
Abstract
In total, 38 patients with cystic dorsal wrist tumours managed with surgical excision were prospectively followed up for 2 years. Tissue was examined histologically after primary surgery and at recurrence. Two distinct tissue types were found: ganglion cyst and synovial cyst.
Keywords
Cystic soft tissue tumours of the dorsal aspect of the wrist commonly present to hand surgeons. The current literature uses the terms ganglion cyst, synovial cyst and bursal cyst interchangeably, despite their distinct histological characteristics (Giard and Pineda, 2014). There is no good way to differentiate these subtypes clinically.
Surgical excision is associated with high rates of recurrence, and repeat operation is a burden to both the patient and the healthcare system. There are few systematic studies describing the histological structure of these cystic tumours (O’Valle et al., 2014). Various pathological aetiologies have been proposed, but none universally accepted (Minotti and Taras, 2002).
We conducted a prospective study with ethical approval to examine the tissue removed at primary surgery and after reoperation for recurrence. In total, 43 patients presented with cystic soft tissue tumours at the dorsal aspect of the wrist over a 2-year period. None had been formerly treated and all were offered surgery after providing appropriate consent. Five patients did not have surgery after resolution of the tumour. At operation, the cyst and stalk with a portion of capsule was removed for examination by a senior pathologist at a university hospital. Routine microscopy was performed with a haematoxylin and eosin stain, and additional immunohistochemical staining with vimentin (a stromal marker), CD68 (a macrophage marker) and D2-40 (a synovialis cell marker) to characterize the luminal cells if any were present. Patients presenting with recurrence between the planned follow-up at 1 and 2 years, and who opted for revision surgery, had the excised tissue examined in the same way.
Of the 38 patients undergoing surgery, 18 were found to have a cyst with a synovial cell lining at primary surgery. In most cases the synovial cells were lined with a thick, hyaline connective tissue layer which defined a cystic structure. The cyst cells were positive with D2-40, vimentin and occasionally CD68. A total of 15 patients were found to have a ganglion cyst at primary surgery, with tissue of a cystic structure sometimes lined with a single, flattened and uncharacteristic cell layer. The surrounding tissue was fibrous and there were areas of myxoid degeneration. There was no synovial tissue. The cyst walls were negative when stained with D2-40, vimentin and CD68. The remaining five patients had unspecific histopathological diagnoses with no cyst (Figure 1).
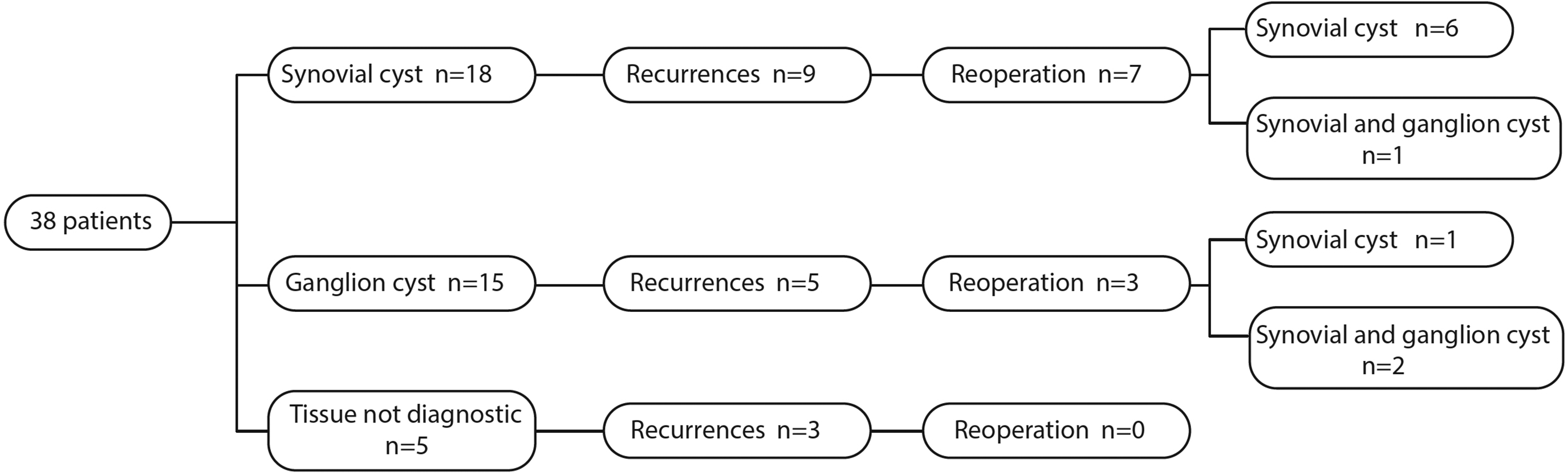
Results of immunohistochemical assessment of tissue removed at primary surgery and after recurrence.
Clinical recurrence was observed in 17 (45%) patients within 1 year of the original surgery. Of these, seven were managed conservatively. The remaining 10 patients had revision surgery. Histological examination of the tissue removed at the time of revision surgery showed synovial tissue in all 10 cases with 3 of the 10 also showing ganglion tissue to be present.
This study has demonstrated two histologically distinct tissue types at primary surgery and the coexistence of both tissue types at recurrence, the recurrence rate being equal in both initial synovial and ganglion groups. The study has its limitations as the sample size is small and therefore there is no clear clinical significance to the findings. It shows a high rate of recurrence, suggesting that open surgery continues to be an ineffective way of managing cystic soft tumours of the dorsal aspect of the wrist.
To facilitate further research on the subject, we suggest that cystic soft tissue tumours of the dorsal aspect of the wrist should be collectively described as such, and the terms ‘ganglion cyst’ or ‘synovial cyst’ only used if they have been examined histologically. This could be helpful in comparing clinical features of these cystic soft tissue tumours such as pain, size, underlying trauma and concurrent wrist pathology, and in attempting to determine recurrence.
Footnotes
Acknowledgements
We would like to thank Lisbeth Vesterløkke, Helle Raagaard Larsen, Nana Vermehren, Guðlaug Rósa Sigurðardóttir, Britt Ebstrup, Gitte Anni Lindy Wallbohm, Dimitar Radev, Camilla Ryge, Merete Juhl Kønig and Xiong Xie for their contribution to the project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from De Videnskabsetiske Komitéer for Region Hovedstaden, Center for Regional Udvikling, Sundhedsforskning og Innovation, Blegdamsvej 60, 1. Sal opgang 94A11, 2100 København Ø, Denmark (project ID: H-16037773; approval number/ID 99523).
Informed consent
Written informed consent was obtained from all participants before the study.