
Abstract
The presentation, management and outcomes of brachial plexus injuries are likely to be subject to regional differences across the globe. A comprehensive literature search was performed to identify relevant articles related to spinal accessory to suprascapular, intercostal to musculocutaneous, and ulnar and/or median nerve fascicle to biceps and/or brachialis motor branch nerve transfers for treatment of brachial plexus injuries. A total of 6007 individual brachial plexus injuries were described with a mean follow-up of 38 months. The specific indication for accessory to suprascapular and intercostal to musculocutaneous transfers were considerably different among regions (e.g. upper plexus vs. pan-plexal), while uniform for fascicular transfer for elbow flexion (e.g. upper plexus +/− C7). Similarly, functional recovery was highly variable for accessory to suprascapular and intercostal to musculocutaneous transfers, while British Medical Research Council grade ≥3 strength after fascicular transfer for elbow flexion was frequently obtained. Overall, differences in outcomes seem to be inherent to the specific transfer being utilized.
Introduction
Disability after traumatic brachial plexus injury (BPI) has increased with improved trauma survival, particularly in lower sociodemographic index regions (GBD Diseases and Injuries Collaborators, 2020). The effect on upper extremity function has a devastating physical and socioeconomic impact on patients, their vocations and their quality of life (Estrella et al., 2021). BPI remains a complex reconstructive challenge worldwide. The specific management strategy and extent of recovery is subject to a number of regional differences and influences due in part to differences in energy and mechanisms of injury, patient factors (age, BMI, co-morbid conditions), timing of presentation and subsequent surgical delay, medical resource availability, surgeon preferences and insurance variations.
Some large epidemiologic studies of traumatic BPI limited to institutional/regional experiences have been mistakenly extrapolated to global management and expected outcomes (Faglioni et al., 2014; Jain et al., 2012; Midha, 1997). Nerve transfers have gained significant popularity in recent decades and are considered an integral part of nerve injury management. A multitude of transfers have been described for BPI, and their varied outcomes have been reported from authors and institutions across the world.
Global differences in patient populations and reconstructive preferences with respect to injury pattern, energy and severity are not reported in the literature, although are hypothesized to exist based on a recent publication (Shin et al., 2022). The purpose of this systematic review and meta-analysis is to evaluate potential variations in three frequently performed nerve transfers used to treat BPI and determine regional differences in patient characteristics, injury patterns and functional outcomes.
Methods
A comprehensive literature search was performed to identify relevant nerve transfers for restoration of shoulder and elbow motion after traumatic BPI (Figure 1). Frequently reported nerve transfers included spinal accessory to suprascapular nerve (SAN-SSN) transfer, intercostal motor nerves to the musculocutaneous nerve or biceps motor branch of the musculocutaneous nerve (ICN-MCN) transfer, and ulnar and/or median nerve fascicles to biceps and/or brachialis motor branches (fascicular transfer for elbow flexion) transfer. Three electronic databases (PubMed, Embase, Web of Science) were queried from their inception through to November 2021. Guidelines as detailed in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement were followed (Moher et al., 2010).
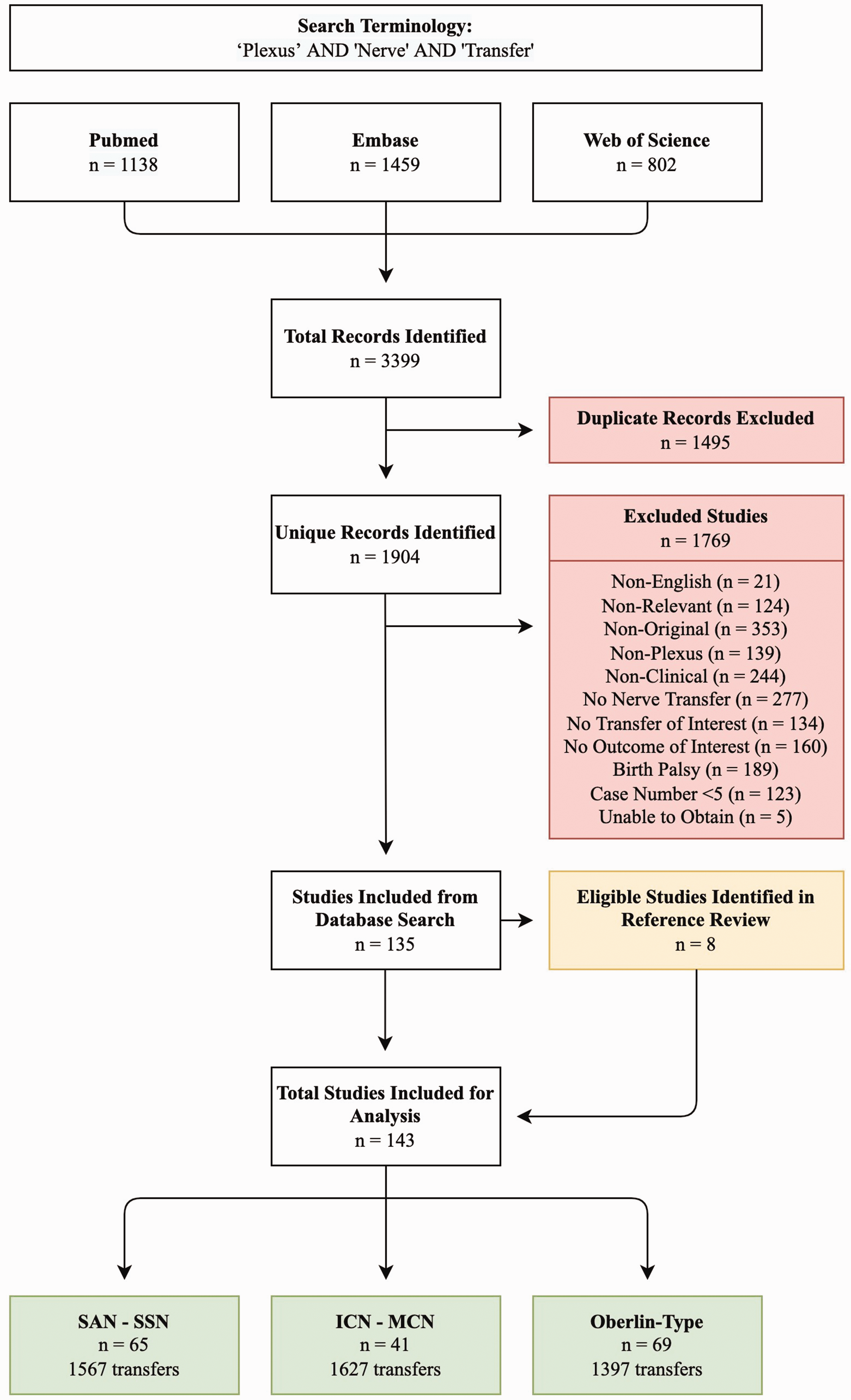
Article selection and study design. A total of 1904 unique articles were available for review. After applying the inclusion and exclusion criteria, 143 articles comprising 4591 individual nerve transfers were selected for analysis.
Exclusion criteria
Duplicate articles were identified and omitted without further review. All articles were then manually sorted and their abstracts screened for exclusion criteria. Non-relevant studies were removed. Full-text review was then performed of all remaining articles. Non-original articles (e.g. reviews, letters and abstract-only publications), non-clinical studies (e.g. cadaver, animal, in vitro models), those that did not describe BPI, surgical management, relevant nerve transfers or include a discernable outcome after nerve transfer were excluded. Articles studying obstetrical brachial plexus injuries, case reports and low-volume case series (n = <5) were also excluded. A cross-reference bibliographic check was performed to ensure completeness of the review, and identified articles were retroactively added for analysis.
A total of 3399 articles were identified on initial database query. After exclusion of duplicate records, 1904 articles were available for evaluation. Full-text review was conducted for 487 articles. Only five articles were unable to be obtained for full-text review. After applying the exclusion criteria, 135 articles remained. A review of both included manuscripts and non-original article references identified an additional eight unique articles. A total of 143 articles were included in the final analysis (Table S1).
Variables of interest
For all studies, the number of patients sustaining BPI, mean age, sex, surgical delay and follow-up were recorded. Associated injuries and BMI were infrequently described and not included in the analysis. The mechanism of injury, level (i.e. involvement of specific nerve roots) and severity of injury (i.e. pre- vs. postganglionic injury) were determined specifically for patients undergoing a given transfer. Concomitant injuries (vascular, neurologic and orthopaedic) were surveyed during the review, but were not reported with a frequency that allowed for meta-analysis. The method of determining pre-ganglionic injury was highly variable (clinical examination, radiographic imaging, intraoperative evaluation) and relied on what was reported.
For SAN-SSN transfers, the surgical approach to the spinal accessory nerve (anterior vs. posterior) and concomitant nerve reinnervation via grafting from an intact root or nerve transfer for axillary nerve function was recorded when documented. Recovery of external rotation was evaluated to assess the outcome from suprascapular nerve reinnervation without confounding contribution from axillary reinnervation. For ICN-MCN transfers, the number of intercostal nerves utilized and use of an interposition graft was recorded. For fascicular transfers for elbow flexion, the specific donor fascicle(s) and recipient nerve were recorded when specified. For both ICN-MCN and fascicular transfers, recovery of elbow flexion was evaluated to assess the outcome of the musculocutaneous nerve reinnervation.
Outcomes of interest included active range of motion (AROM) and British Medical Research Council (BMRC) grades (Table S2). AROM was analysed based on total arc of motion for the shoulder, but not for elbow motion as this was considered less clinically relevant. A number of modifications of the BMRC were used and details regarding the modifications were not always provided. Averages of outcomes were recorded when provided, or tabulated and calculated when individually available. Weighted averages (mean) of BMRC scores and AROM were then calculated globally, regionally and nationally, based on study outcome and sample size. The country of origin was determined for each study and categorized by World Bank region (Table S3) as utilized in the Global Burden of Disease Study (GBD Diseases and Injuries Collaborators, 2020; Mitra et al., 2021).
Pearson’s chi-square test was used to compare differences in patient populations and frequency of recovery. A p-value ≤0.05 was considered statistically significant.
Results
Of the 143 unique articles included in the final analysis, 6007 brachial plexus or related peripheral nerve injuries were reported. Study publication rates increased over time for all transfers (Figure S1). A mean age of 28 years and male-to-female ratio of 10:1 were observed globally. The mean surgical delay was 6 months and the follow-up was 38 months for included studies. The mechanism of injury was most frequently motorcycle accidents (29%, n = 1746) and motor vehicle collisions (8%, n = 473), but was often not reported. The extent and pattern of injury was adequately reported in 4050 (67%) patients (Figure S2). Discrete functional outcomes were described for 4591 relevant transfers in 4214 patients who sustained traumatic BPI. BMRC was reported as a binary outcome (e.g. BMRC ≥3 or ≥4) in 40 studies, an average in three studies and individually (e.g. BMRC 1–5) in 107 studies. There was tremendous variation in the reporting of motor strength depending on the nerve transfer performed (Figure S3). Similarly, shoulder AROM after SAN-SSN transfer was reported inconsistently (Figure S4).
Spinal accessory nerve to suprascapular nerve transfer
Spinal accessory nerve to suprascapular nerve transfer was the focus of 65 articles, totalling 1567 individual nerve transfers with a mean follow-up of 34 months (Tables 1 and S4). The mechanism of injury was most commonly motorcycle accidents (n = 374, 68%), with the lowest rate being observed in North America (n = 13, 16%). The proportion of upper root (C5-C6) injury was highest in South Asia (72%) and lowest in North America (22%) (Figure S5). Pan-plexal BPI were reported with the highest frequency in Latin America (63%) and East Asia (47%).
Patient and injury characteristics for SAN-SSN transfer by World Bank region (65 articles comprising 1567 individual SAN-SSN transfers were included in the analysis).
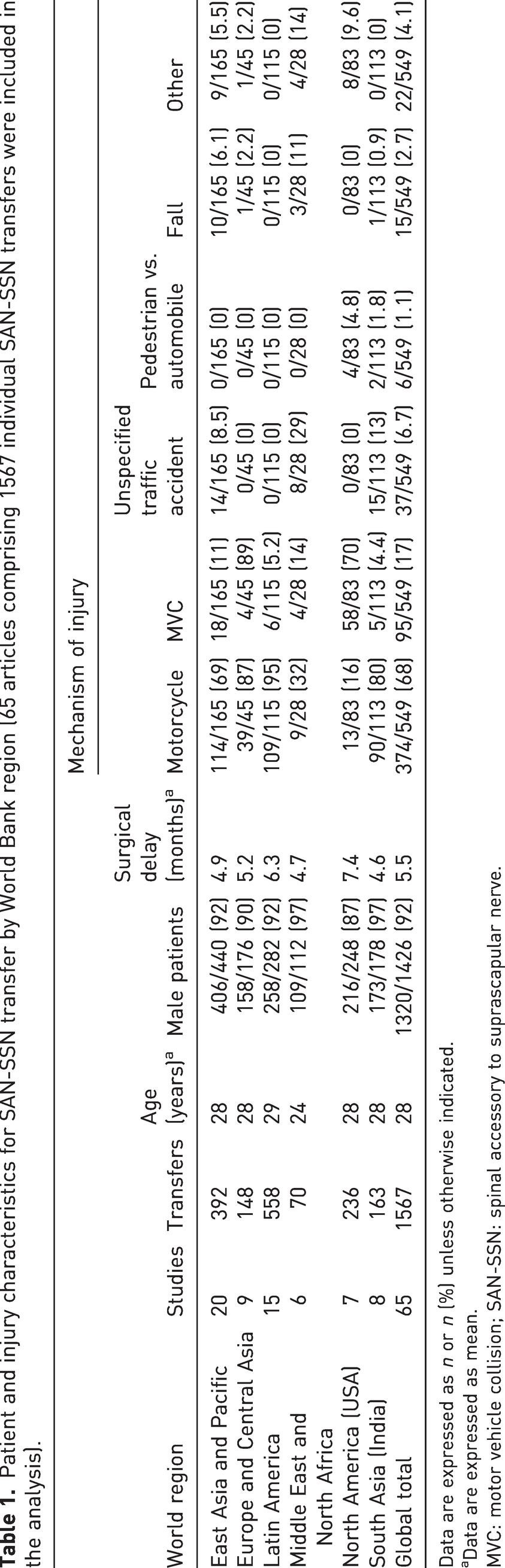
Data are expressed as n or n (%) unless otherwise indicated.
Data are expressed as mean.
MVC: motor vehicle collision; SAN-SSN: spinal accessory to suprascapular nerve.
Concomitant axillary nerve reinnervation, by nerve grafting from an intact cervical spinal root or distal nerve transfer, was performed in approximately one-third of cases worldwide (n = 564, 36%) (Table S5). When specified, an anterior approach to the spinal accessory nerve was most frequently performed.
The global weighted average for external rotation BMRC strength after SAN-SSN transfer was 2.5, although strength outcomes were highly variable by individual study and region (Figure 2(a)). External rotation of at least BMRC grade 3 and 4 strength was attained globally in 65% and 39% of patients, respectively. Higher rates of BRMC grade 3 and 4 recovery were observed in Europe compared to all other regions with available data (p < 0.05) with the exception of grade 3 recovery in East Asia (86% vs. 75%, p = 0.22) (Figure 2(b)).
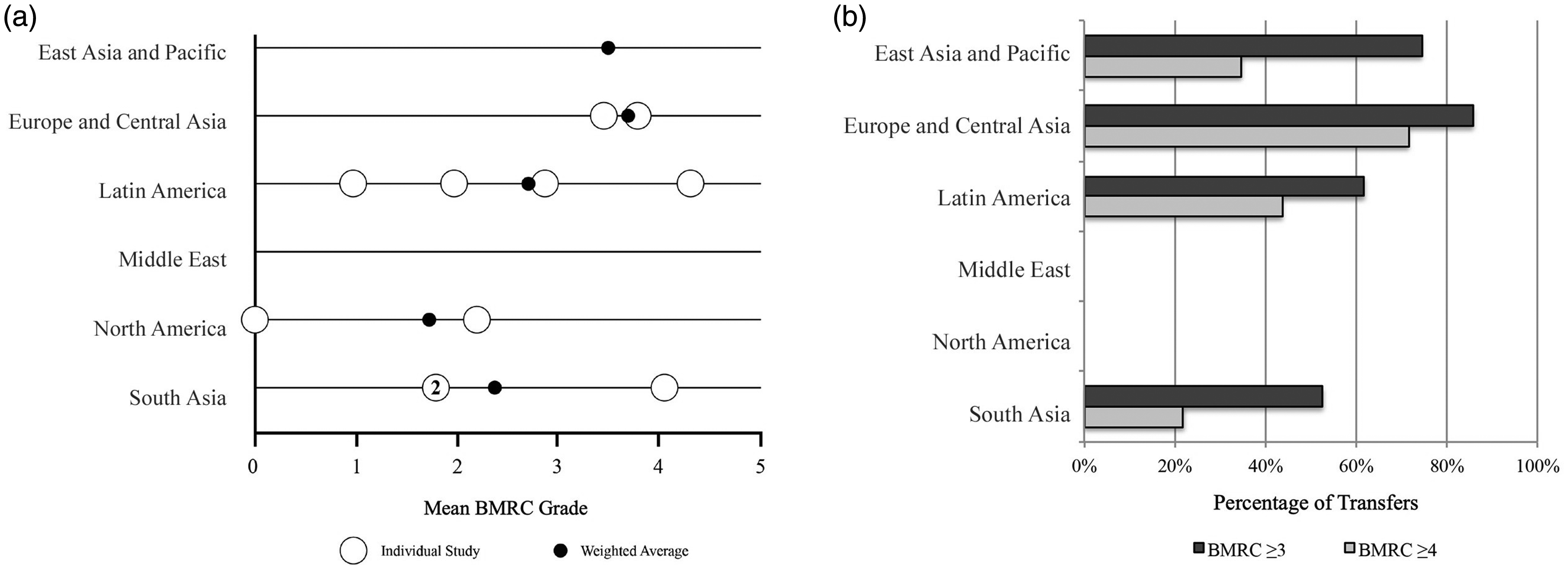
(a) Weighted average BMRC strength for external rotation after SAN-SSN transfer. Individual study outcomes (white) and weighted averages by region (black) are shown. No outcomes were available from studies originating in the Middle East and (b) Percentage recovery of external rotation strength after SAN-SSN transfer. Proportion of patients obtaining at least BMRC strength 3 (dark grey) and 4 (light grey) are shown. No outcomes were available from studies originating in the Middle East or North America.
The worldwide weighted average external rotation AROM (total arc of motion) after SAN-SSN transfer was 43° (Figure S6). AROM >30° was obtained in 65% of patients globally, while >90° was only achieved in 14%. The proportion of patients obtaining >30° of motion was not significantly different between regions (p = 0.91) (Figure S7).
Intercostal nerve(s) to musculocutaneous nerve transfer
Intercostal nerve transfer for reinnervation of the musculocutaneous nerve or its motor branches was the focus of 41 studies comprising 1627 individual nerve transfers with a mean follow-up of 37 months (Tables 2 and S6). The cause of injury was most commonly motorcycle accidents (n = 243, 72%). The majority of injuries treated by ICN-MCN transfer were pan-plexal (Figure S8). The majority of ICN-MCN transfers were performed using three intercostal nerves (n = 876, 54%) and with few requiring interposition grafts (n = 45, 3%) (Table S5). The musculocutaneous nerve proximal to the biceps branch was the target recipient nerve in most cases (n = 1460, 90%).
Patient and injury characteristics for ICN-MCN transfer by World Bank region (41 articles comprising 1627 individual ICN-MCN transfers were included in the analysis).
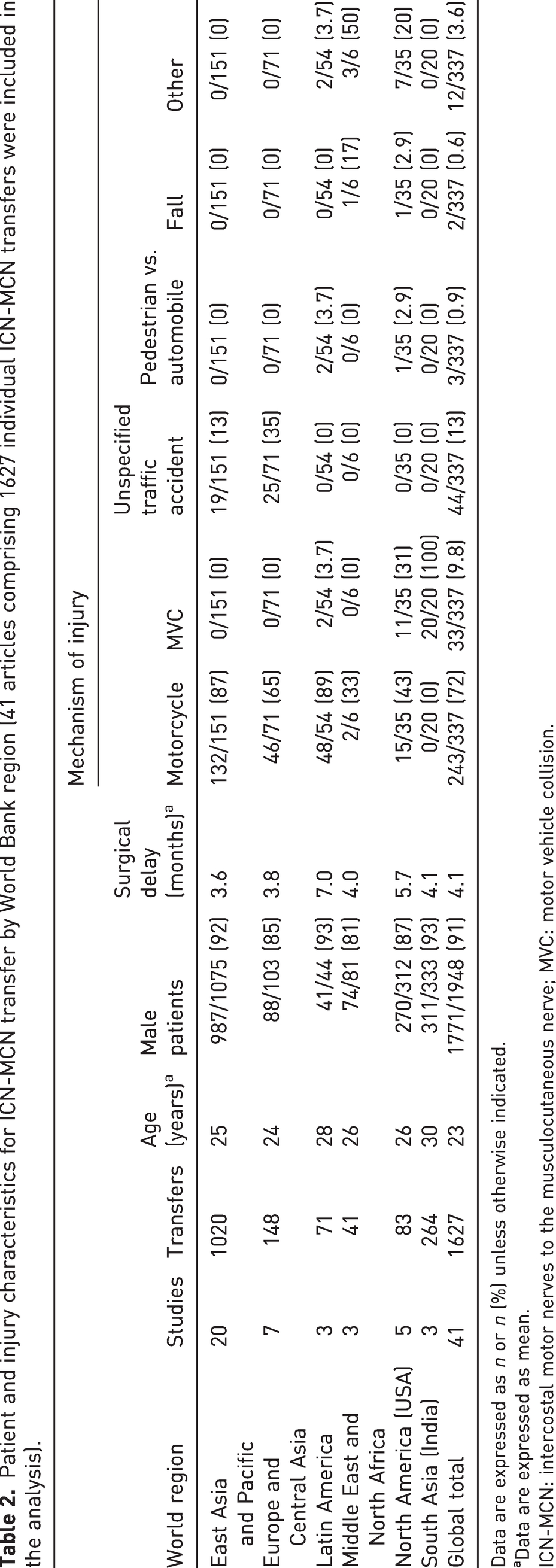
Data are expressed as n or n (%) unless otherwise indicated.
Data are expressed as mean.
ICN-MCN: intercostal motor nerves to the musculocutaneous nerve; MVC: motor vehicle collision.
The global weighted average BMRC grade for the ICN-MCN transfer was 2.8 (Figure 3(a)). East Asia reported the highest average BMRC grade (3.1). Elbow flexion of at least BMRC grade 3 and 4 strength was attained globally in 71% and 38% of patients, respectively (Figure 3(b)). East Asia had higher rates of recovery of BMRC strength compared to all other regions (p < 0.001) except for the Middle East (p = 0.62). With the exception of South Asia, there was no significant difference between regions with regard to BMRC grade 4 recovery (p = 0.40). Taiwan reported the highest recovery of BMRC grade 4 strength (67%), compared to a global aggregate of 38%.
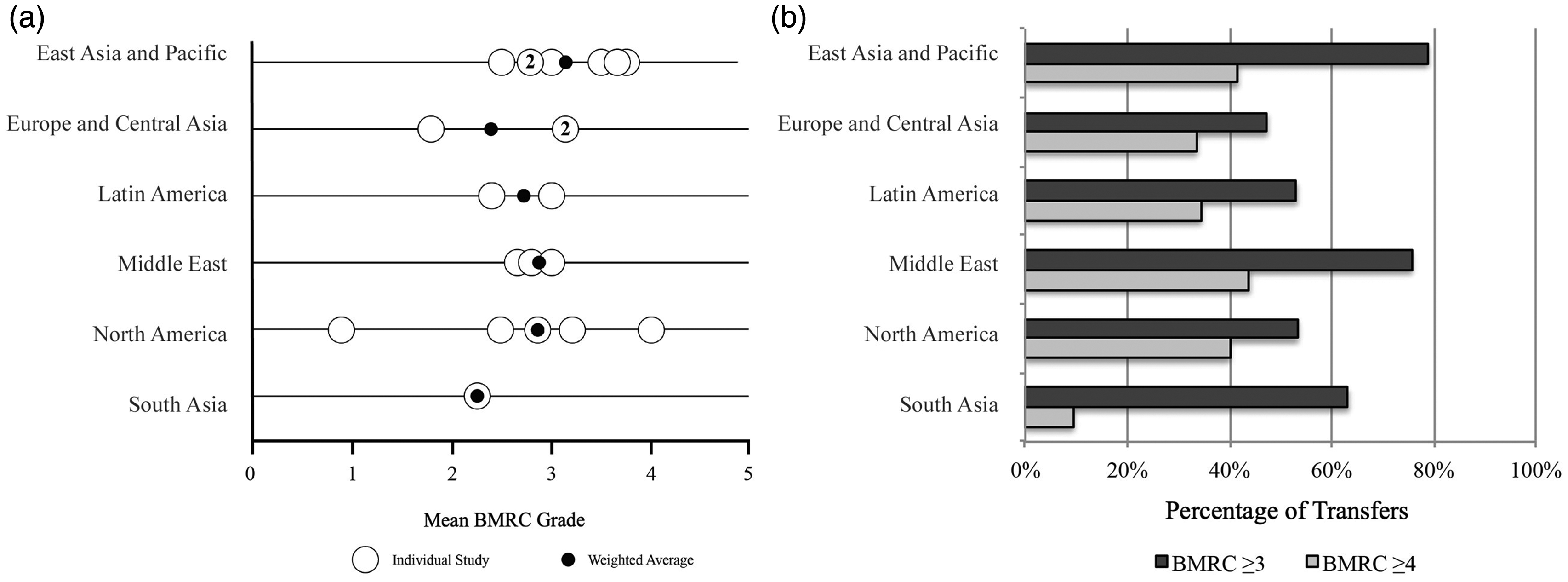
(a) Weighted average BMRC strength for elbow flexion after ICN-MCN transfer. Individual study outcomes (white) and weighted averages by region (black) are shown and (b) Percentage recovery of elbow flexion strength after ICN-MCN transfer. Proportion of patients obtaining at least BMRC strength 3 (dark grey) and 4 (light grey) are shown.
Fascicular transfers from the ulnar and/or median nerve for elbow flexion
Partial fascicular ulnar and/or median nerve transfer to biceps and/or brachialis nerves was the subject of 69 studies comprising 1397 individual nerve transfers with a mean follow-up of 29 months (Tables 3 and S7). Injuries were most commonly caused by motorcycle accidents (n = 411, 29%). Upper root with or without C7 involvement comprised the vast majority of injury patterns treated with ulnar nerve fascicle transfer (Figure S9). Single fascicular transfers (n = 1003, 72%) were more frequently employed compared to double fascicular transfers (n = 394, 28%) (Tables 4 and S8).
Patient and injury characteristics for fascicular transfer for elbow flexion by World Bank region (69 articles comprising 1397 individual fascicular transfers for elbow flexion were included in the analysis).
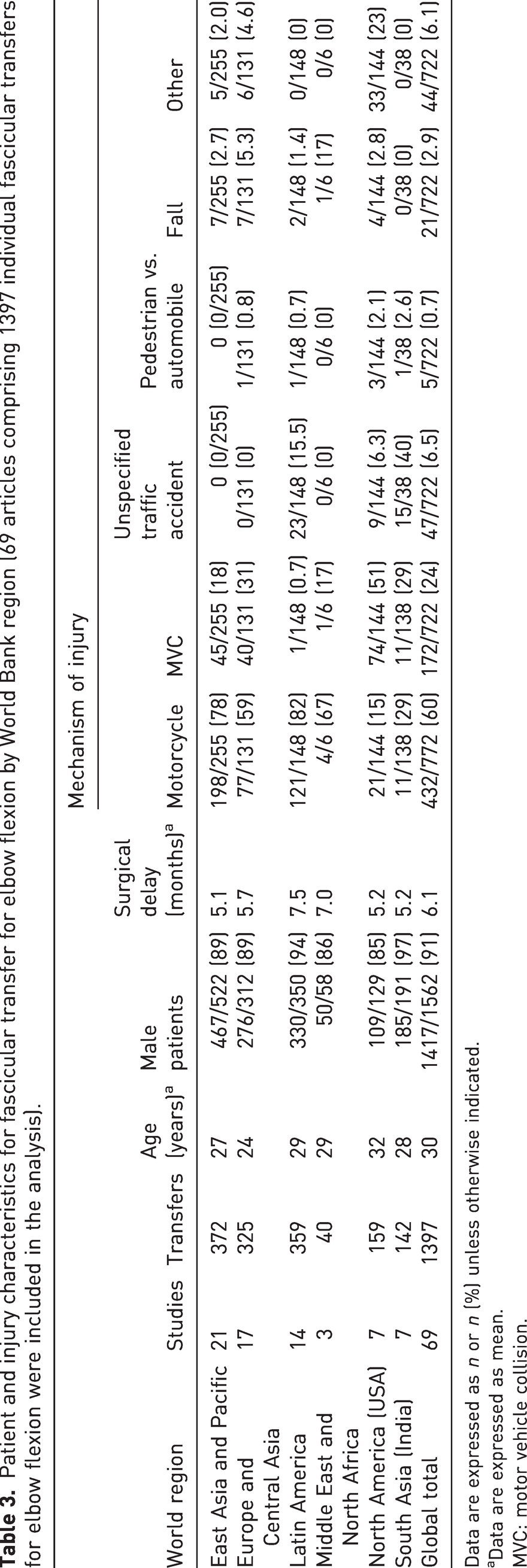
Data are expressed as n or n (%) unless otherwise indicated.
Data are expressed as mean.
MVC: motor vehicle collision.
Variations of fascicular transfer for elbow flexion technique by World Bank region (the specific donor and recipient nerves used for fascicular transfer are described for each transfer).
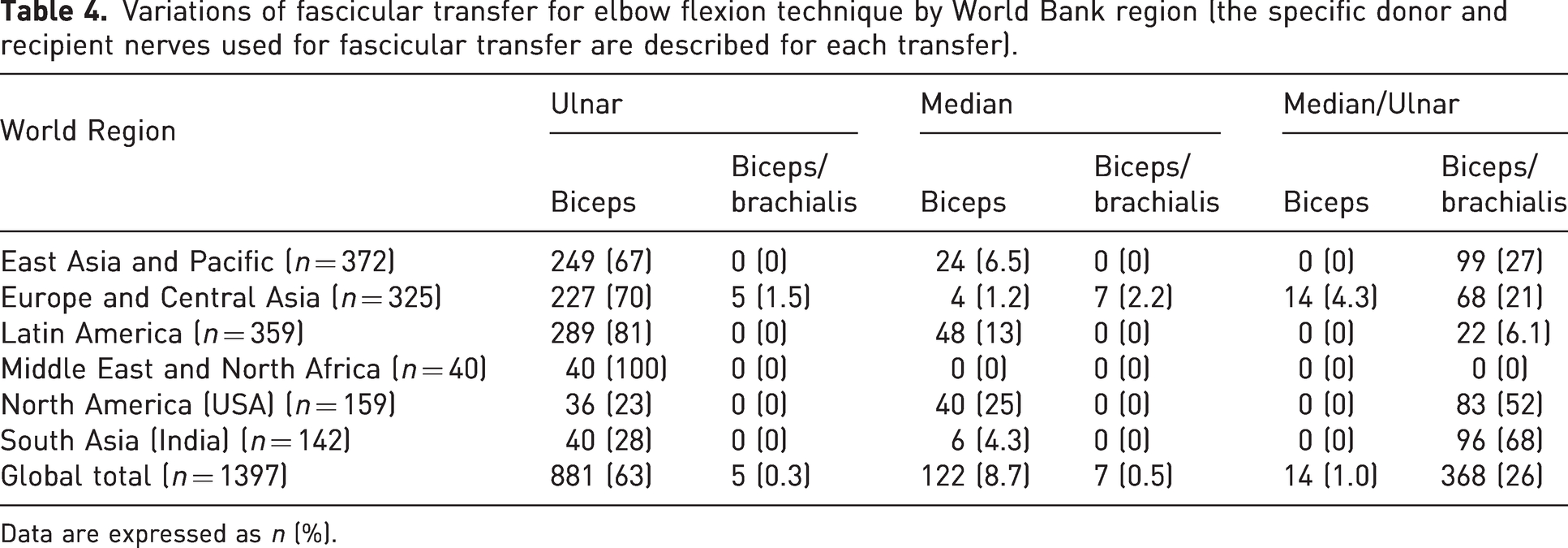
Data are expressed as n (%).
The global weighted average BMRC grade was 3.5 for single fascicular partial ulnar or median transfers compared to 3.8 for double fascicular transfers (Figure 4(a)). Elbow flexion of at least BMRC grade 3 and 4 strength after single fascicular transfer was attained globally in 87% and 72% of patients, respectively (Figure 4(b)). For single transfers, all regions demonstrated recoveries greater than 80%. BMRC grade 4 recovery was highest in North America (80%); however, this was not significantly different from recovery in Europe (78%, p = 0.65), East Asia (71%, p = 0.11) and the Middle East (78%, p = 0.72).
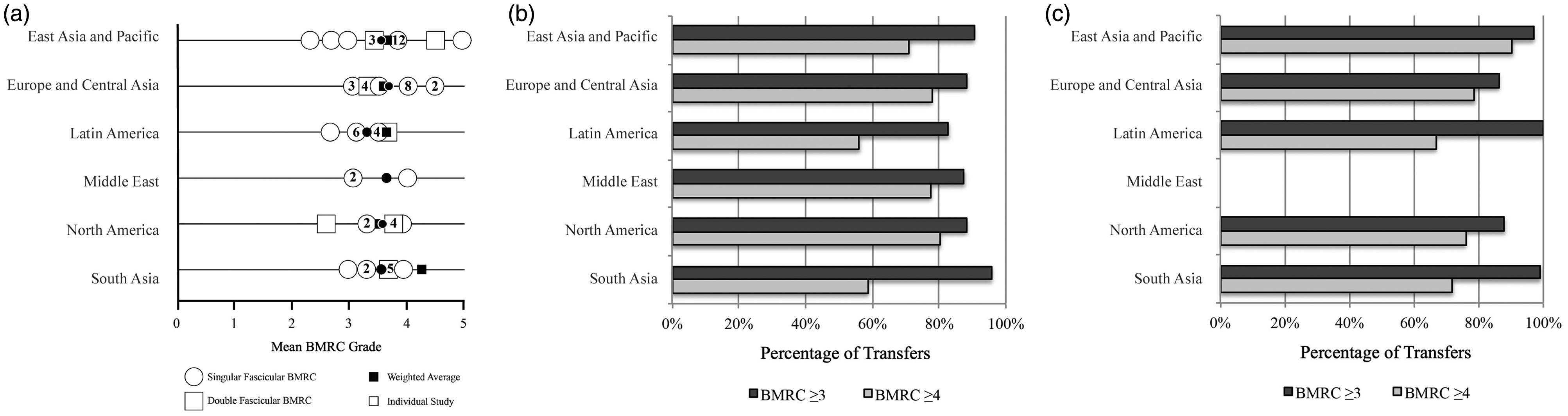
(a) Weighted average BMRC strength after fascicular transfer for elbow flexion. Single (circle), e.g. Oberlin, and double (square), e.g. MacKinnon, transfers are reported separately. Individual study outcomes (white) and weighted averages by region (black) are shown. (b) Percentage recovery of strength after single fascicular transfer for elbow flexion. Proportion of patients obtaining at least BMRC strength 3 (dark grey) and 4 (light grey) are shown and (c) Percentage recovery of strength after double fascicular transfer for elbow flexion. Proportion of patients obtaining at least BMRC strength 3 (dark grey) and 4 (light grey) are shown. No outcomes were available from studies originating in the Middle East.
Elbow flexion of at least BMRC grade 3 and 4 strength after double fascicular transfer was attained globally in 93% and 79% of patients, respectively (Figure 4(c)). For double fascicular transfers, recovery of BMRC grade 3 strength was uniformly >85%. BMRC grade 4 strength was achieved most frequently in East Asia (90%), which was significantly greater than all other regions (p < 0.05), except for Latin America where reports of BMRC grade 4 recovery were low (n = 3).
Discussion
Traumatic injuries of the brachial plexus remain a reconstructive challenge around the world. This study identified consistent features of BPI across geographic regions that parallel other forms of trauma – patients are typically young, male (Haagsma et al., 2016) and sustain injury in traffic accidents (James et al., 2020). Outside of these shared characteristics, the analysis demonstrated tremendous regional variability for three commonly performed nerve transfers.
The spinal accessory nerve is a well-studied donor nerve for restoring shoulder motion and is preserved in up to 95% of patients with BPI (Bertelli and Ghizoni, 2011). External rotation is exclusively restored by reinnervation of the suprascapular nerve for infraspinatus function. Therefore, recovery of external rotation is a proxy for success of the SAN-SSN transfer, especially when concomitant transfers or nerve grafting to the upper trunk and its distal targets have been performed. Such concomitant axillary nerve reinnervation was performed in over one-third of cases globally.
As the spinal accessory nerve is extraplexal, SAN-SSN transfer can be performed in a majority of injury patterns. While its use for upper plexus injuries was most frequently reported in the Middle East, Europe and South Asia, SAN-SSN was more commonly reported for pan-plexal injury in Latin America. This may be explained in part by a regional preference to transfer the SAN for other functional purposes (e.g. elbow flexion) in pan-plexus cases. Pre-ganglionic injury was reported in nearly all cases of SAN-SSN in East Asia, but was found in half of the studied patients in Latin America – consistent with a study from this region that found graftable C5 roots in 88% of cases (Bertelli et al., 2017).
Recovery of external rotation after SAN-SSN transfer is generally inferior compared to abduction (Bertelli and Ghizoni, 2016; Hsueh and Tu, 2020). Considerable regional variability exists with regard to rates of BRMC recovery, ranging from 53% to 86%. European literature reported the greatest recovery of strength in the postoperative follow-up period. No variations in patient age, surgical delay, approach or injury pattern can entirely account for these differences. Despite external rotation being a superior proxy for successful SAN-SSN transfer, it was reported less frequently compared to shoulder abduction.
Intercostal nerves may be used to reinnervate the biceps and brachialis muscles via the musculocutaneous nerve or distal branches. Although ICN-MCN nerve transfers can be performed in any injury pattern, the vast majority of reported transfers in the literature are indicated for pan-plexal injuries. The notable exception is Europe, in which two-thirds of cases treated with ICN-MCN transfer were upper trunk injuries (C5-6) with or without the involvement of the C7 root. The first possible explanation is that fewer pan-plexal injuries were reported in Europe overall regardless of specific transfer (14% vs. ≥30% for other regions). The second is that all but one study originating from Europe was published before Oberlin’s description of the partial ulnar fascicular transfer for elbow flexion (Oberlin et al., 1994).
The majority of published outcomes after ICN-MCN transfer originate in East Asia (de Mendonça Cardoso et al., 2020), and two nerves were most commonly transferred in this geographic region. Several comparative studies have shown that the number of intercostal nerves transferred does not affect strength (Kawai et al., 1988; Leland et al., 2018; Xiao et al., 2014). Consistent with this finding, average BMRC and proportion of patients reaching at least BMRC grade 3 after ICN-MCN transfer was highest in Asia despite generally fewer transferred nerves. Less variability was noted when weighted averages for ICN-MCN transfer were compared across regions, in contrast to the significant variability of SAN-SSN transfer outcomes.
Fascicular transfer for elbow flexion is another means of restoring elbow flexion in patients with BPI and was initially described utilizing fascicles of the ulnar nerve (Oberlin et al., 1994). Several variations have since been published (Mackinnon et al., 2005; Sungpet et al., 2023). The fascicular transfer technique has become a widely accepted and performed transfer around the world, greatly outnumbering published reports of ICN-MCN transfer after 2005. As expected, all patients undergoing this transfer sustained upper trunk injury with or without C7 involvement. Similar to SAN-SSN transfers, pre-ganglionic injury was reported to be highest in East Asia and lowest in Latin America and South Asia. This difference may be in part due to how root avulsion injuries are diagnosed and defined.
Outcomes of fascicular transfers for elbow flexion demonstrated considerably less inter-regional variability compared to SAN-SSN transfer. Unlike ICN-MCN transfer, weighted average outcomes of fascicular transfers were favourable and approached BMRC 4 in all regions. Over 80% of patients achieved BMRC grade 3 strength after single fascicular transfer globally, with East Asia, South Asia and Latin America reporting nearly 100% grade 3 strength after double fascicular transfer. This is consequently a highly reproducible transfer with generally good outcomes across geographic areas. Contributing to its success is its narrower indication for upper plexus injury with intact ulnar and/or median nerve function, relatively straightforward anatomical dissection in unscarred areas and close distance to the target recipient nerve(s).
The present study has some limitations. The most substantial limitation is the vast heterogeneity of data reported; specifically, the manner by which studies of BPI report functional data varied considerably. These reporting differences limit the ability to determine the statistical significance of geographic differences. BMI, injury mechanism, severity measures (i.e. injury severity score), energy and associated concomitant trauma were also inconsistently reported, but are likely to vary geographically. These features provide important prognostic information that cannot otherwise be accounted for when assessing outcomes after BPI. A subset of articles may have been missed by searching three databases and some were inaccessible altogether.
Variations in reporting BMRC muscle grade, unique non-standard methods of strength measurement and inconsistent measures of motion without use of a standard consensus make comparisons between authors and regions challenging. The development of standardized data reporting would allow for the comparison of BPI outcomes across groups and regions. At a minimum, this should include demographic information, energy and mechanism of injury, level of brachial plexus involvement, pre- versus post-ganglionic injury and standardized outcome measures (BMRC strength, range of motion, validated pain measures and patient-reported outcome measures) (Miller et al., 2023; Quick and Brown, 2020).
These limitations notwithstanding, we have demonstrated that the outcomes of BPI reconstruction clearly vary across regions. However, the magnitude of those differences seems to be inherent to the specific transfer being utilized. An understanding of what makes a nerve transfer reproducible and geographic factors that might affect their outcomes should continue to be a priority for future research.
Supplemental Material
sj-pdf-1-jhs-10.1177_17531934241232062 - Supplemental material for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries
Supplemental material, sj-pdf-1-jhs-10.1177_17531934241232062 for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries by Christopher S. Crowe, Robert J. Spinner and Alexander Y. Shin in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-2-jhs-10.1177_17531934241232062 - Supplemental material for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries
Supplemental material, sj-pdf-2-jhs-10.1177_17531934241232062 for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries by Christopher S. Crowe, Robert J. Spinner and Alexander Y. Shin in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-3-jhs-10.1177_17531934241232062 - Supplemental material for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries
Supplemental material, sj-pdf-3-jhs-10.1177_17531934241232062 for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries by Christopher S. Crowe, Robert J. Spinner and Alexander Y. Shin in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-4-jhs-10.1177_17531934241232062 - Supplemental material for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries
Supplemental material, sj-pdf-4-jhs-10.1177_17531934241232062 for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries by Christopher S. Crowe, Robert J. Spinner and Alexander Y. Shin in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-5-jhs-10.1177_17531934241232062 - Supplemental material for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries
Supplemental material, sj-pdf-5-jhs-10.1177_17531934241232062 for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries by Christopher S. Crowe, Robert J. Spinner and Alexander Y. Shin in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-6-jhs-10.1177_17531934241232062 - Supplemental material for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries
Supplemental material, sj-pdf-6-jhs-10.1177_17531934241232062 for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries by Christopher S. Crowe, Robert J. Spinner and Alexander Y. Shin in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-7-jhs-10.1177_17531934241232062 - Supplemental material for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries
Supplemental material, sj-pdf-7-jhs-10.1177_17531934241232062 for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries by Christopher S. Crowe, Robert J. Spinner and Alexander Y. Shin in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-8-jhs-10.1177_17531934241232062 - Supplemental material for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries
Supplemental material, sj-pdf-8-jhs-10.1177_17531934241232062 for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries by Christopher S. Crowe, Robert J. Spinner and Alexander Y. Shin in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-9-jhs-10.1177_17531934241232062 - Supplemental material for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries
Supplemental material, sj-pdf-9-jhs-10.1177_17531934241232062 for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries by Christopher S. Crowe, Robert J. Spinner and Alexander Y. Shin in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-10-jhs-10.1177_17531934241232062 - Supplemental material for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries
Supplemental material, sj-pdf-10-jhs-10.1177_17531934241232062 for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries by Christopher S. Crowe, Robert J. Spinner and Alexander Y. Shin in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-11-jhs-10.1177_17531934241232062 - Supplemental material for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries
Supplemental material, sj-pdf-11-jhs-10.1177_17531934241232062 for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries by Christopher S. Crowe, Robert J. Spinner and Alexander Y. Shin in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-12-jhs-10.1177_17531934241232062 - Supplemental material for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries
Supplemental material, sj-pdf-12-jhs-10.1177_17531934241232062 for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries by Christopher S. Crowe, Robert J. Spinner and Alexander Y. Shin in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-13-jhs-10.1177_17531934241232062 - Supplemental material for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries
Supplemental material, sj-pdf-13-jhs-10.1177_17531934241232062 for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries by Christopher S. Crowe, Robert J. Spinner and Alexander Y. Shin in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-14-jhs-10.1177_17531934241232062 - Supplemental material for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries
Supplemental material, sj-pdf-14-jhs-10.1177_17531934241232062 for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries by Christopher S. Crowe, Robert J. Spinner and Alexander Y. Shin in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-15-jhs-10.1177_17531934241232062 - Supplemental material for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries
Supplemental material, sj-pdf-15-jhs-10.1177_17531934241232062 for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries by Christopher S. Crowe, Robert J. Spinner and Alexander Y. Shin in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-16-jhs-10.1177_17531934241232062 - Supplemental material for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries
Supplemental material, sj-pdf-16-jhs-10.1177_17531934241232062 for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries by Christopher S. Crowe, Robert J. Spinner and Alexander Y. Shin in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-17-jhs-10.1177_17531934241232062 - Supplemental material for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries
Supplemental material, sj-pdf-17-jhs-10.1177_17531934241232062 for Global trends and outcomes of nerve transfers for treatment of adult brachial plexus injuries by Christopher S. Crowe, Robert J. Spinner and Alexander Y. Shin in Journal of Hand Surgery (European Volume)
Footnotes
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The Mayo Clinic does not require ethical approval for reporting systematic review and meta-analysis.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.