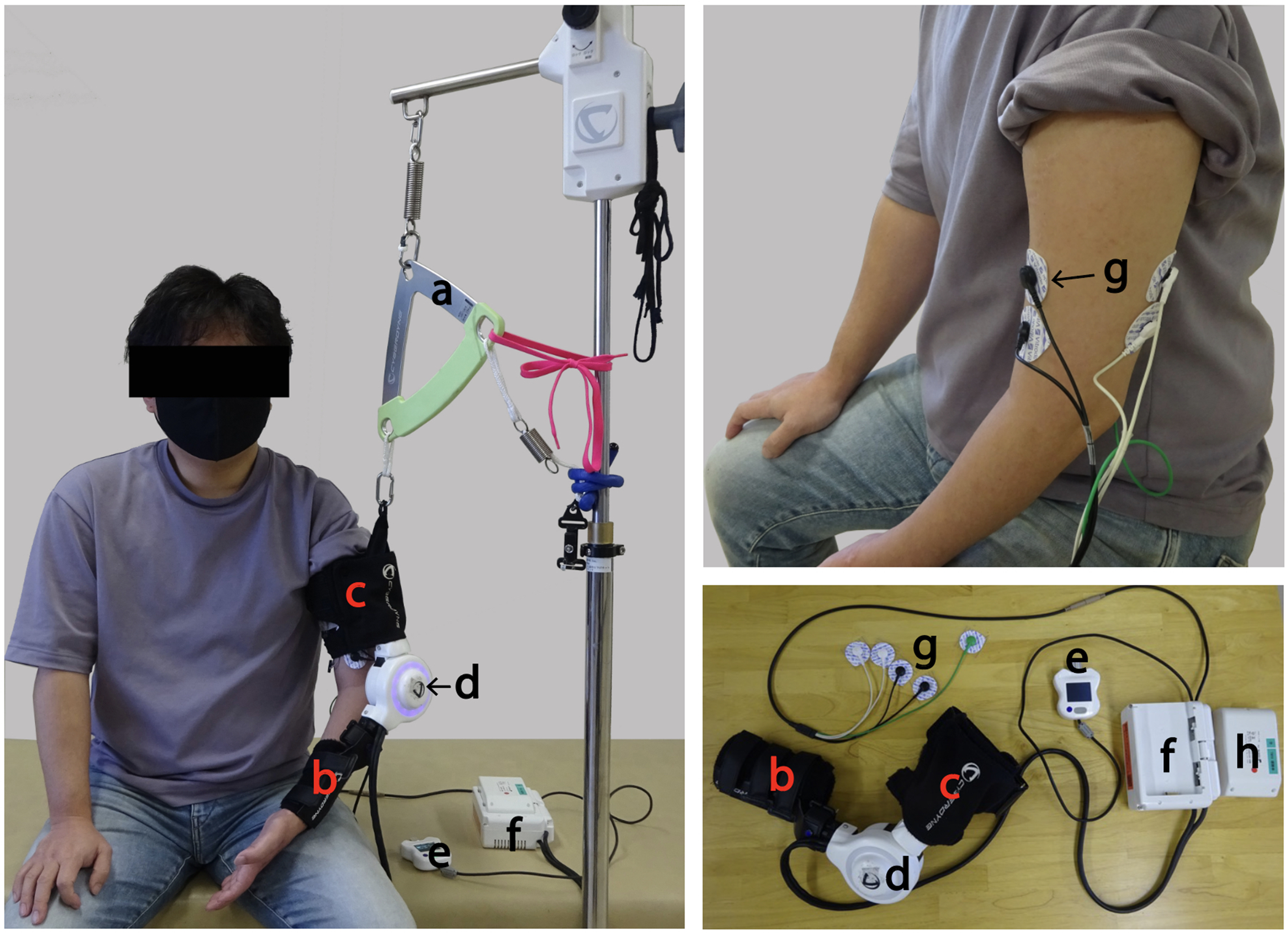
The upper limb HAL is composed of (a) a suspending device, (b) forearm attachment, (c) arm attachment, (d) HAL actuator, (e) handy controller, (f) control device, (g) HAL surface electrode sensors and (h) a battery. HAL: hybrid assistive limb.
A total of 13 patients (9 men, 4 women; mean age 35.8 years) with previous BPIs participated in this study. Of them, 12 patients were injured in a traffic accident and one patient had a sports-related injury. The types of BPIs were as follows: four C5–6, one C5–7, one C5–8 and seven whole BPI types. In total, 12 patients underwent elbow flexor reconstruction for BPI (ICN-MCN transfer, n = 7; intercostal nerve-to-thoracodorsal nerve, n = 1; partial ulnar nerve transfer, n = 2; and nerve grafting, n = 2) and one patient (sports injury) underwent conservative treatment. Elbow training using the upper limb HAL was performed in patients in the acute or chronic phases of BPI. Elbow flexion training with upper limb HAL was performed by patients at a frequency ranging from once weekly to once monthly, mainly on an outpatient basis. Each session of elbow flexion training using upper limb HAL (consisting of a vital sign check, pre-assessment, upper limb HAL training and post-assessment) lasted approximately 60 min. The patients performed the maximum number of repetitions of elbow flexion with the upper limb HAL in each session; however, the number of repetitions was adjusted according to the level of patient motivation and endurance (approximately 200–300 elbow flexions/session). To evaluate the feasibility of elbow flexion training with upper limb HAL in patients with BPI, the following were studied: number of upper limb HAL sessions; duration of the HAL programme (months); number of postoperative months (POM); postoperative years (POY) since starting the HAL training (HAL start) and completion (HAL finish); biceps MRC grade; and HAL-related adverse events.
The mean duration since surgery was 49.5 POM (SD 79.9) in the 12 patients with BPI, with the exception of the patient who underwent conservative therapy, whose duration since the injury was 4 months. Patients with BPI (n = 13) underwent 21.5 HAL sessions (SD 15.7). The biceps MRC grade at HAL start of the 12 patients (excluding a conservative patient) was 0 (0, 0%), 1 (10, 83.3%), 2 (0, 0%), 3 (1, 8.3%), 4 (1, 8.3%) and 5 (0, 0%); the grade at HAL finish was 0 (0, 0%), 1 (3, 25.0%), 2 (1, 8.3%), 3 (6, 50.0%), 4 (2, 16.7%) and 5 (0, 0%), respectively. No serious adverse events associated with upper limb HAL were observed in any of the 13 patients. Other adverse events, such as upper limb pain, excessive fatigue or abrasion of the affected upper limb, were not observed during elbow flexion training with the upper limb HAL in any patient.
After functional reconstruction of the elbow function in BPI, upper limb HAL training is performed such that elbow movement can be induced starting immediately after reinnervation of the disabled joint is achieved (elbow flexor power MRC grade 1). This approach has advantages. First, it becomes practical to learn complete elbow flexion at an early phase of rehabilitation. Second, it is practical for proprioceptive sensibility input (elbow joint). Third, there is increased ease of contraction of the reinnervated muscle due to flexion of the elbow with the upper limb HAL. Finally, insensitivity to co-contractures was achieved in patients with upper palsy. We believe that the sequence of these events, associated central nervous system plasticity and the possibility of efficient induction in this study helped to achieve positive results. We attribute the successful outcomes in our patient group to a combination of effective conventional rehabilitation and high compliance levels. Doi et al. (2022) reported the outcomes of virtual rehabilitation of elbow flexion using single-joint HAL for patients with BPI. HAL replaced the elbow flexion muscle action potential with elbow flexion force before the reinnervation detection stage, thus expediting speeding up learning for patients and shortening the rehabilitation period. The significant differences between the report by Doi et al. and our own report is the inclusion of patients with chronic BPI who have experienced long-term injuries and surgeries, as well as a conservative patient. We demonstrated that upper limb HAL training was feasible without serious adverse events for both patients with chronic and acute-phase BPI. Biofeedback therapy using other devices has already become the standard and conventional treatment for BPI. Any further work should compare the effectiveness of HAL training with that of conventional biofeedback therapy.
Footnotes
Acknowledgements
We would like to thank Mayuko Sakamaki and Yumiko Ito, Center for Innovative Medicine and Engineering (CIME), University of Tsukuba Hospital, for their excellent technical assistance.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Industrial Disease Clinical Research Grants of the Ministry of Health, Labour and Welfare, Japan (14060101-01), the Japan Society for the Promotion of Science (JSPS) KAKENHI (grant no. 20K19303) (Grant-in-Aid for Young Scientists) and the ZENKYOREN (National Mutual Insurance Federation of Agricultural Cooperation).
Ethical approval
This study was approved by the ethics committee of our university (TCRB18-38).
Informed consent
The patient was informed about the aim and design of this study and provided written informed consent for participation and publication.