
Abstract
The ReMotion wrist replacement has good short- to medium-term survival with an acceptable complication profile as we previously reported in a cohort of patients with rheumatoid arthritis. We now report the long-term results of the same cohort and details of explant analysis of revisions undertaken for aseptic loosening. A total of 16 wrists were reviewed. Seven prostheses remain in situ with no obvious signs of wear or radiological loosening at a mean follow-up of 15.5 years. Three wrists had been revised: one for infection and two for aseptic loosening. Five patients (six wrists) died 2–9 years after operation from unrelated causes. Explant analysis demonstrated relatively minor wear compared with the published results of the Universal-2 prosthesis. We hypothesize that this may be explained by differences in polyethylene sterilization and prosthetic design. The ReMotion wrist replacement has favourable long-term results in patients with rheumatoid arthritis with a 16-year survival rate of 78%–86%.
Introduction
Despite the numerous advances in medical treatment for rheumatoid arthritis (RA), surgical intervention retains a role in the management of advanced rheumatoid wrist disease (Park et al., 2021). Wrist arthrodesis was historically the preferred surgical technique, sacrificing joint movement for pain relief. Total wrist arthroplasty (TWA) offers an alternative with the advantage of preserving movement and quality of life (Zhu et al., 2021). There is, however, a lack of long-term TWA survivorship data, which can make it difficult to counsel patients.
The ReMotion TWA (Stryker Corp., Kalamazoo, MI, USA) is a fourth-generation uncemented wrist arthroplasty with three main components: a cobalt chromium (CoCr) radial component with a highly polished articulating surface and a stem coated with titanium (Ti) to facilitate bone ingrowth, and a polished CoCr carpal plate with a Ti coated capitate peg, which is secured with two Ti carpal screws. Articulation occurs between an ellipsoidal mobile bearing ultra-high molecular weight polyethylene (UHMWPE) insert and the radial component. Its design aims to maintain stability by preserving bone, ligamentous and soft tissue attachments (Zijlker et al., 2022).
Several studies have evaluated the short- and medium-term results for the ReMotion TWA, including a series from our unit in rheumatoid patients (Bidwai et al., 2013; Zijlker et al., 2022). However, long-term data are lacking.
The aim of the present study was to review the long-term survivorship of the ReMotion TWA in our institution and to combine this with explant analysis.
Methods
This study used the original cohort of patients from our unit (Bidwai et al., 2013) and a further three patients operated on in the same period who were not identified in the original study. In total, 16 wrists in 14 patients who underwent ReMotion TWA between 2004 and 2010 by a single surgeon (DB) were identified. The indications for TWA surgery were painful pan-carpal RA without severe bone loss, carpal subluxation or previous infection. Patients had been appropriately counselled and were given the choice of TWA as an alternative to arthrodesis.
The surgical technique was based on the manufacturer’s recommendation and is documented in the original series (Bidwai et al., 2013). Postoperatively, patients were placed in an anterior plaster splint in slight extension. One week postoperatively, patients started rehabilitation with a gentle range of movement supervised by a hand therapist and were fitted with a custom resting wrist orthosis in slight extension for 2 months. All patients were advised against heavy lifting and manual labour for their lifetime.
Patients were invited to a specifically created clinic for annual radiological and clinical assessment, which was run by the unit’s occupational hand therapist. If patients were unable to attend, case notes were reviewed, radiographs were obtained remotely, and a telephone consultation undertaken.
Survival was determined according to both the Kaplan–Meier method, in which the end point was revision or removal of components, and by using a competing incidence analysis (Wongworawat et al., 2015), in which late revision for aseptic loosening was the end point.
When revision surgery was carried out for aseptic loosening, explants were sent for analysis at a specialist university biomedical engineering laboratory. The components were visually analysed at the macroscale and examined at the microscale using a Quickscope (Mitutoyo, Kawasaki, Japan), a non-contact vision measuring system, at 25× magnification. Using a Zygo Newview 5000 (Zygo Corp., Middlefield, CT, USA) non-contacting profilometer (with a sensitivity of 0.001 µm for surface roughness [Sa]) (Scholes et al., 2017)), the surfaces of the radial and carpal plates and the insert were examined at the nanoscale. In total, 20 Sa and skewness (Ssk) measurements were taken from each surface.
The study protocol was registered with our institutional research department as a service assessment and a Medical Research Council/Health Research Authority online test confirmed that formal ethical approval was not required.
Results
In total, 14 patients had 16 ReMotion TWAs implanted between 2004 and 2010. Of them, 11 patients were women and the mean age at surgery was 57 years (range 26–76). The case details are summarized in Table 1. Short- and medium-term clinical outcomes were reported in our previous article (Bidwai et al., 2013) and this report is focused on long-term survivorship. There were three significant short-term complications, reported in the original series, that included two significant wound problems (in cases 3 and 4), which, although affecting short-term outcome did not affect long-term outcomes, and a peri-prosthetic infection (case 16) treated by a two-stage revision to arthrodesis, 3 years after the primary operation. There were two cases of late aseptic loosening that were successfully revised to Motec TWAs (Swemac Innovations LLB, Linköping, Sweden) 11 (case 15) and 16 (case 1) years postoperatively. The demographics, postoperative radiographs and medium-term outcome of the two patients with aseptic loosening were unremarkable when compared with the others. Illustrative radiographs of the three revision cases are shown in Figure 1. Five patients (six wrists) died of unrelated causes 2–9 years postoperatively; they were all under annual review and none had evidence of aseptic loosening or other implant-related complication. This number of deaths is to be expected considering the age and the life expectancy of patients with RA in northwest England.
Case details of the series of ReMotion TWAs.
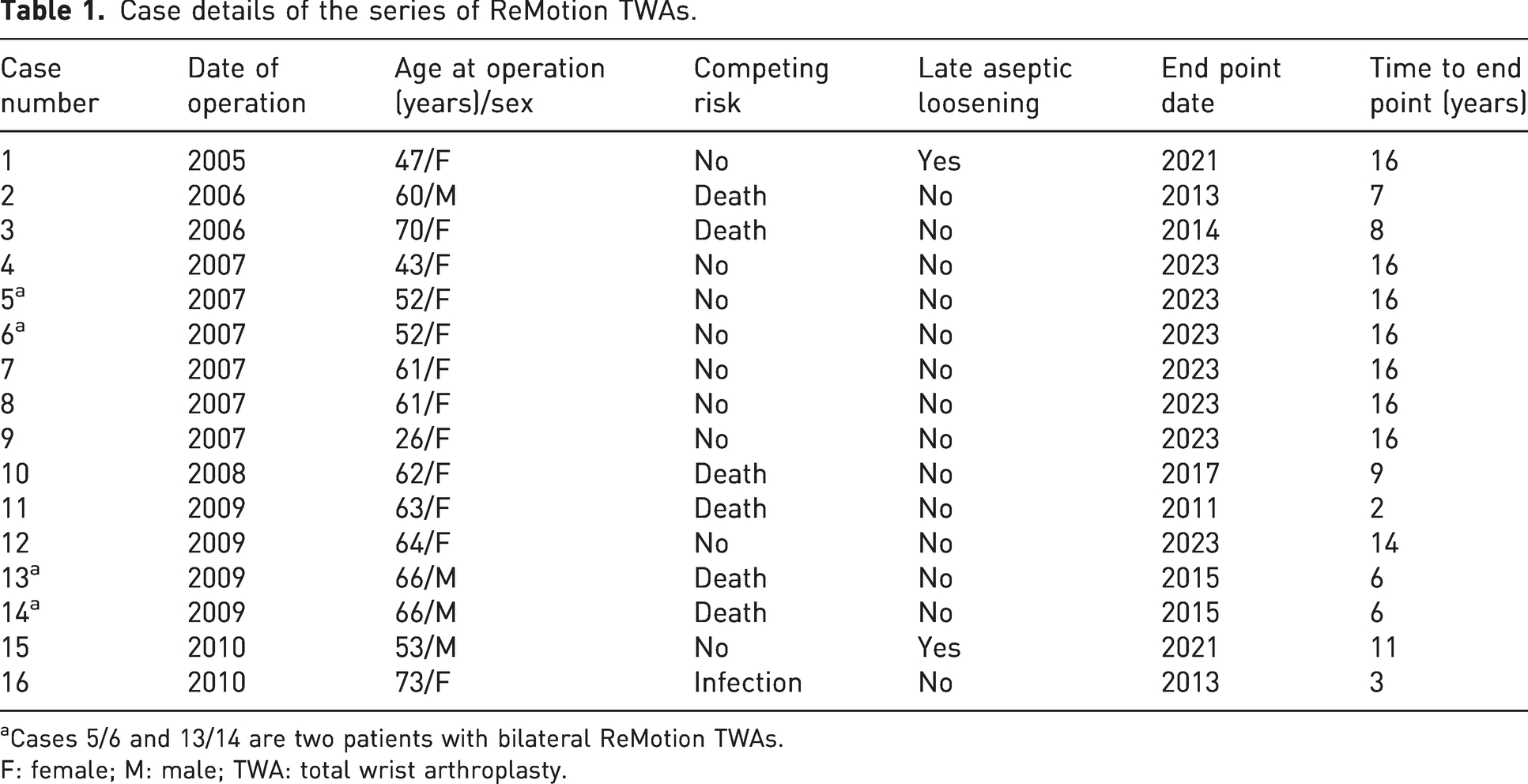
Cases 5/6 and 13/14 are two patients with bilateral ReMotion TWAs.
F: female; M: male; TWA: total wrist arthroplasty.

Radiographs of the three cases of that required revision. (a, b) Immediate initial postoperative PA and lateral radiographs of case 1 and (c, d) pre-revision showing aseptic loosening. (e, f) Pre-revision PA and lateral radiographs of case 15 showing aseptic loosening and (g, h) after revision to Motec TWA. (i, j) Pre-revision radiographs showing infected loosening of case 16. PA: posteroanterior; TWA: total wrist arthroplasty.
Seven TWAs remain in situ; all have been recently reviewed, at a follow-up of 14–16 years postoperatively, with no obvious signs of wear or loosening. The Kaplan–Meier survival curve is shown in Figure 2(a) and the cumulative survival based upon competing incidence analysis is shown in Figure 2(b), both with 95% confidence intervals (CI). The Kaplan–Meier survival is estimated at 86% at 16 years (95% CI: 42 to 98) and the cumulative survival is estimated at 78% at 16 years (95% CI: 50 to 90).
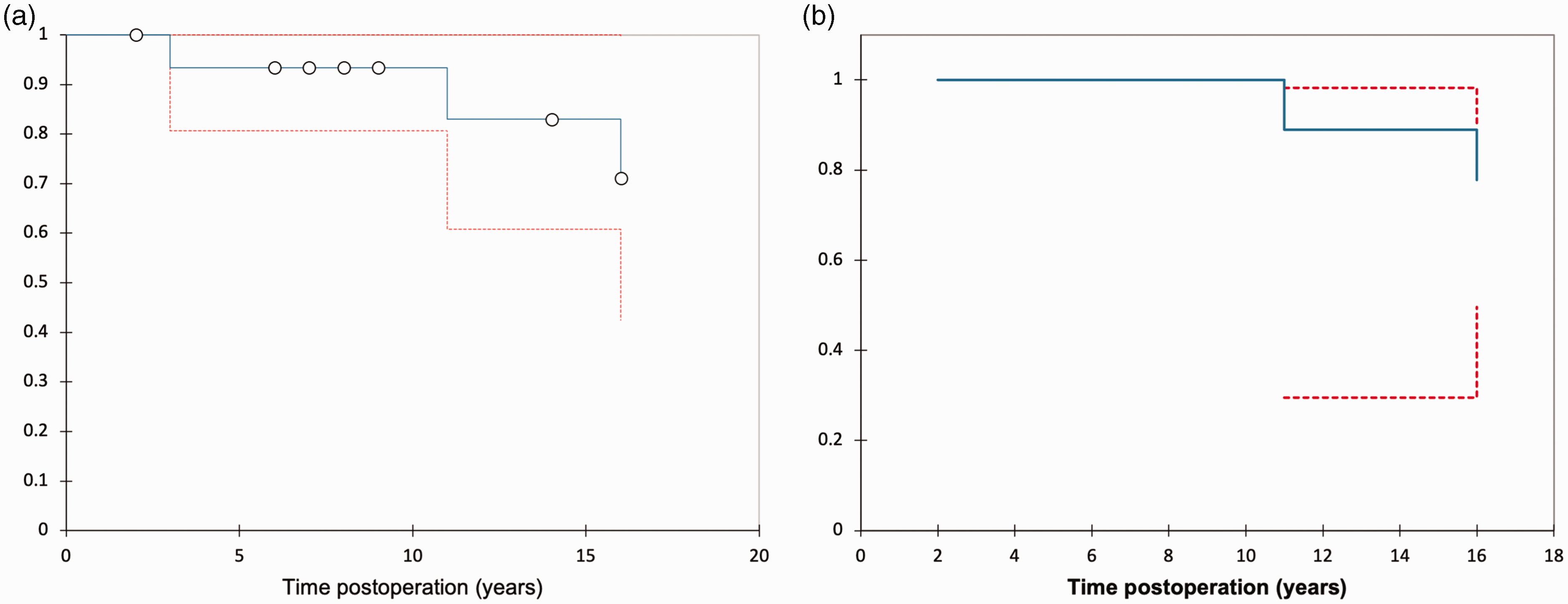
(a) Kaplan–Meier survival curve for ReMotion wrist replacement and (b) Competing Incidence Analysis based survival curve. Dotted lines indicate 95% confidence intervals; circles indicate the index events, revision and death.
The implant removed for infection was not analysed. The two implants revised for aseptic loosening are shown in Figures 3 and 4. Neither specimen showed major or catastrophic wear; however, both explants showed multidirectional scratches on the articulating surface of the radial plate and concentric scratches on the carpal plate. There were also concentric scratches observed on the backside of the polyethylene insert (Figures 3(b) and 4(b)). Although no significant macroscopic damage was seen on the articulating surface of the polyethylene inserts, both had slight damage to the rim and one showed some discolouration. Compared with unworn surfaces, both explants displayed increased surface roughness on the backside of the polyethylene insert. All analysed surfaces had negative skewness, suggesting removal of material (Table 2).
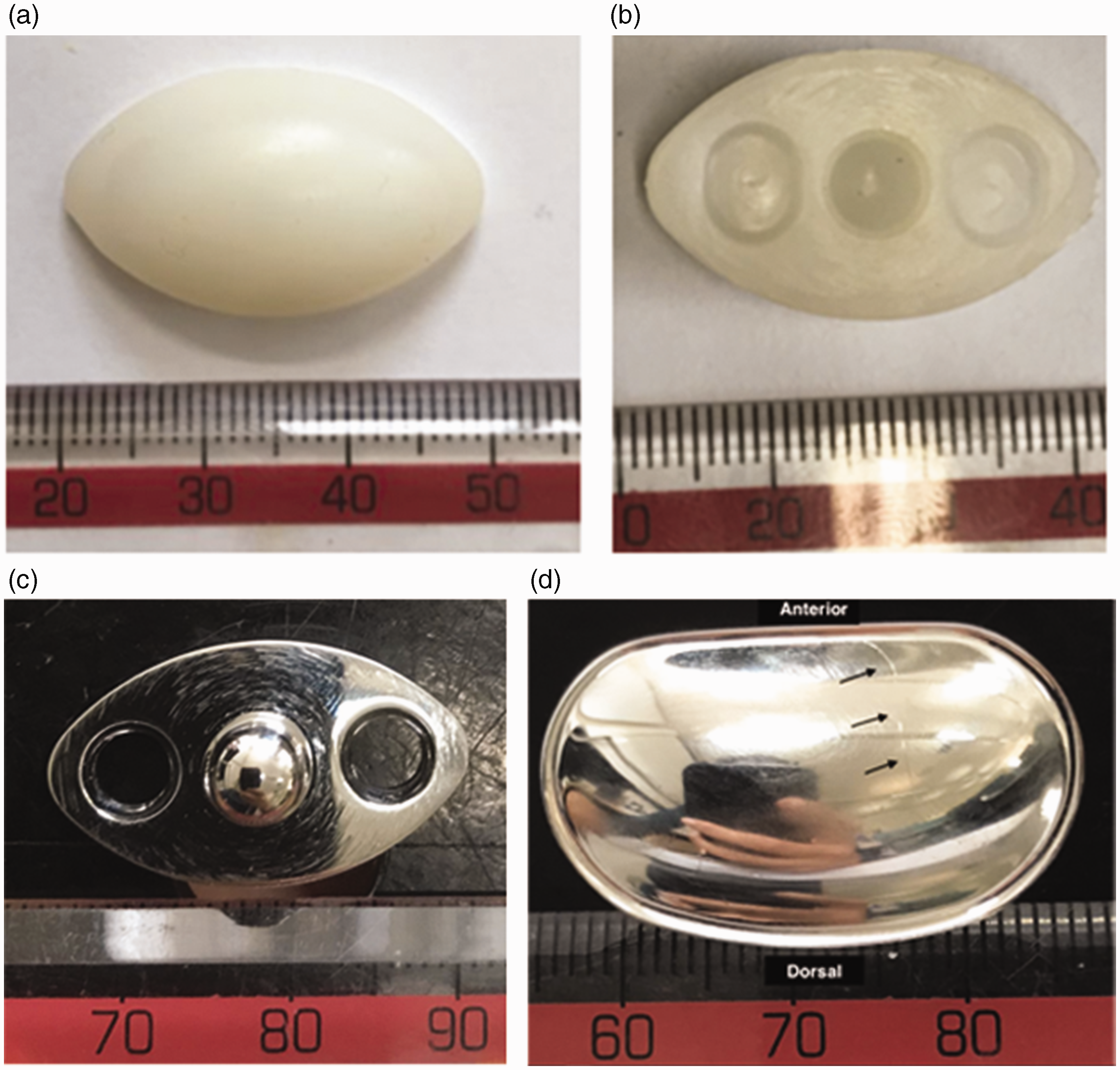
Explants from case 1 after revision for aseptic loosening. (a) Articulating surface of polyethylene insert, with no significant damage. (b) Back of polyethylene insert, with concentric scratches and minor rim damage on right hand edge. (c) Front polished surface of carpal plate showing concentric wear damage and (d) Articular surface of radial implant. The obvious scratch on the radial surface, marked with black arrows, was caused during explantation.
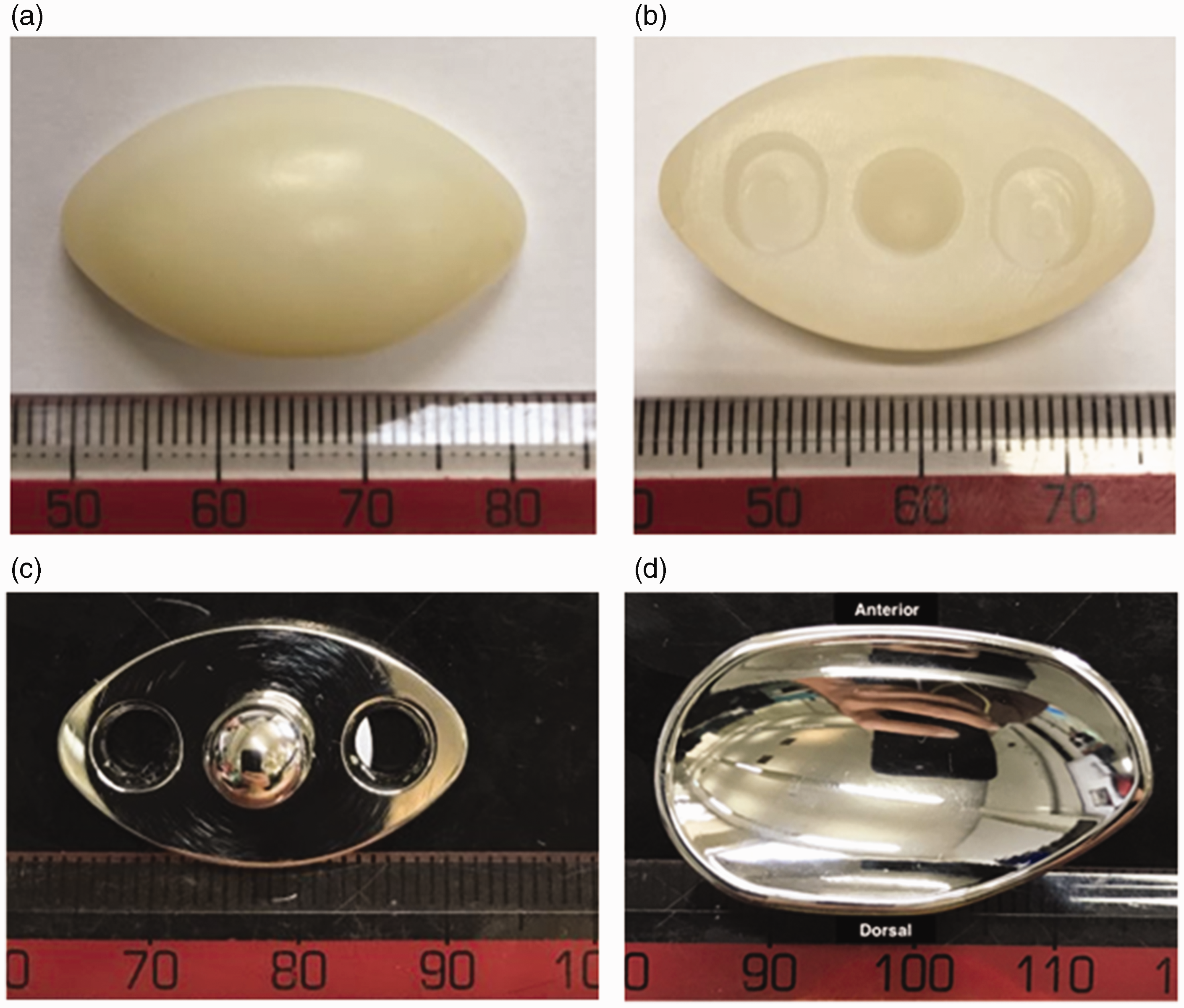
Explants from case 15 after revision for aseptic loosening. (a) Articulating surface of polyethylene insert, with no significant damage. It appears shiny. (b) Back of polyethylene insert, with minor rim damage on left hand edge. (c) Front polished surface of carpal plate showing concentric wear damage and (d) Articular surface of radial implant.
The mean roughness data collected from the components of the explanted ReMotion wrists.
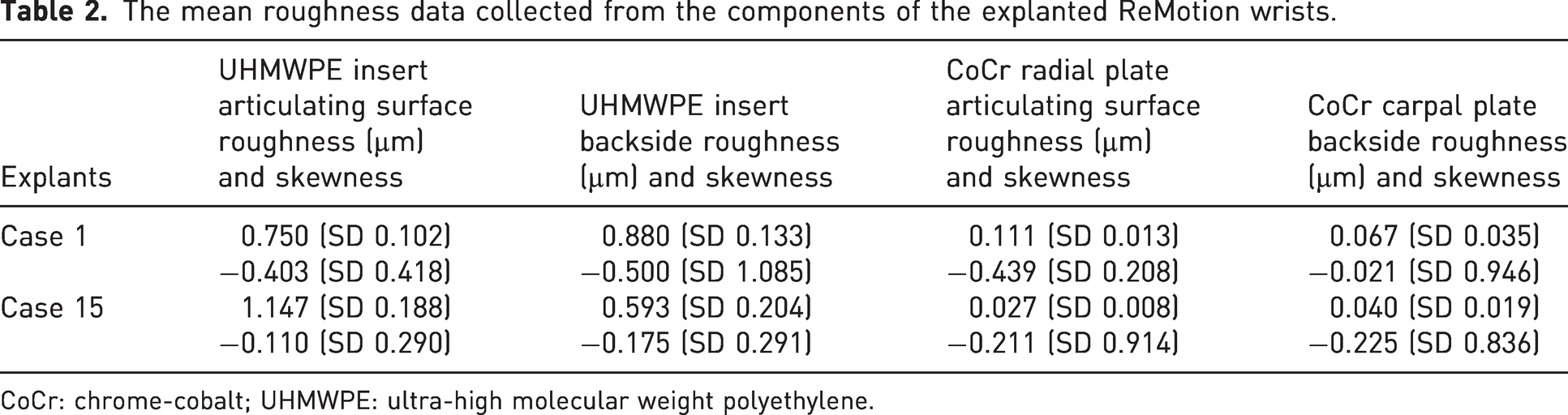
CoCr: chrome-cobalt; UHMWPE: ultra-high molecular weight polyethylene.
Discussion
To our knowledge, this is the longest follow-up for the ReMotion prosthesis to date. The 16-year Kaplan–Meier survivorship of the TWA for RA was 86% (95% CI: 42 to 98). Although we acknowledge that the dataset is relatively small, it is complete and is the only published series that includes explant analysis. The small dataset does, however, mean that the 95% CIs for survivorship are wide and probably overestimate the long-term survival of the implant, as we do not know the long-term outcome of the six implants in patients who died of unrelated causes. It is for this reason that competing incidence analysis based survival is more appropriate in longer-term survival studies, in which the effect of events such as death and unrelated implant failure, such as for infection, are accounted for when assessing long-term failure for aseptic loosening (Wongworawat et al., 2015). Calculated in this way, the 16-year survival is estimated to be 78%.
Honecker et al. (2019) reported the medium-term outcomes for ReMotion TWA. In total, 23 ReMotion TWAs were included in their series, of which 19 patients had RA. Their 10-year survival was 69% with a mean follow-up of 6 years (range 1–10). Our series reports a superior survivorship with over double the length of mean follow-up.
Where revision for aseptic loosening was required, the ReMotion was revised to a Motec TWA. The senior clinical author uses the ReMotion for cases of inflammatory arthritis, particularly where there is preoperative deformity at the wrist or metacarpophalangeal joints, and the Motec for other forms of arthritis and for revisions. The wide variety of fixation options with the Motec prosthesis make it suitable for dealing with the bone loss found in revision surgery. There can, however, be issues with its use in inflammatory arthritis as there is evidence that the unconstrained nature of the ball-and-socket articulation of the Motec exaggerates any pre-existing deformity (Redfern et al., 2023) often seen in RA.
Explant analysis has not previously been reported for the ReMotion TWA and it offers an interesting insight into the reasons behind its in vivo performance. Although this is not a direct comparative study, a recent medium- and long-term follow-up study for the Universal-2 TWA (Integra Life Sciences, Plainsboro, NJ, USA) (Newton et al., 2023) has shown catastrophic polyethylene wear, which did not occur in our series. We hypothesize that this may be due to differences between the two implants in prosthesis design or specific methods of polyethylene sterilization, or both.
The ReMotion prosthesis, like the Universal-2 TWA, is designed to mimic the anatomy of the radiocarpal rather than the midcarpal joints to facilitate flexion/extension and radial/ulnar deviation. However, there are many studies that have shown that most functional movements in the normal wrist occur in an oblique plane, between 30° and 45° to the coronal planes; this movement from radial extension to ulnar flexion is known as the dart throwers’ motion (DTM) (Moritomo et al., 2007). To achieve the DTM, a relatively small amount of ‘out-of-plane’ radiocarpal movement aligns the capitate/middle metacarpal axis with the DTM plane and from here most of the movement occurs in the midcarpal joint (Werner et al., 2004). To mimic the DTM, it is likely that after TWA with implants that do not have a midcarpal joint, the wrist will attempt to rotate at the articulation to allow the capitate/middle metacarpal to align with the DTM plane. This could possibly explain why the ReMotion, with the polyethylene ellipsoidal insert that has the inherent ability to rotate against the base plate, shows less wear than the Universal-2, in which the fixed base plate may cause shear forces across the polyethylene. Our explant analysis found clear macroscopic concentric scratching on the backside of the polyethylene insert and on the polished carpal baseplate (Figures 3(b), 3(c), 4(b), 4(c)), confirming motion is taking place at this interface. Although we did not find any evidence of catastrophic wear, the negative skewness on the backside of the polyethylene confirms that this movement generates microscopic particles that may contribute to aseptic loosening via the wear cascade and may explain the osteolysis that was seen around the implanted components before revision.
The ReMotion polyethylene insert has always been manufactured and sterilized in an inert gas, thereby improving wear characteristics and reducing the risk of catastrophic delamination. The Universal-2 was manufactured and sterilized with gamma radiation in the presence of air. Free radicals produced during the irradiation process in air cause oxidation within the polymeric component, which, in turn, results in an increase in wear (Bracco et al., 2017). This difference in sterilization technique may explain why delamination and catastrophic polyethylene wear was seen in the Universal-2 and not in our ReMotion series.
In conclusion, the ReMotion TWA shows good long-term survival in patients with RA with no catastrophic wear on explant analysis. Our findings support the continued use of the ReMotion TWA in this select group of patients who have undergone appropriate counselling.
Footnotes
Declaration of conflicting interests
The authors disclosed the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The senior clinical author (DJB) has a paid consultancy role with Swemac, a manufacturer of an alternative wrist replacement. He receives no royalties for the use of any wrist replacements.
Funding
The authors received no financial support for the research, authorship, and/or publications of this article.
Ethical approval
This project has been registered with departmental research committee who felt that as it is a service evaluation, formal ethical approval is not required.
Informed consent
There is no patient identifiable information or images within this submission and as a result informed consent has not been obtained.