
Abstract
Wrist arthroscopy is a valuable and widely utilized tool in the treatment of triangular fibrocartilage complex (TFCC) injuries. These procedures include synovectomy alone, peri-capsular or transosseous repair, and arthroscopic-assisted reconstruction, and each are associated with specific complications. This review describes the types of complications and their rates in different types of arthroscopic TFCC surgery reported in the literature and in our centre. Across the spectrum of arthroscopic TFCC surgery, complication rates and the learning curve increase with surgical complexity. Relevant anatomy, prevention and management of complications including nerve injury and irritation, extensor tendon injury and tendinitis, fracture, stiffness, and persistence of symptoms or instability are discussed. Vigilance to anatomical details and careful dissection can help to reduce complications that may result in disturbing pain and functional loss.
Keywords
Introduction
Wrist arthroscopy has become an increasingly popular tool for the treatment of a variety of wrist conditions since its first published description in 1979 (Chen, 1979), and has since earned an important place in the armamentarium of hand surgeons. It is generally considered a safe procedure, with a low complication rate of 5.98% as reported in a multicentre review (Leclercq and Mathoulin, 2016). It provides detailed information on the status of articular structures and enables targeted surgery without the additional trauma of an open arthrotomy. These two characteristics make it a particularly invaluable tool for the treatment of triangular fibrocartilage complex (TFCC) disorders, when symptoms remain severe despite conservative treatment. A magnified view of both the distal and proximal parts of the TFCC combined with tactile assessment allows for detailed diagnosis of the type of TFCC injury and helps with decision making regarding treatment. Furthermore, arthroscopic access for TFCC repair or reconstruction eliminates the need for detaching the distal radioulnar joint (DRUJ) and ulnar wrist capsule from the dorsal TFCC and distal ulna, which may itself produce capsular contracture and secondary symptoms. Arthroscopic TFCC repair has been shown to yield similar outcomes compared with open repair, with fewer patients experiencing nerve pain (Anderson et al., 2008). However, arthroscopic access in the presence of tendons and neurovascular structures, including sensitive cutaneous nerves clustered at the wrist, places considerable demands on the knowledge and skill of the surgeon. A detailed knowledge of anatomy, a sensitive tactile feedback and meticulous technique are required to ensure the accurate and safe creation of portals, instrumentation, suturing and passage of tendon graft. In particular, for the ulnar side of the wrist, precise anatomical knowledge of dorsal branches of the ulnar nerve and their variations is essential. As with most types of surgery, a learning curve exists, and an inverse relationship between experience and complication rate in wrist arthroscopy has been shown by a multicentre retrospective study (Leclercq and Mathoulin, 2016). They reported a minimum threshold of approximately 25 arthroscopies a year and/or greater than 5 years of experience for a surgeon to have a lower complication rate.
The potential surgical complications and their risks depend on the specific type of TFCC surgery, in addition to the anatomical and surgeon-related factors mentioned above. A myriad of different techniques exists in the literature that address the different types of TFCC tears; and multiple techniques exist even for any given type of tear. In general, arthroscopic repair techniques fall into categories of outside-in, inside-out and all-inside methods. For TFCC foveal tears (Atzei Classes 2 and 3 of the Palmer 1b tear) (Atzei, 2009), two categories of repair have been described, peri-foveal capsular repair and direct foveal (transosseous) fixation. For the purpose of this article, the procedures that will be covered will be grouped into TFCC debridement for traumatic or degenerative central tear, repair of an ulnar-sided TFCC tear, dorsal TFCC repair and TFCC reconstruction under arthroscopic assistance.
Overview of complication rates in arthroscopic TFCC surgery
Studies on the complications of wrist arthroscopy and on the outcomes of arthroscopic TFCC repair and reconstruction provide data on complications related to arthroscopic TFCC surgery. In a single-centre review on complications related to wrist arthroscopy, four complications were encountered out of 78 arthroscopic procedures involving the TFCC, including two cases of dorsal ulnar sensory neurapraxia and one case of ulnar neurapraxia (Beredjiklian et al., 2004). A systematic review of 18 studies on TFCC debridement alone for stable tears found that out of 456 patients, 11 (2%) had complications (Saito et al., 2017). A review of arthroscopic TFCC repair for peri-foveal capsular TFCC and dorsal TFCC repairs in 35 patients in our centre found complications in 7 (20%) patients, all with minor adverse effects. Of these, six were related to neurapraxia or irritation of the dorsal branch of ulnar nerve (Estrella et al., 2007). A systematic review of seven studies involving 131 patients who underwent TFCC transosseous repair reported a complication rate of 10.7% (n = 14/131) (Jung et al., 2021). A series of 28 patients with arthroscopic-assisted TFCC reconstruction in our centre with a 5-year mean follow-up reported complications in 7 (25%) patients (Mak and Ho, 2017). Another series of 11 patients with arthroscopic TFCC reconstruction reported complications in nine patients (Luchetti and Atzei, 2017). An all-inside arthroscopic TFCC reconstruction technique was reported in a series of five patients with no complications (Atzei et al., 2023); this was attributed to the authors not having used any incision over the distal ulna and an overall minimal surgical access.
Specific and relevant complications to each type of procedure will be discussed below in more detail, including anatomical considerations, suggestions on reducing risks and management of these complications (Supplementary Table S1).
Complications related to TFCC debridement
Early complications
Arthroscopic TFCC debridement is the least invasive procedure on the TFCC, usually requiring only two or, less commonly, three arthroscopic portals. Complications that may occur are those that are applicable to wrist arthroscopy in general. These include infection, complications related to the traction setup and thermal injury related to the use of radiofrequency.
Infection
In a systematic review of 456 patients with arthroscopic TFCC debridement, septic arthritis was reported in 1 (0.2%) patient (Saito et al., 2017). Infection of the joint is rare and prophylactic antibiotics are not routinely given unless implants are used. Theoretically, wet arthroscopy may have a lower infection risk as the joint is continuously lavaged with fluid, unless that fluid itself is the source of contamination. Arthroscopic washout combined with 6 weeks of antibiotics is the standard treatment in our centre (Chow et al., 2020).
Setup-related complications
Complications directly related to arthroscopic setup include burns from a hot traction tower and neurapraxia of digits from over-zealous traction (Beredjiklian et al., 2004). These can be prevented if the placement on the traction tower is done with due care by the surgeon, with padding applied to areas where the traction tower is in contact with the patient’s skin, and ensuring traction does not exceed 15 lbs.
Thermal injury from radiofrequency
The use of radiofrequency may cause iatrogenic injury to neighbouring tissues, ranging from tissues within the joint to the skin at the portal site. Irreversible cell death in cartilage occurs with exposure to 50°C for 5 minutes (Voss, 2006). Thermal injury causing widespread cartilage damage has been reported after TFCC debridement (Giddins et al., 2021). This may occur if the temperature inside the joint is allowed to build due to a burst of high energy over a short time, or if fluid inflow and outflow are not well established. The extensor tendons are also at risk during the use of radiofrequency because of their close proximity to the dorsal capsule (Giddins et al., 2021). When performing dorsal debridement of TFCC or synovectomy, in addition to adequate fluid flow, care has to be taken to avoid over-concentration of energy at a particular spot. Tendon ruptures due to thermal injury may not be immediately apparent and tend to present 2–3 weeks after surgery.
Nerve irritation and injury
Saito et al. (2017) reported an incidence of injury of 0.8% to the dorsal branch of the ulnar nerve (DBUN) after wrist arthroscopy in a systematic review. Portals on the ulnar side of the wrist, including the 6U, 6R and 4/5 portals, are close to the DBUN, and nerve irritation or injury during instrumentation or portal creation may cause symptoms at the ulnar dorsal part of the hand. The 6R portal is commonly used in TFCC debridement and may be very close to or right over the DBUN. Therefore, careful portal creation technique has to be used at all times, with a superficial skin-only incision and gentle spreading of subcutaneous tissue with blunt artery forceps. The anatomy of the nerve branches, prevention and management of nerve injuries are further discussed in the section on TFCC repair.
Mid-term complications
Instability of the distal radioulnar joint
In general, the articular disc is not a major stabilizer within the TFCC. However, DRUJ instability may occur with excessive debridement of more than two-thirds of the disc (Adams, 1993), or if parts of the dorsal or volar radioulnar ligaments are debrided. Therefore, debridement should be limited to trimming of the unstable rim only.
Persistence of symptoms
After arthroscopic debridement alone for stable or degenerative TFCC tears, persistent pain may be caused by recurrent synovitis or ongoing ulnar impaction syndrome. A systematic review has shown that TFCC debridement alone in the presence of positive ulnar variance is associated with worse outcomes of satisfaction and Mayo Modified Wrist Score compared with ulnar neutral and negative variance (Saito et al., 2017). In the presence of significant positive ulnar variance, unloading of the ulnocarpal joint by the wafer procedure or ulnar shortening osteotomy, in addition to debridement, may lead to better outcomes.
Complications related to repair of an ulnar-sided TFCC tear
Early complications
Nerve irritation and injury
Compared with debridement alone, nerve-related complications are relatively more frequent in TFCC repair, especially if dissection on the ulnar side is required. Of particular relevance to TFCC surgery is the ulnar nerve and its dorsal sensory branch (DBUN). High-grade injury to the ulnar nerve proper is quite unusual during an arthroscopic TFCC repair, as it is located a few millimetres away from the volar-ulnar joint capsule at the radiocarpal joint level. However, one case of transection injury of the ulnar nerve has been reported in the literature from placement of a trocar at the 6U portal (Nguyen et al., 2011). More commonly affected is the DBUN, which bifurcates from the ulnar nerve 5 cm proximal to the pisiform, exits from beneath the flexor carpi ulnaris tendon, runs subcutaneously around the distal ulna within 1 cm of the ulnar head, and runs towards the ulnar two digits dorsally and occasionally up to the ulnar aspect of the middle digit. Cadaveric studies examining anatomical variations of the DBUN and its relationship to arthroscopic portals have found that the 6U portal was directly located over a branch of the DBUN in many specimens, and the 6R portal was at a mean of 8 mm and a minimum of 2 mm from the DBUN, which also places it at risk of injuring the nerve (Shyamalan et al., 2016). Another study of 20 cadaver specimens showed that the DBUN consistently intersected a line joining the ulnar styloid and the fourth web space at 24 mm along this line or at 23% of its length distal from the ulnar styloid (Tindall et al., 2006). Based on this finding the authors recommended a ‘safe zone’ for the 6R portal to be within one-fifth of this line proximally. Symptoms related to the DBUN was reported in 17% of patients with peripheral pericapsular TFCC repair (Estrella et al., 2007). These authors found the DBUN being entrapped by a suture in one patient.
The arborization pattern of the DBUN is also an important consideration. Two to five terminal branches arise around the level of ulnar styloid, including a transverse branch in 20 out of 24 specimens (Lourie et al., 1994). In dissections of 45 cadaver specimens, a transverse branch was found in 12 of 45 specimens (Ehlinger et al., 2005). They described two patterns: type 1 was proximal to the ulnar styloid (2 out of 12) and type 2 was distal (10 out of 12). A type 1 transverse branch is particularly risky for portals and incisions at the DRUJ. The mean distance from the 6R portal was 3.68 mm (range 1–14.9). The anatomy, transverse branch patterns and distance from the 6R and 6U portals are illustrated in Figure 1. Neuroma formation of the transverse branch after surgery in the region of the DRUJ was reported in three patients, who were all treated successfully with a simple neuroma excision (Lourie et al., 1994). Portals for the DRUJ (proximal, distal and direct foveal portals) are increasingly adopted and gaining popularity for TFCC surgery. Although anatomical studies of the relationship of these portals to the DBUN are lacking, it can be assumed that they are also at close proximity to the transverse or main branches and similar nerve injuries to those described by Lourie et al. (1994) can also be caused by DRUJ arthroscopy.
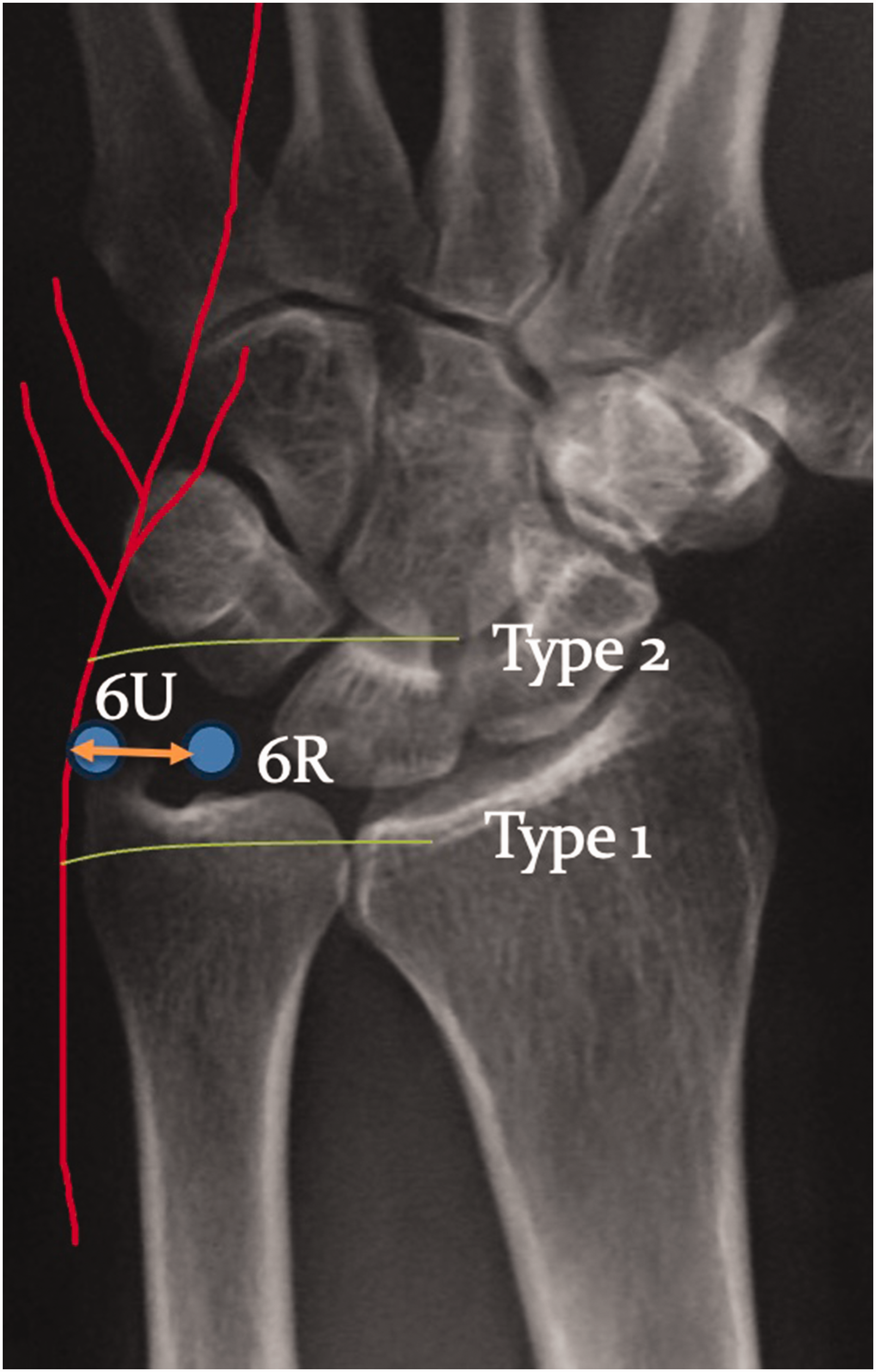
Schematic drawing of type 1 and type 2 transverse branch of the dorsal branch of the ulnar nerve. Dorsal branch of the ulnar nerve (red) transverse branch patterns (green), arrow showing the distance of the dorsal branch from the 6R portal (mean of 8 mm, minimum of 2 mm).
Compared with the pericapsular method of TFCC repair, a systematic review of transosseous repair found no nerve-related complications, which may be related to the use of a different incision that is dorsal and proximal to the dorsal branches of the ulnar nerve (Jung et al., 2021).
Risks of injury to these superficial nerve branches could be mitigated by correct portal placement, which can be facilitated by direct arthroscopic visualization of a needle in the intended portal site, and adjustments can be made accordingly. For example, for the 6R portal, the needle should be seen radial to the extensor carpi ulnaris (ECU) sub-sheath and parallel to the joint. However, even with accurate portal locations, injury to these superficial nerve branches could still occur due to their close proximity to and sometimes overlapping with the 6U and 6R portals and possibly the DRUJ portals, as evidenced from the anatomical studies discussed. Therefore, a ‘nick and spread’ technique is fundamental in wrist arthroscopy. With the wrist suspended in a traction tower, the surgeon should use his/her thumb and index finger to stabilize the patient’s skin before cutting the skin. The subcutaneous tissue, superficial nerves if any, and extensor tendons should be spread apart with blunt dissection using a fine haemostat while the wound is gradually deepened to perforate the capsule. Use of a sharp stab wound incision down to the capsule to make a portal should be avoided. A heightened tactile awareness during introduction of any instruments is important and can help to alert the surgeon to the presence of structures in the way of entry. After puncturing the joint capsule, the introduction of instruments should be done smoothly without much force. For the 6U and direct foveal portals, placing the forearm in full supination maximizes the distance of the DBUN from the portal and exposes the foveal region for access, since the ulnar styloid and ECU tendon are displaced dorsally. The maximum distance between the nerve and 6U portal occurs in forearm supination with the wrist in flexion (Esplugas et al., 2014); however, when the wrist is neutral and under traction, full forearm supination alone significantly increases the safety margin compared with pronation.
Apart from arthroscopic portals, a mini-open incision just proximal to the wrist on the ulnar aspect is often utilized for TFCC repair and reconstruction. Of particular relevance is the inside-out peri-foveal technique, where this incision is placed more distally and nearer the wrist joint. These are also close to the DBUN and places it at risk. It is recommended and usually possible to locate and protect the DBUN after incision using a soft sling, so that the passing of needles in and out of the wrist joint can proceed safely, and to prevent strangulation of the nerve within the sutures (Chen et al., 2006) (Figure 2).
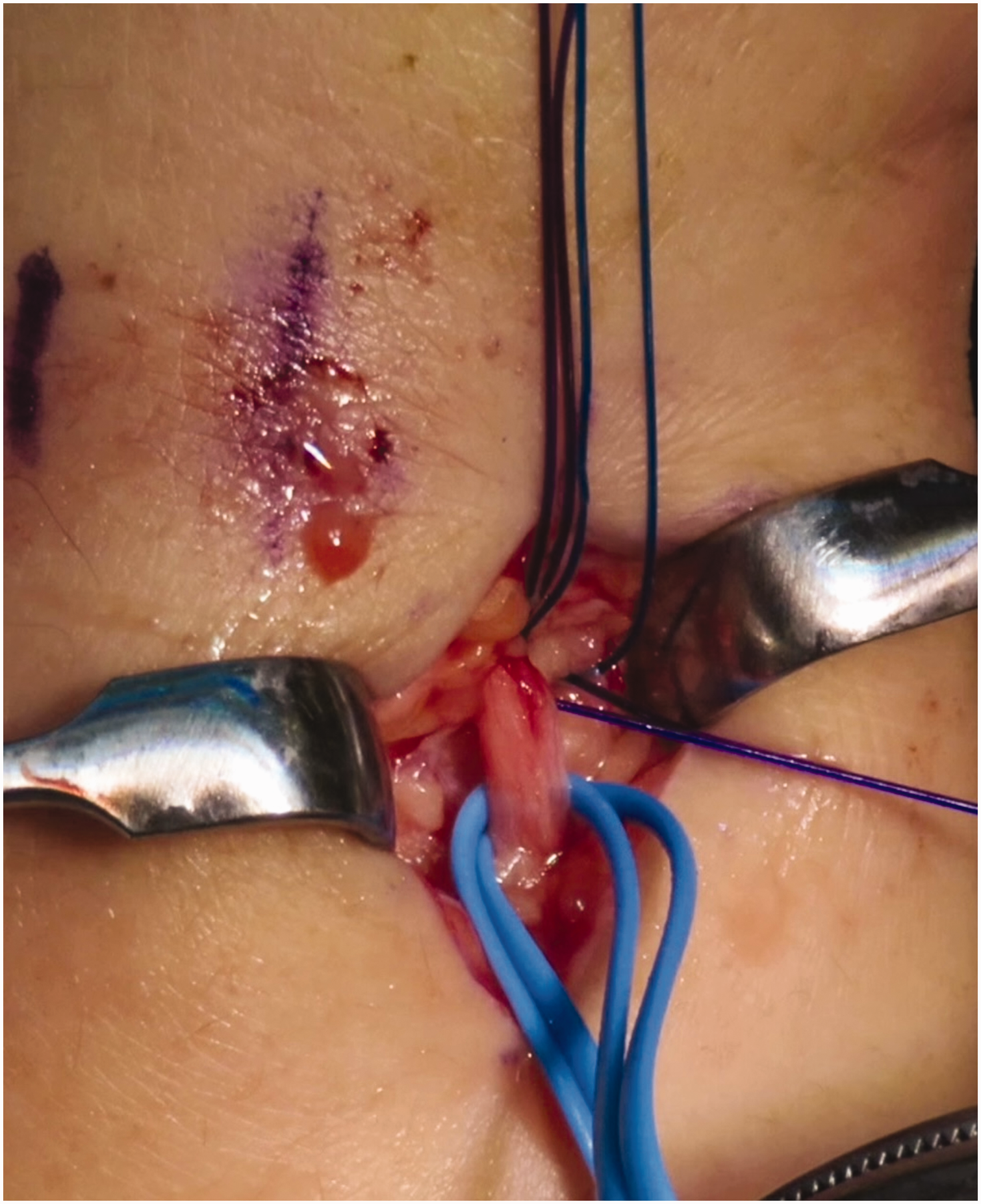
Clinical picture showing isolation of the dorsal branch of the ulnar nerve in a sling.
The diagnosis of iatrogenic DBUN injury is mainly established by the presence of numbness in its innervated territory or a portion of it, neuropathic pain such as with marked hypersensitivity, sensory disturbance in the innervated territory and positive Tinel’s sign. Vasomotor changes with dry skin and erythema are indicators of a high-grade injury with axonal disruption rather than neurapraxia. An injection test with a small dose of anaesthetic targeted superficially at the site of pain helps to confirm the diagnosis. An ultrasound scan performed by an experienced musculoskeletal radiologist may provide the status of the nerve, although the accuracy is limited for small nerve branches. The differentiation of low-grade (neurapraxia) and high-grade (transection or neuroma-in-continuity) nerve injury requires observation for up to 8 weeks, during which time conservative treatment is begun with scar physical therapy, desensitization and monitoring of response. A lack of improvement and persistent significant pain despite a period of conservative treatment may indicate one of three possibilities – of end neuromas, neuroma in continuity or scar tethered nerves (Elliot, 2014) – and require surgery for symptom relief and restoration of sensation. Wrapping the nerve stump with a piece of free muscle graft, a more recent technique termed regenerative peripheral nerve interface (RPNI), has shown to cause the nerve fibres to re-innervate the muscle forming new neuromuscular junctions and thus reduce pain (Kung et al., 2014) (Figure 3). Detailed discussion of surgical management of these conditions is beyond the scope of this review.
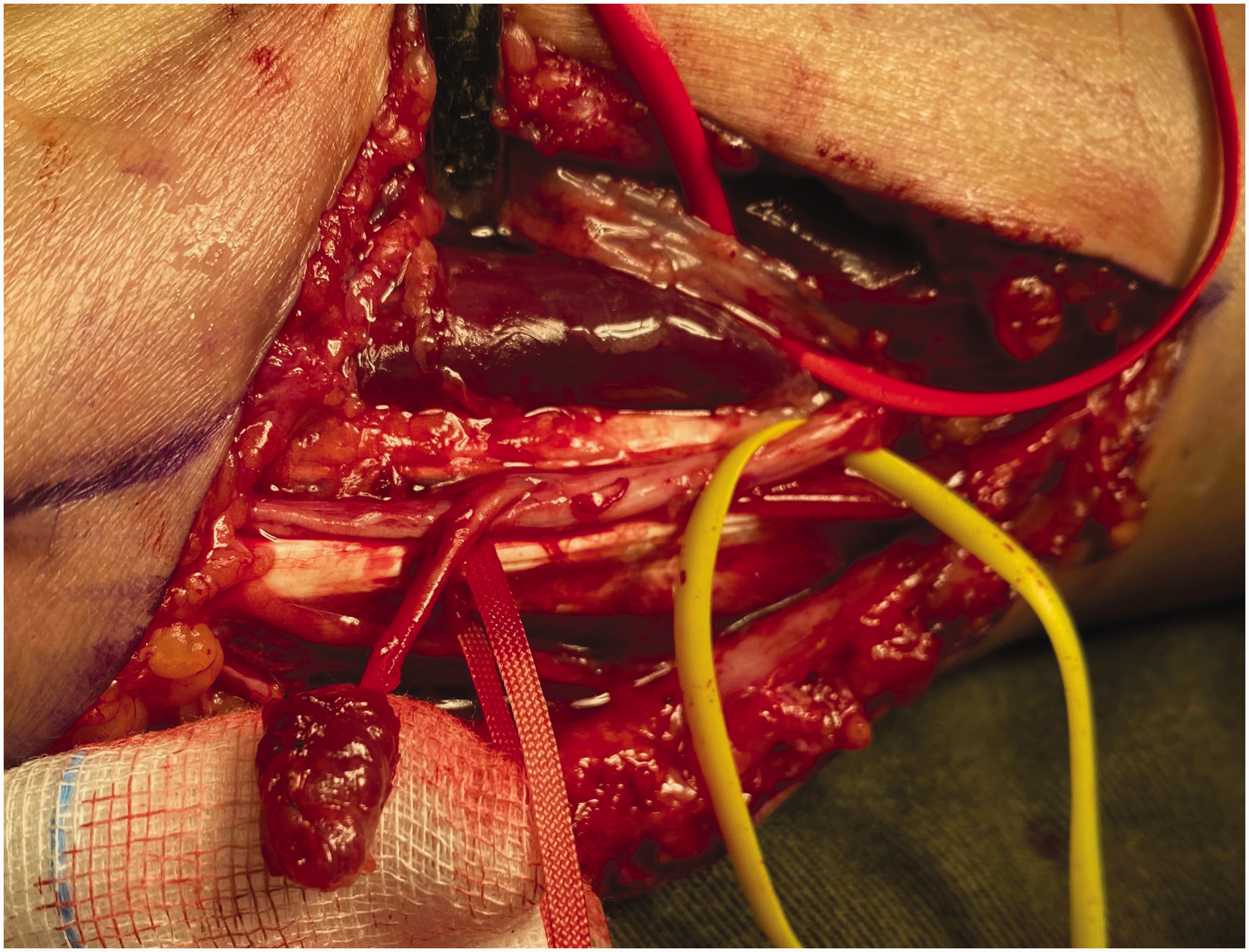
Clinical picture showing an end neuroma treated with regenerative peripheral nerve interface (RPNI).
Extensor tendon complications
ECU tendonitis and tendon injury, especially that of the extensor digiti minimi (EDM), are the two types of extensor tendon issues that may arise as a result of arthroscopic TFCC surgery. In one cadaveric study of 10 specimens, six specimens were found to have various injuries to the extensor tendons after arthroscopic TFCC repair (Shyamalan et al., 2016). Three specimens showed scuffing of the epitenon (extensor digitorum communis [EDC] to the index finger, EDC to the middle finger and ECU), two other specimens had partial lacerations to one extensor tendon each (30% of the ECU tendon through the 6U portal and 50% of the EDC to the index), and in one specimen the EDM was included in a stitch passed through the 6R portal during TFCC repair. Several measures need to be taken to reduce the chance of extensor injury. As mentioned above, accurate portal placement is necessary using direct arthroscopic visualization with needle localization. Radiofrequency ablation or shrinkage on the dorsal side has to be applied sparingly and should only be done under wet arthroscopy with adequate fluid outflow and ventilation. Performing arthroscopic surgery under portal site local anaesthesia with the patient wide awake and without the use of tourniquet further increases the safety, as assessment of active finger extension during and immediately after the surgery is possible (Ong et al., 2012), and is our routine practice.
Extensor tendon rupture from thermal damage or its propagation from a partially torn tendon usually occurs 2–3 weeks postoperatively and presents with finger drop, with patients experiencing a popping sensation. Exploration often shows a zone of attrition and scarring with a varying degree of adhesions to the extensor retinaculum. Tendon repair may be possible for narrow zone injury, but more often tendon transfer using the extensor indicis or a slip of EDC to the middle finger is the treatment of choice.
ECU tendinitis after TFCC repair was reported in up to 19% using open and arthroscopic techniques (Anderson et al., 2008). The exact cause has not been studied but may be related to ECU tendon instability after surgical trauma to the sheath, or irritation of the tendon by suture knots causing tenosynovitis. There was no significant difference in occurrence rate between open and arthroscopic methods, and among these only a small number of patients required reoperation by tenosynovectomy (Anderson et al., 2008). In surgical methods that require opening of the ECU sheath, ECU instability could be prevented by ensuring a secure repair of the sheath (Chen, 2017), and care should be taken to ensure suture knots are located away from the tendon.
Mid-term complications
Irritation from suture knots
A systematic review of TFCC transosseous repair reported that the most common complication was skin irritation from suture knot (9.16%), of which 3 out of 12 patients required reoperation for removal. Covering the knots by soft tissue, such as extensor retinaculum, and tying at areas further away from the DBUN may reduce this risk.
Wrist stiffness
Loss of motion after TFCC surgery usually affects the range of pronosupination and a permanent loss of flexion-extension is rather uncommon, as arthrofibrosis of the unaffected radiocarpal joint seldom occurs; surgical trauma should be limited to the ulnar-most aspect. Loss of pronosupination may be related to prolonged immobilization, nerve compression or scarring causing undue pain or complex regional pain syndrome (CRPS), or the repair technique itself. A loss of 45° of supination in 2 out of 90 (2%) patients was reported in one study of arthroscopic and open TFCC repair (Nakamura et al., 2011). Patient factors including motivation, pain tolerance and preoperative status may also play a part in the amount of motion that can be regained. Preoperative wrist and forearm stiffness due to the TFCC injury and pain should be optimized with appropriate therapy and mobilization regime. On the technical side, if the repair is eccentric and not at the isometric footprint, or if the repair attaches the TFCC to a wider area than the anatomical footprint, then there would be excessive tension on either the dorsal or volar distal radioulnar ligaments, or both, which would restrict rotational motion. An anatomical study recommends placement of the tunnel at the lowest point of the ulnar fovea, which although is not the centre of the footprint, correlates best with the attachment of the deep component of the TFCC (Okuda et al., 2021). A C-ring targeting drill guide can facilitate accurate placement of bone tunnel. Postoperatively, we recommend immobilization for 3 weeks, with the forearm in neutral rotation position in a Muenster cast; motion is resumed thereafter and increased gradually from mid-range to full range by 6 weeks. Nevertheless, some cases of persistent wrist stiffness still occur; therefore, longer periods of immobilization are best avoided. Passive mobilization exercises can usually be initiated by 8 weeks postoperatively, but the precise timing should be judiciously advised in order to attain a fine balance between stiffness (loss of physiological motion) and instability (excessive unphysiological motion).
If stiffness persists, and the DRUJ remains stable, manipulation under regional or local anaesthesia can be considered after 9 weeks to hasten recovery. If a permanent loss of rotation occurs in the presence of restored DRUJ congruity and stability, open DRUJ release, including the distal oblique bundle of interosseous membrane, can be performed. Otherwise, salvage procedures may be considered to achieve functional forearm motion.
Persistent or recurrent instability
Persistent DRUJ instability after arthroscopic TFCC repair may be due to factors related to the injury pattern, surgical technique and rehabilitation. One factor that was thought to contribute to poor healing is chronicity of the injury, raising the question of whether repair should be done in chronic tears. Nakamura et al. (2011) looked at 24 patients with arthroscopic repair and 66 patients with open transosseous repair and reported that in the arthroscopic group a chronicity of injury of 7 months or more led to fair and poor results, while outcomes in the open group were not affected by chronicity. In a multicentre review involving 274 patients with a mean duration of symptoms of 20 months who received open TFCC foveal repair (Feitz et al., 2021), a longer period of symptoms, higher pain and a higher functional Patient Related Wrist Evaluation (PRWE) total score at baseline were associated with poorer functional scores and increased pain. However, recent studies, especially those reporting an arthroscopic transosseous repair technique, disputed this concept and showed good outcomes regardless of the duration of injury. A systematic review of seven studies reported good outcomes in all studies with a mean preoperative duration of symptoms of 6–12.4 months (Jung et al., 2021). The study with the longest duration of preoperative symptoms among these had a mean of 11 months (range 2–60) of symptoms in 16 patients, all treated with a single tunnel arthroscopic transosseous repair. They reported no recurrence of instability at a mean postoperative follow-up of 31 months (Park et al., 2018). Finally, a single-centre study that compared outcomes between early and late repair after transosseous single-tunnel repair showed that functional outcomes were similar between repair within 6 months and beyond 12 months (Park et al., 2020). Although to date there is no clear evidence of superiority of one technique over another, one may postulate that difference in outcomes in chronic tears may be related to the surgical method.
Complications related to arthroscopic dorsal TFCC repair
Early complications
Nerve irritation and injury
Dorsal TFCC tears are located between the ECU sub-sheath and DRUJ, and are repaired via an extension of the 6R portal, which also places the DBUN at risk as it is over or at a close distance to the repair site, although the incidence of nerve injury specific to dorsal TFCC repair has not been reported.
Extensor tendon complications
The EDM, in particular, is at risk during repair due to its more recessed position directly overlying the DRUJ, which is the area of dorsal TFCC repair. In our series of TFCC repair, there was one instance where the EDM was caught within the suture loop during dorsal repair, which was identified during operation and corrected (Estrella et al., 2007). Therefore, it is prudent to actively identify and sling the EDM tendon before suture placement near the 4-5 and 6R portals after the transverse incision is made for the repair.
Complications related to TFCC reconstruction under arthroscopic assistance
Early complications
Nerve-related complications
Arthroscopic TFCC reconstruction involves the intra-articular placement of a tendon graft through small capsular windows without a formal capsulotomy, while extra-articular bone tunnelling is achieved by open approaches on both volar and dorsal aspects. Nerve-related complications were present in 3 out of 28 patients in our series following this technique (Mak and Ho, 2017). This included ulnar nerve entrapment by tendon graft at the volar ulnocarpal joint level in one patient and transient neurapraxia of the ulnar nerve in two patients due to operative traction. Ulnar nerve palsy after arthroscopic surgery warrants early surgical exploration unless the cause is purely neurapraxia beyond doubt, such as when the nerve was explored and inspected before wound closure. Early ultrasound imaging may help to detect signs of nerve injury, such as nerve swelling or even transection, but it should not be a cause to delay surgical exploration. Luchetti and Atzei (2017) reported one DBUN transient neurapraxia after arthroscopic TFCC reconstruction in a series of 11 patients. The relatively high incidences of ulnar nerve and DBUN neurapraxia need to be addressed by avoidance of vigorous traction at the distal ulnar and volar approaches used for the passing of tendon graft. In a recently reported all-inside reconstruction technique, incision at the distal ulna was not required and this may be a promising technique to reduce nerve-related complications (Atzei et al., 2023).
Fracture
In some reported techniques of TFCC repair or reconstruction, sizeable osseous tunnels in the distal ulna were used (Luchetti and Atzei, 2017; Park et al., 2018). In the latter study of TFCC reconstruction, one incidence of ulnar styloid fracture occurred during insertion of a 4 mm interference screw in the distal ulna tunnel. Breaking of a guidewire during the drilling process may also occur (Mak and Ho, 2017). Therefore, care has to be taken during this step with respect to the relative size and the direction of the tunnel in the ulna.
Others
Other complications, such as looping of tendon graft around the ulnar neck, have been reported, although rare (Luchetti and Atzei, 2017).
Mid- to long-term complications
Recurrent or persistent instability
In our series of 28 patients, recurrence of instability occurred in five patients (Mak and Ho, 2017). Of these five, four were due to graft ruptures, of which two were due to repeat injuries and the remaining one was due to graft loosening. In their series of 11 patients, Luchetti and Atzei (2017) reported one patient with re-injury and tendon graft rupture, and one with late tendon graft rupture. The reason for graft loosening was often due to failure of final fixation. In revision surgery, using an additional transverse bone tunnel proximal to the ulnar foveal tunnel for passing one limb of the graft through and tying to the other limb restores stability. Additional fixation with the use of suture anchors could be performed if the length of the graft is insufficient to tie it securely back to itself.
In patients with recurrent DRUJ instability, graft rupture should be suspected and confirmed with arthroscopy, and may require revision tendon graft reconstruction.
Scar pain
Scar pain, discomfort and hypersensitivity over the ulnar incision may occur without true paraesthesia of the DBUN, occurring in 10.5%–45.5% of patients with arthroscopic TFCC reconstruction (Atzei et al., 2023). Patients may complain of a combination of four symptoms, including spontaneous pain, pressure pain, movement pain and hypersensitivity and allodynia on light touch (Elliot, 2014). This may be due to dysfunction and neuropathy of the cutaneous nerves in the vicinity caused by perineural fibrosis, trauma from vigorous retraction and entrapment by adjacent scar tissue. Suture knots should be cut short and tied to the soft tissue as deep as possible to avoid this. Absorbable suture materials may have less chance of causing long-lasting nerve irritation. Most of these complications are self-limiting, though some patients may require neurolysis or management of neuroma.
Persistent wrist pain
Ulnar wrist pain that persists even after TFCC reconstruction requires careful assessment to determine the possible causes, including cutaneous nerve injury or scarring, residual instability, chondral injury, ulnar impaction syndrome, persistent synovitis, ECU tendinitis or DRUJ arthritis. DRUJ arthrodesis was reported by Chou et al. (2003) as a last resort in one patient with persistent pain, despite multiple surgeries with good effect.
With the refinement of techniques in diagnosis, repair and reconstruction of the TFCC, including the addition of new portals and approaches to the DRUJ, the foothold of arthroscopy in this area has become stronger. Across the spectrum of arthroscopic TFCC surgery, complication rates and the learning curve increase with increasing surgical complexity. The ulnar side of the wrist is a common site for wrist disorders but is also a delicate area in close proximity to nerves and tendons. For some of the more common complications, such as neuritis from scarring, traumatic neuroma and delayed extensor ruptures, a perfect salvage treatment is often elusive. Vigilance to anatomical details and a meticulous dissection technique can help to reduce complications that may result in disturbing pain and functional loss.
Supplemental Material
sj-pdf-1-jhs-10.1177_17531934231218608 - Supplemental material for Complications after arthroscopic triangular fibrocartilage complex (TFCC) surgery
Supplemental material, sj-pdf-1-jhs-10.1177_17531934231218608 for Complications after arthroscopic triangular fibrocartilage complex (TFCC) surgery by Michael Chu Kay Mak and Pak Cheong Ho in Journal of Hand Surgery (European Volume)
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.