
Abstract
We developed a finger motion-based diagnostic system for carpal tunnel syndrome by analysing 10 second grip-and-release test videos. Using machine learning, it estimated presence of carpal tunnel syndrome (89% sensitivity and 83% specificity) and correlated with severity on nerve conduction studies (coefficient 0.68).
Level of evidence
III
Patients with carpal tunnel syndrome (CTS) frequently have complaints of hand clumsiness even without thenar atrophy. Nerve conduction studies (NCS) suggest that both sensory and motor impairment occur early in CTS (Loscher et al., 2000). However, assessing early motor impairment may be challenging due to its subtle manifestations. Recently, smartphone-based markerless motion capture technology for hands and machine learning have been developed, and their combination enables further analysis of motion features. We hypothesized that changes in finger motion due to CTS could be evaluated by recording simple hand movements, such as the 10-s grip-and-release test (10-s test), usually used for cervical myelopathy examination, and analysing them with machine learning.
This study included 25 patients (20 women, 5 men) with CTS (38 hands) and 34 volunteers (17 women, 17 men) (65 hands). Hand surgeons diagnosed CTS based on specific symptoms, physical examination and NCS, which were categorized according to the Bland classification (Table S1). Thirty-one hands were classified as grade 3 or worse on NCS. The control group had no symptoms of CTS. Both groups had no specific symptoms of other diseases affecting hand movement. All participants completed the Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire.
The methods followed our previous study (Ibara et al., 2023). We recorded the 10-s test’s movement using a smartphone (Figure 1(a)). We used MediaPipe Hands (Google, California, USA), which could estimate 21 feature points on the hand from the hand gesture video. Each point was represented as a three-dimensional coordinate system. The origin was located at the centre of the wrist, and one axis was located in the line of the index finger (Figure 1(b)). The position of each point, excluding the origin at the wrist, was calculated using an adjusted coordinate system. Subsequently, we applied two preprocessing steps. First, the time series data of the feature values were divided into 20 data frames along the time axis (64 frame length). Second, each 60-dimensional feature value was converted into frequency characteristics using a fast Fourier transform, and 32 frequency feature values were extracted (Figure S1).
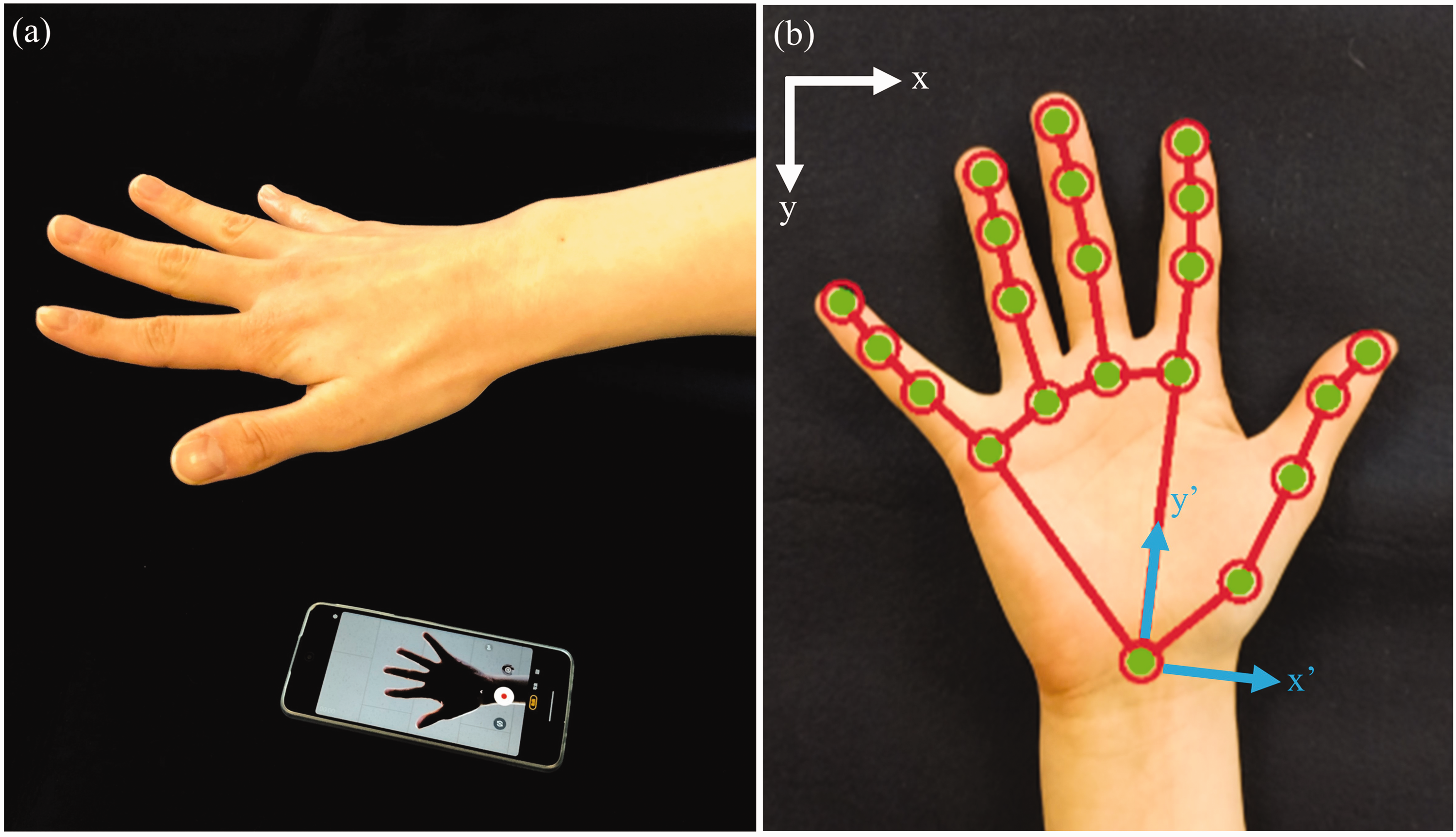
(a) Setting of the measurement. (b) Hand tracking with MediaPipe Hands. White arrows: original coordinate system; blue arrows: adjusted coordinate system. x’-axis: adduction-abduction direction, y’-axis: distal-proximal direction, z’-axis: flexion-extension direction.
We created a binary classification model using a support vector machine classifier to distinguish CTS from non-CTS hands (Figure S1). The classification process was repeated for 20 data frames independently, with the final classification result being the average of these frames. A model with parameters for each finger and direction was created to identify the fingers contributing to the classification. In the validation phase, 10-fold cross-validation was used.
Based on the Bland classification and DASH score, random forest analysis was performed to evaluate the relationship between the acquired dataset and disease severity (Figure S1). The independent variable was set as the Bland classification or DASH score, and the explanatory variables were set as the feature values determined in the final classification model. The average of the 20 regression results for each segment was used as the final result. Leave-one-subject-out cross-validation was performed during the validation phase. All data analyses were performed using Python software (Python Software Foundation, Wilmington, DE, USA).
The sensitivity and specificity of the model, which included all variables representing the features, were 87% and 75%, respectively. The model focusing on the little finger’s DIP joint in the z’-axis (flexion-extension) direction exhibited the highest area under the curve value (89% sensitivity and 83% specificity) (Figures S2(a–d) and S3). Although this finding was unexpected due to the median nerve innervation, it is not surprising given the complexity of human motor control (Napadow et al., 2006). Furthermore, a previous study showed that the little finger was released later in patients with CTS (Sasaki et al., 2020).
Regression analysis showed correlation coefficients of 0.68 and 0.31 with the Bland classification and DASH score, respectively (Figures S4(a, b)). The correlation was modest for the Bland classification score and weak for the DASH score. The DASH score may have a weaker correlation because it reflects bilateral upper extremities symptoms. However, the Bland classification assesses the nerves’ electrophysiological state; therefore, a relationship between it and the changes in finger motion in CTS was suggested.
This study had some limitations. The CTS group included mostly severe cases, while the control group may have included asymptomatic CTS and other excluded diseases. In addition, significant differences were found in sex between the two groups.
Based on this study’s results, we aim to develop a system for analysing disease-specific action patterns. By developing models for other diseases affecting finger motion, we may develop screening systems for other diseases (Ibara et al., 2023).
In conclusion, we developed a model that was able to confirm diagnosis of CTS using a 10-s test with a smartphone and a machine learning algorithm. The model could differentiate between a normal hand and one with severe CTS in our pilot study. This method’s non-invasiveness and simplicity could facilitate self-screening for CTS in daily life, leading to earlier detection and treatment. Further research is warranted to validate and refine this method.
Supplemental Material
sj-jpg-1-jhs-10.1177_17531934231214661 - Supplemental material for Diagnosis of carpal tunnel syndrome using a 10-s grip-and-release test with video and machine learning analysis
Supplemental material, sj-jpg-1-jhs-10.1177_17531934231214661 for Diagnosis of carpal tunnel syndrome using a 10-s grip-and-release test with video and machine learning analysis by Kazuya Tsukamoto, Ryota Matsui, Yuta Sugiura and Koji Fujita in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-jpg-2-jhs-10.1177_17531934231214661 - Supplemental material for Diagnosis of carpal tunnel syndrome using a 10-s grip-and-release test with video and machine learning analysis
Supplemental material, sj-jpg-2-jhs-10.1177_17531934231214661 for Diagnosis of carpal tunnel syndrome using a 10-s grip-and-release test with video and machine learning analysis by Kazuya Tsukamoto, Ryota Matsui, Yuta Sugiura and Koji Fujita in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-jpg-3-jhs-10.1177_17531934231214661 - Supplemental material for Diagnosis of carpal tunnel syndrome using a 10-s grip-and-release test with video and machine learning analysis
Supplemental material, sj-jpg-3-jhs-10.1177_17531934231214661 for Diagnosis of carpal tunnel syndrome using a 10-s grip-and-release test with video and machine learning analysis by Kazuya Tsukamoto, Ryota Matsui, Yuta Sugiura and Koji Fujita in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-jpg-4-jhs-10.1177_17531934231214661 - Supplemental material for Diagnosis of carpal tunnel syndrome using a 10-s grip-and-release test with video and machine learning analysis
Supplemental material, sj-jpg-4-jhs-10.1177_17531934231214661 for Diagnosis of carpal tunnel syndrome using a 10-s grip-and-release test with video and machine learning analysis by Kazuya Tsukamoto, Ryota Matsui, Yuta Sugiura and Koji Fujita in Journal of Hand Surgery (European Volume)
Footnotes
Acknowledgements
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI (grant no. JP21H03485), JST PRESTO (grant no. JPMJPR2134) and the Japanese Society for Surgery of the Hand.
Ethical approval
Ethical approval for this study was obtained from the ethics committee of Tokyo Medical and Dental University.
Informed consent
Written informed consent was obtained from all participants before the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.