
Abstract
The primary aim of this study was to report outcomes after fingertip terminalization in 90 patients over a 19-year period. We report excellent functional outcomes and satisfaction, but a 33% incidence of neuropathic pain.
Fingertip injuries are most common in manual workers in the manufacturing or construction industries. Broad surgical strategies include replantation, reconstruction and terminalization. Terminalization is often a favoured option for manual workers, often because of an expected faster return to work. Most of the previous studies examining terminalizations focus on short-term outcomes and there is little objective examination of cold-intolerance or neuropathic pain (Wang et al., 2013). The primary aim of this study was to describe the long-term patient-reported functional outcomes (PROMs) after primary terminalization for acute fingertip injuries. The secondary aims were to assess complications, patient satisfaction and the incidence of neuropathic pain.
This was a single-centre-retrospective study in a district general hospital. All patients who underwent primary terminalization after traumatic fingertip injuries between 2000 and 2018 were included. All operations were either performed or supervised by a single consultant hand surgeon. The primary outcome measure was the Quick version of the Disabilities of the Arm, Shoulder and Hand (QuickDASH) score. Patients also completed the Leeds Assessment of Neuropathic Symptoms and Signs Scale (LANSS) to look for the presence of neuropathic pain. Patient satisfaction was assessed, and the Normal Hand Score and Net Promoter Score (NPS) were also included. The Normal Hand Score assesses self-perceived hand normality in terms of look, feel and function on a 100-point Likert scale with 0 indicating ‘least normal’ and 100 indicating ‘most normal’. The NPS is a metric derived from the ‘friends and family test’ and examines how likely a patient is to recommend the procedure to a friend or family member from 0 (extremely unlikely) to 100 (extremely likely). Scores >90 are considered promoters, and scores <70 are classified as detractors. The percentage of promoters minus the percentage of detractors gives the NPS. A NPS greater than 50 is considered excellent. Patients were also asked how long it was before they returned to work, as well as whether their employment status had changed as a result of the injury, taking into account duties, hours and any career changes.
In total, 76 patients were alive at the time of follow-up and complete follow-up was available for 51 (67%) patients at a mean follow-up of 14 years (SD 5; range 4–22). Patient and injury characteristics are summarized in Table 1. There were no statistically significant demographic differences between responders and non-responders.
Patient and injury characteristics.
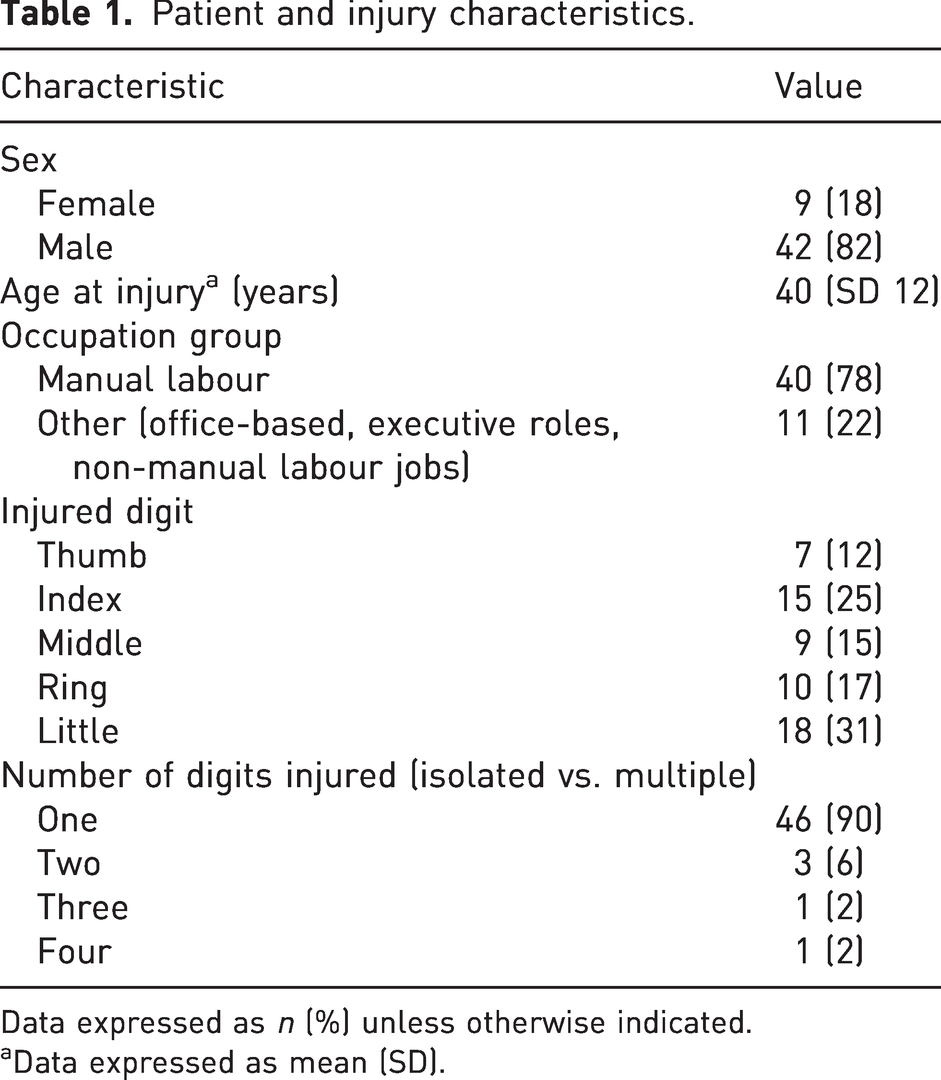
Data expressed as n (%) unless otherwise indicated.
Data expressed as mean (SD).
The median QuickDASH score was 4.5 (interquartile range [IQR] 18.2). A total of 17 (33%) patients reported a LANSS score suggestive of neuropathic pain. There was no statistically significant difference in length of follow-up between those with and without neuropathic pain. The median normal hand score was 90 (IQR 23). The NPS was 68 and 96% of patients were satisfied with their surgery. A total of 49 (96%) patients returned to their previous level of work after surgery, taking into account work duties and hours. Two did not return to work for unrelated reasons. Median return to work was 6 weeks (IQR 10).
Five patients (10%) reported complications. Two patients underwent successful excision of painful neuromas after initial conservative treatment, one had surgical correction of a hook nail deformity, one had a single debridement for recurrent infections and one patient underwent a proximal interphalangeal joint fusion.
This paper demonstrates that primary terminalization for acute fingertip injuries is associated with excellent long-term PROMs, high levels of satisfaction and low rate of complications, despite one in three patients reporting long-term neuropathic pain. The main limitations of this study are the retrospective nature and lack of operative data, including the level of the amputation for these patients. While the return to work was rapid after terminalization, the retrospective nature of this study also precludes us from comparing the results with other options of treatment, such as local flap or replantation. Compared to existing literature, however, our findings are strengthened by a comparatively longer-follow up, sample size, and the use of an objective and validated measure of neuropathic pain (Elliot et al., 1997, Hattori et al., 2006).
While this does not represent a comparative study, our results support the decision to undertake this procedure in patients who wish rapid return to work. Previous economic analysis has shown that the greater time off work associated with replantation is associated with a larger economic cost (Sears et al., 2014). As such, the shorter time off work associated with terminalization can be attractive to manual workers, who formed the majority of our patient cohort.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was not sought for the present study because this was a service evaluation of a commonly performed procedure using previously validated outcomes questionnaires. Furthermore, there was no randomization or concealment of treatment. For these reasons, it did not meet the criteria for research and ethics committee review but was registered with the local musculoskeletal quality improvement department. This study was completed in accordance with the Helsinki Declaration as revised in 2013.
Informed consent
All patients gave consent for data collection. This was a service evaluation of a commonly performed procedure using previously validated outcomes questionnaires. Furthermore, there was no randomization or concealment of treatment.