
Abstract
Despite being in use for over 25 years, long-term data regarding the Herbert ulnar head prosthesis remain scarce. The aim of the present multicentre observational study was to describe the survivorship of this implant in the UK. Retrospective data were collected from clinical records and via telephone consultation. Data were submitted for 227 primary and five revision ulnar head prostheses. Indications for surgery included distal radioulnar joint osteoarthritis, inflammatory arthritis and failed ulnar head resection surgery. The mean follow-up was 5.5 years (range 1 month–21 years) with 91% (n = 108) and 87% (n = 44) survival at 5 and 10 years, respectively. Indications for reoperation included pain, instability, aseptic loosening and distal impaction. In total, 12 patients had implant removal, eight had revision arthroplasty and five underwent soft tissue stabilization. Overall, reassuring mid- to long term survivorship data for the ulnar head prosthesis were found. We recommend the use of arthroplasty registries for implant surveillance.
Level of evidence:
IV
Keywords
Introduction
The Herbert ulnar head prosthesis (UHP; KLS Martin, Freiburg, Germany) is one option for the management of distal radioulnar joint (DRUJ) pathology. The UHP is an uncemented DRUJ hemiarthroplasty, featuring a titanium ulnar stem with a modular neck and a ceramic head for articulation with the native radial sigmoid notch (Figure 1). It is the only DRUJ hemiarthroplasty currently available in the UK. It is designed to relieve pain, preserve motion and maximize function for a variety of indications, including osteoarthritis and inflammatory arthritis.
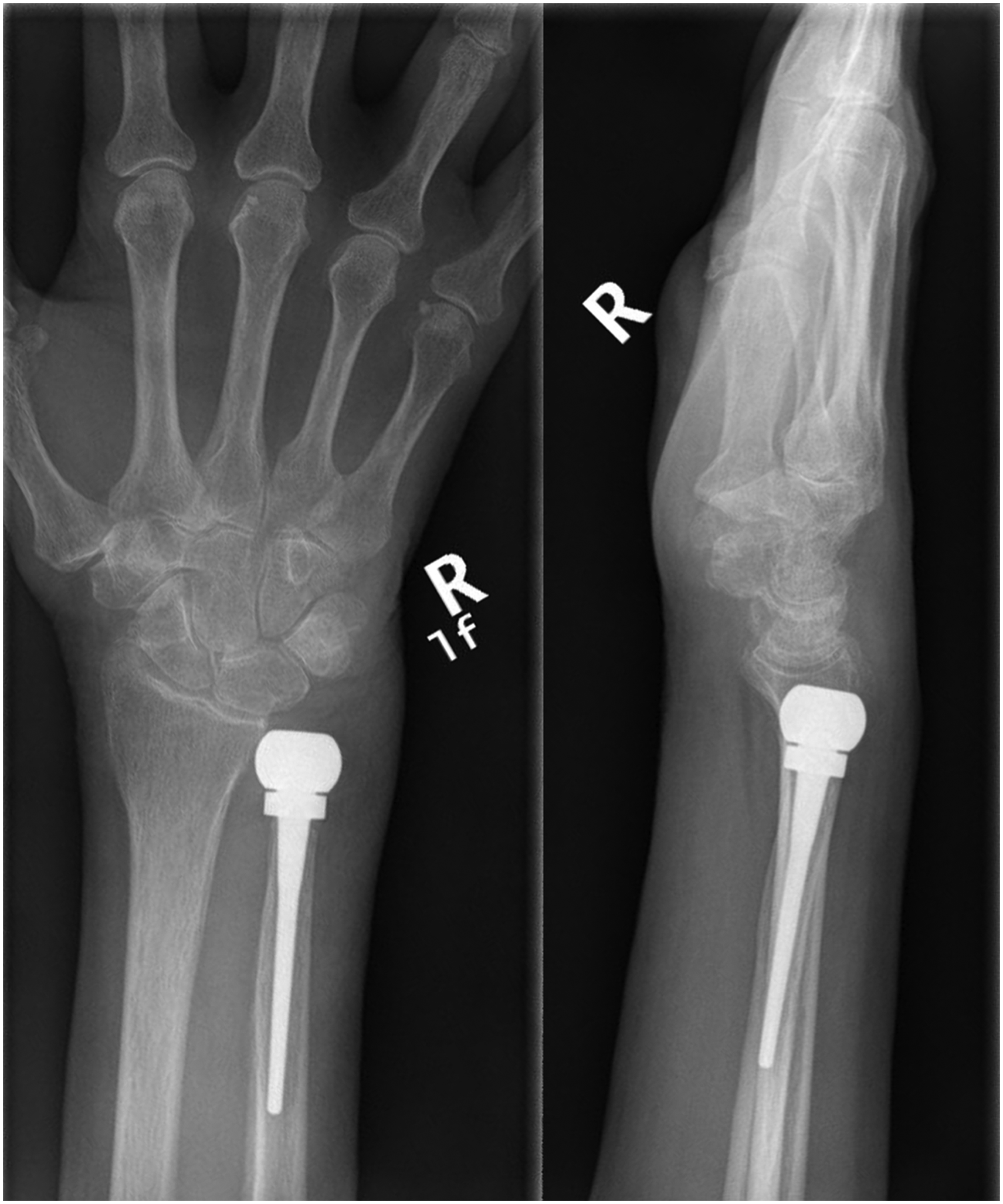
Posteroanterior and lateral radiographs of a 66-year-old woman with an ulnar head prosthesis in situ for 5 years.
The UHP has increased in popularity as an alternative to salvage surgery (Moulton and Giddins, 2017). In addition, it can be used in the setting of unsuccessful previous salvage surgery. Despite over 25 years of experience and increasing usage of the UHP, there remains a paucity of literature relating to this implant (Kakar et al., 2012; Sabo et al., 2014; van Schoonhoven et al., 2012; Warwick et al., 2013). To our knowledge, there is only one systematic review of the UHP (Moulton and Giddins, 2017) whereas all other publications are level IV case series. The largest of these contains fewer than 60 cases (Warwick et al., 2013). The majority, if not all, current case series contain data from a single centre. The aim of the present study was to establish the medium- to long-term survivorship of the UHP. We also report on complications associated with the UHP.
Methods
We approached the supplier for a list of UHP invoices within the UK, including the date of billing and hospital name. The study period was 1 October 2001 to 31 December 2022; the former reflecting the earliest invoice date available. During this time, 893 UHPs had been distributed to 101 UK centres. We contacted hand and wrist surgeons from the 25 centres with the highest UHP usage. To maximize the data capture, we also advertised this study on the British Society for Surgery of the Hand (BSSH) online discussion forum. We invited surgeons with any number of UHPs to contribute to the study, accepting that this implant is used in low volumes by most. Data were submitted from 21 surgeons in 13 centres, comprising 227 primary and five revision UHPs. Figure 2 depicts the total number of UHP cases, those included in the study and their fates.
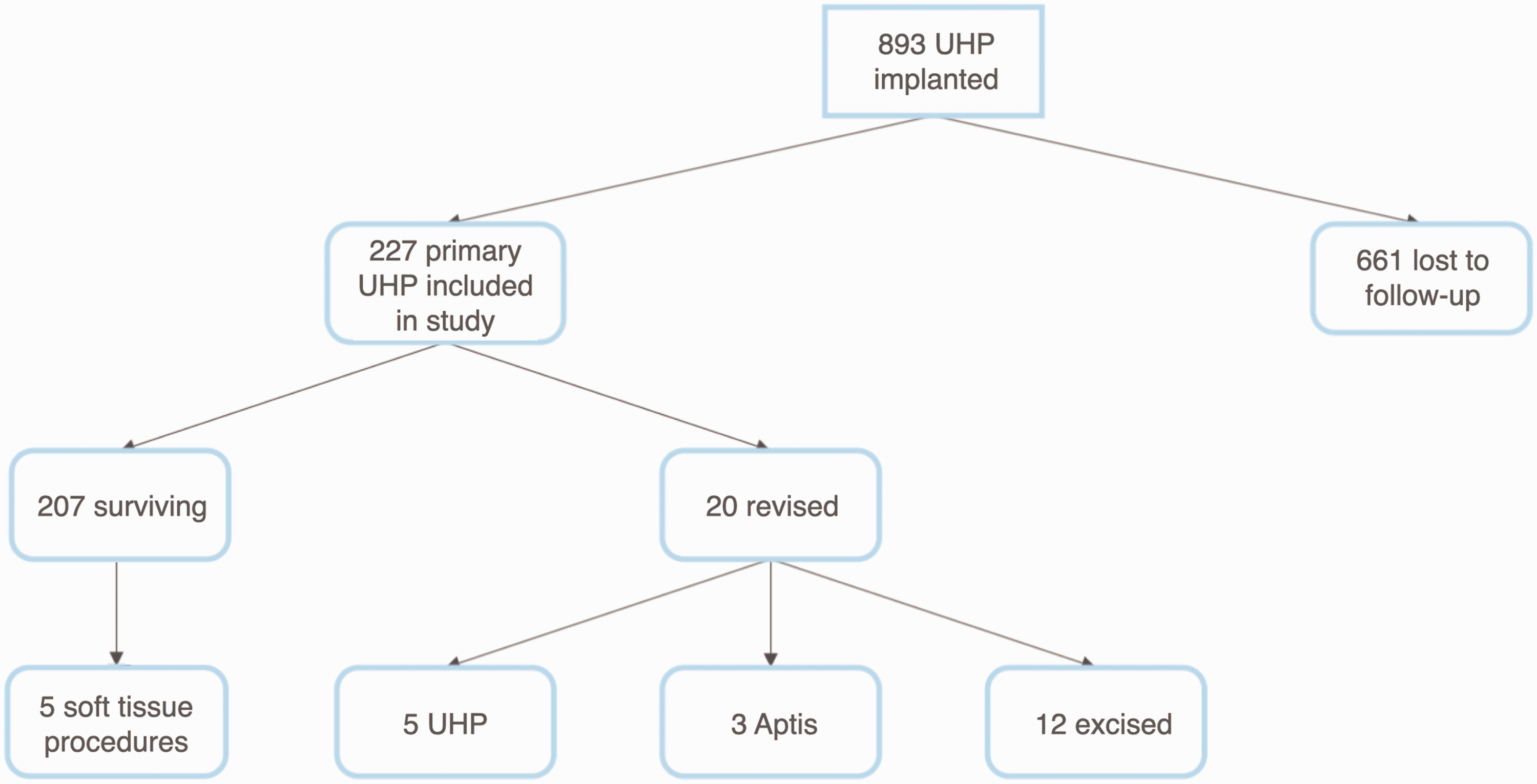
Flow chart showing total number of ulnar head prostheses (UHP) implanted in the UK during the study period, proportion captured and their fates.
Following local governance approval at each site, participating surgeons identified their cases of UHP using the invoice list and personal logbook data. Retrospective data were collected by participating surgeons from clinical records including, where applicable, date of birth, date of surgery, indication for surgery, concurrent wrist procedures, complications, date of revision, indication for revision, type of revision procedure, death and date of death. Revision UHPs were included in the survival analysis. Cases were anonymized and entered onto Excel spreadsheets, which were then collated by the primary authors. Cases with incomplete data were not accepted.
Revision was defined as implant removal or replacement of any or all the components. Reoperations that were purely soft tissue procedures were also investigated. Surgeons were asked to review records for all clinical follow-ups since the index procedure. In addition, they were asked to telephone patients to verbally confirm survivorship of the implant since their last clinical follow-up. This was to maximize the follow-up time for survivorship while minimizing the risk of missed events (such as revision surgery at a different hospital since last local clinical follow-up). We performed a Kaplan–Meier survival analysis.
Results
This study analysed 232 UHPs (227 primary and 5 revision) in 219 patients. The caseload per consultant surgeon was in the range of 1–57 cases. The date of index surgery spanned a 21-year period between October 2001 and December 2022. The age at index surgery was in the range of 25–89 years (mean 64 years). The most common indication for surgery was primary osteoarthritis (104 cases), followed by rheumatoid arthritis (55 cases). Less common indications included failed DRUJ salvage surgery (Darrach or Sauvé-Kapandji), post-traumatic osteoarthritis and Vaughan Jackson syndrome, among others (Table 1). In total, 17 UHPs were used in conjunction with other procedures: wrist arthroplasty and partial and total wrist arthrodesis. These other procedures took place before, simultaneously or after UHP implantation. Eight patients had bilateral implants, and one of these received a unilateral revision UHP.
Primary ulnar head prosthesis (UHP) patient demographics.
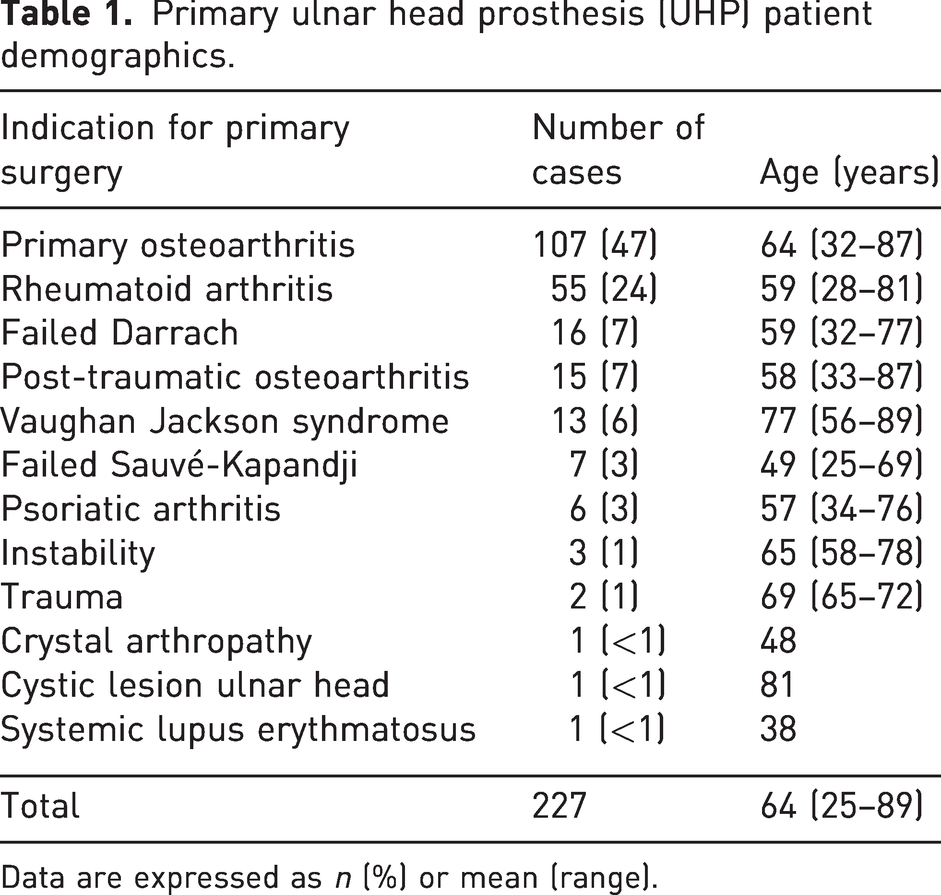
Data are expressed as n (%) or mean (range).
As shown in Figure 3, the cumulative survival for the UHP was 99% (95% confidence interval [CI]: 96 to 100) at 1 year (n = 181), 96% (95% CI: 92 to 98) at 2 years (n = 155), 91% (95% CI: 85 to 94) at 5 years (n = 108) and 87% (95% CI: 80 to 91) at 10, 15 and 20 years (n = 44, 15 and 3, respectively). The overall reoperation incidence was 11% (25 cases). The commonest indication for implant revision was pain (six cases), followed by aseptic loosening and ulnar carpal impaction. Revision took place in seven UHPs primarily indicated for osteoarthritis, five for rheumatoid arthritis and three for failed salvage surgery, among others. A total of 12 patients underwent implant excision; five had revision UHPs and three were converted to total DRUJ arthroplasty using an Aptis implant (Aptis Medical, Louisville, KT, USA). Revision surgery occurred between 4 months and 6 years after the index surgery. Half of the revisions occurred within 2 years of the index procedure. All five revision UHPs were surviving at the last follow-up, which was at a mean of 7 years (range 2–14).
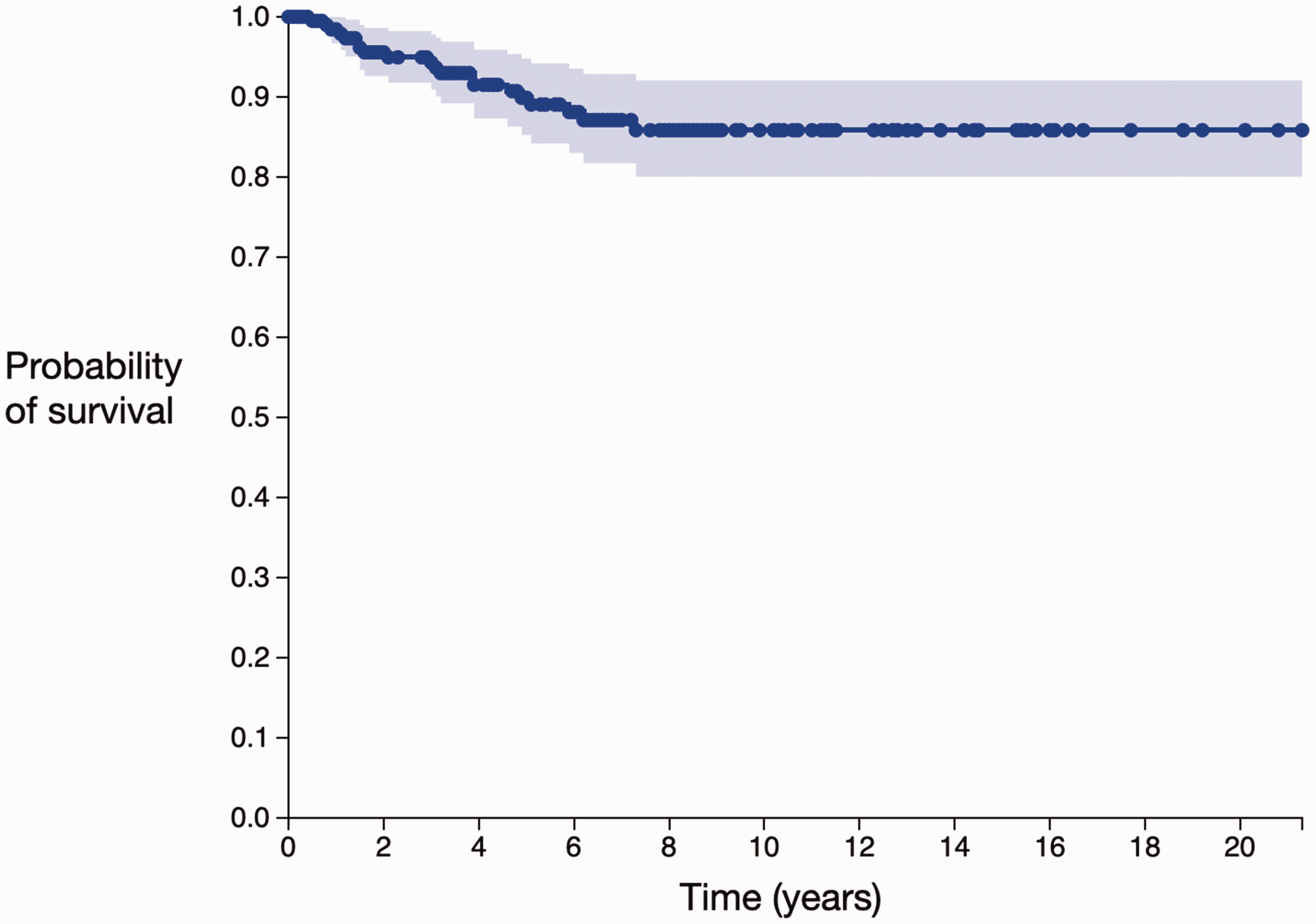
The Kaplan–Meier survival estimate for 232 ulnar head prostheses. The blue dots represent censored cases. Light blue shading represents the 95% confidence interval.
Complications were reported in 44 (19%) primary cases (Table 2); 13 had ongoing pain, eight had DRUJ instability and six had ulnar carpal impaction. Five patients underwent soft tissue stabilization procedures after their primary surgery. Three other cases had infection. Two deep infections required implant excision, and one superficial infection settled with a course of antibiotics. In total, 27 patients died during the study period, three of whom had bilateral UHPs. All of these patients died with their primary UHP in situ, except for one patient who died 8 years after implant excision for deep infection. Those who died did so between 6 months and 15 years after their primary surgery (mean 6 years), at a mean age of 81 years (range 42–95). The cause of death was unrelated to the UHP in each case.
Complications and revisions after primary ulnar head prosthesis (UHP).
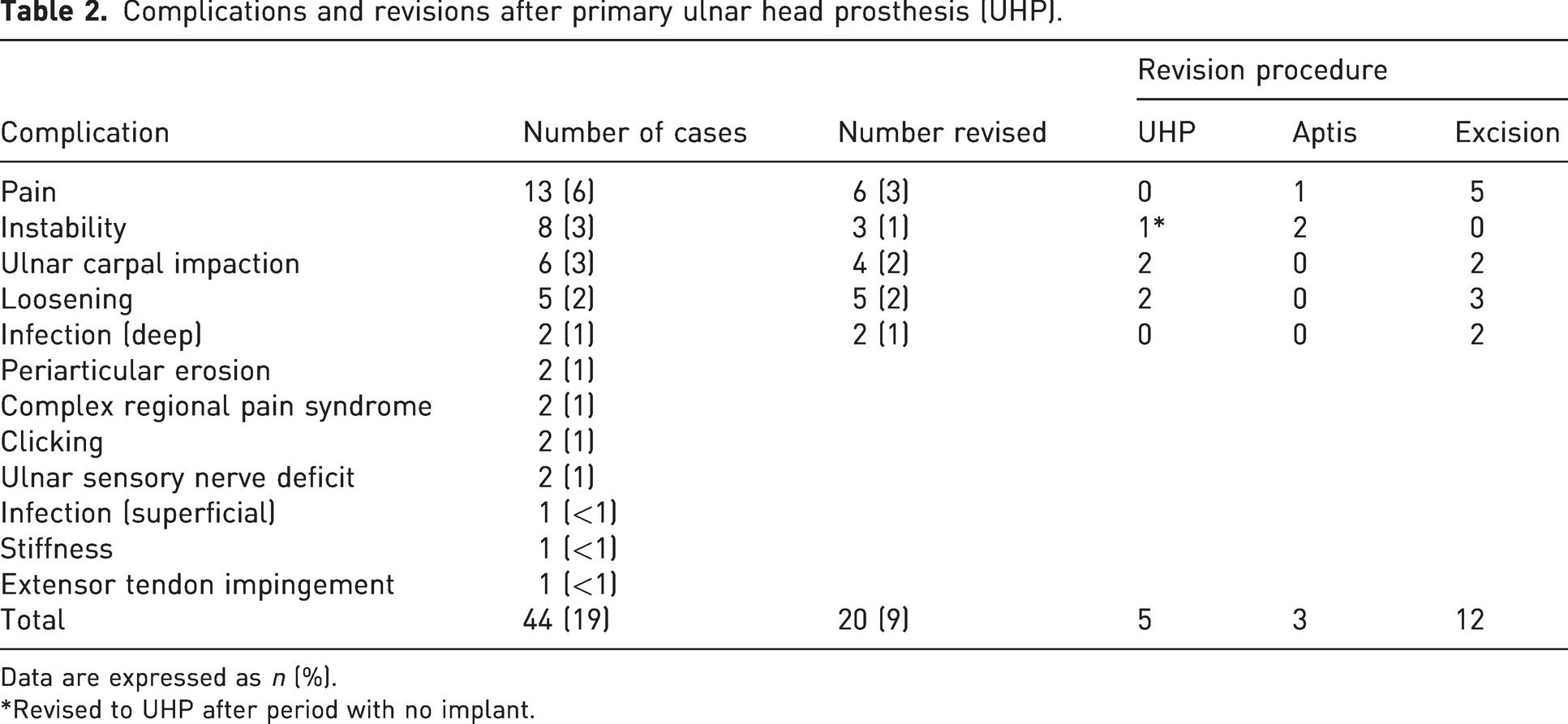
Data are expressed as n (%).
*Revised to UHP after period with no implant.
Discussion
The present study reports on 227 primary and five revision UHPs. Thanks to the implant supplier, we were able to identify dates and locations of UHP surgery across the UK. A total of 893 UHPs were implanted in the UK during our 21-year study period, of which data from 26% were captured in this study. We harnessed the power of collaboration to obtain meaningful results by directly contacting individuals working at the identified centres and via advertising the study on the BSSH online discussion forum. We found our colleagues were willing to contribute their data, and together were able to obtain a substantial amount of data on this relatively rare procedure. This study has the advantage of including data from multiple surgeons in different centres, whereas previous literature focused on single centre/surgeon case series.
Our overall implant revision incidence was 9%, equivalent to that of Sabo et al. (2014) in their series of 79 DRUJ hemiarthroplasties of various types. Half of the revisions in our cohort occurred within 2 years of primary surgery. The existing literature agrees that early revisions predominate (Sabo et al, 2014). Kakar et al. (2012) reported an overall 30% reoperation incidence in their series of 47 patients. Eight patients (17%) required implant excision or replacement. They proposed the following potential risk factors for revision: use of an extended collar; lucency of >2 mm around the implant; bony pedestal formation; and dorsal DRUJ translation >5 mm. These factors may be surrogate markers for ulnar carpal impaction, loosening and DRUJ instability, respectively. We propose that early revisions may be the result of inappropriate implant positioning, sizing or soft tissue tensioning, and that good surgical technique may protect against early revision. Our study found a similar revision incidence between primary indication subgroups, with no apparent correlation between age and revision (mean 60 years; range 28–80 years).
There is a paucity of survival data described in published case series of the UHP. Kakar et al. (2012) found an 83% survival rate of 47 UHPs at 6 years. Sabo et al. (2014) analysed 79 cases of various ulnar head implants (including the UHP) and noted a 5- and 15-year survival rate of 90%. All of the implant revisions in this series occurred within 26 months of the primary surgery. Survival of the Aptis total DRUJ prosthesis appears to be comparable to the UHP, with Stougie et al. (2023) demonstrating a 92% survival at 4 years. However, they found an alarmingly high incidence of reoperation (41%) among their 59 cases. At 10 years, Lambrecht et al. (2022) reported an 84% survival rate with the Aptis prosthesis.
Moulton and Giddins (2017) performed a systematic review of the UHP, concluding that clinical and patient-reported outcomes generally improved, while complications were low. Our study found an overall complication incidence of 19%, which included minor problems such as clicking. Pain was both the most common reported complication and the most common reason for revision (6 of 20 cases) in our series. Instability was the second most common complication in our series. Waseem et al. (2008) found instability to be the most common complication. This conflicts with van Schoonhoven et al.’s (2012) case series of 16 patients, where all were reported to have a clinically stable DRUJ postoperatively. A recent article has cast doubt over the reliability of clinical assessment of DRUJ stability; this may influence the variable results regarding this parameter (Pickering et al., 2022).
Previous publications suggest overall improvement in patient-reported outcome measures (PROMs) after UHP, along with high patient satisfaction (Warwick et al., 2013). Moreover, PROMs improved regardless of primary indication in one study by Shipley et al. (2009). This makes the UHP an attractive option for patients with failed salvage surgery, when alternatives are sparse. Fernandez et al. (2006) found most patients returned to their previous type of employment after UHP, bolstering its reputation for good functional outcomes. However, not all studies have reported the UHP so favourably, with substantial disability persisting in a high proportion of cases in the paper by Sabo et al. (2014). Despite this, patients were generally satisfied with their outcomes.
The UHP, while biomechanically closer to normal than results from DRUJ salvage surgery, does not restore a normal wrist (Masaoka et al., 2002). Appropriate preoperative counselling and careful surgical technique are requisite. Persistent pain and ulnar carpal impaction can result from failure to restore DRUJ congruence, while instability can result from inadequate tensioning of the soft tissue envelope (Grechenig et al., 2001). The Getting it Right First Time and Beyond Compliance initiatives aim to improve orthopaedic implant stewardship (Briggs, 2015). Hand registries, such as the UK Hand Registry, are gaining popularity (Vakalopoulos et al., 2021). It seems likely that routine use of these will soon be encouraged if not mandated, as they are for many other joint arthroplasties in the UK. Data from such registries will likely help further our knowledge of the UHP to ultimately improve patient care.
The present study has some limitations. Due to its retrospective nature, it was not possible to obtain a complete, standardized set of outcome data to include validated patient-reported, clinical or radiographic outcome measures. This information, in combination with survivorship, would provide a comprehensive evidence base for the UHP. The study only captured 26% of the documented total number of UHPs implanted in the UK during the study period. We cannot account for the remaining 661 UHPs that were implanted during this time. This raises a considerable risk of selection bias, if those surgeons with good results were more willing to submit their data. Many of the cases included in this study have previously been included in separate studies, meaning this work should not be incorporated into systematic review for risk of duplication (Warwick et al., 2013; Waseem et al., 2008).
We recognize heterogeneity in follow-up time between cases, accepting that survivorship of recently implanted UHPs is less useful than of those with several years of follow-up. We concede that there is a wide range of surgical indications and expect that more than one may apply in certain cases. For example, those with failed salvage surgery or Vaughan Jackson syndrome may also have rheumatoid arthritis. It is possible that these patient factors (among others we did not account for) influenced the UHP survivorship, even though our study did not find it to be the case. We included cases with any indication for surgery, as we believe this presents a realistic spectrum of pathology. There may be other factors influencing the longevity of the implant, such as surgical technique, which are beyond the scope of this study.
This case series reports excellent survivorship of the UHP. Revision rates were lower than benchmark criteria of 10% at 5 years and 15% at 10 years set by the Orthopaedic Data Evaluation Panel for wrist arthroplasty (ODEP, 2023). With the data currently available, we recommend the use of the UHP but acknowledge an ongoing need for comprehensive, prospective research. In the absence of mandatory hand and wrist arthroplasty registries, this study demonstrates the power of collaboration to provide meaningful implant survivorship information. We support the use of registries for implant surveillance and for high-quality, large-scale research to answer questions about patient-reported and clinical outcomes for both this implant and others.
Footnotes
Acknowledgements
We would like to thank Mr Richard Kinzler for enabling us to locate the implants used and connect us with the relevant surgeons across the UK.
Contributors
The Herbert Collaborative: Jeff Auyeung, Country Durham and Darlington NHS Foundation Trust; Eleni Balabanidou, University Hospital Southampton; David M. S. Bodansky, Chelsea and Westminster Hospital; Daniel J. Brown, Liverpool University Hospitals NHS Foundation Trust; Adrian Chojnowski, Norfolk and Norwich University NHS Trust Hospital; Sherif Fetouh, University Hospital Southampton; Angus K. Y. Fong, Sheffield Teaching Hospitals; Akintunde George, University Hospital Southampton; Alistair J. Graham, Buckinghamshire Healthcare NHS Trust; Rhodri Gwyn, Royal Sussex County Hospital; Eshelle N. Hara, Sheffield Teaching Hospitals; Maxim D. Horwitz, Chelsea and Westminster NHS Foundation Trust; George J. M. Hourston, Peterborough City Hospital; Edwin P. Jesudason, Ysbyty Gwynedd, Bangor; Damilola T. Jimoh, University Hospital Southampton; Jonathan W. M. Jones, Peterborough City Hospital; Sarah Lewis, Buckinghamshire Healthcare NHS Trust; Lucy C. Maling, Queen Elizabeth the Queen Mother Hospital; Deepika Pinto, Ysbyty Gwynedd, Bangor; Grzegorz Sianos, Glasgow Royal Infirmary; Andrew M. Smith, Queen Elizabeth the Queen Mother Hospital; Philip A. Storey, Sheffield Hand Centre; Joseph Turner, Royal Sussex County Hospital; David Warwick, University Hospital Southampton; Khaled Youssef, University Hospital Southampton; Daniel T. Watts, Peterborough City Hospital; Chris R. P. Williams, Royal Sussex County Hospital; Mark Williamson, Queen Elizabeth the Queen Mother Hospital.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was obtained from East Kent Hospitals University NHS Foundation Trust Research Department.
Informed consent
Informed consent was not sought for the present study because according to the NHS Health Research Authority it falls under the category ‘surveillance’, not research.