
Abstract
This systematic review and meta-analysis compare the incidences of complications, reoperations and hardware removal between anterior and dorsal plating after corrective osteotomy for dorsally angulated distal radial malunions. A total of 403 patients were included; 253 patients underwent anterior corrective osteotomy and 150 underwent dorsal corrective osteotomy. Mean follow-up was 30 months. Anterior plating was associated with fewer reoperations (9% vs. 28%), less hardware removal (3% vs. 18%) and comparable major complications (5% vs. 6%) compared to dorsal plating. The adjusted model showed a significant reduction (approximately 85%) in the odds of reoperation and hardware removal in the anterior group. There was no difference in major or minor complications between the groups. Surgeons should be fully aware of the increased risks when using dorsal plate fixation after corrective osteotomy for dorsally angulated distal radial malunions.
Introduction
Symptomatic distal radial malunion (DRM) is the most common complication of distal radial fractures that are treated non-operatively. It can result in restricted range of motion, pain, loss of grip strength and suboptimal function (Katt et al., 2020). Patients who experience symptomatic DRM often undergo a corrective osteotomy to restore acceptable radiographic alignment, distal radioulnar joint (DRUJ) congruity and overall functional capacity (Dineen et al., 2019).
Although the benefits of corrective osteotomy have been extensively documented (Mulders et al., 2017; Stirling et al., 2020), there is still no consensus on the most appropriate surgical approach for dorsally angulated DRMs, specifically the choice between dorsal and anterior approaches. This uncertainty is due to the balance between access to the malunion site and the probability of short- and long-term complications with plate placement after an opening wedge osteotomy.
The dorsal approach has several advantages, including a clear view of the deformity and osteotomy site and the ability to access the void created by the opening wedge osteotomy for potential bone graft placement. However, this approach has been associated with a higher risk of extensor tenosynovitis, tendon injuries and of the need for hardware removal due to irritation and limited soft tissue coverage (Sánchez et al., 2005; Schnur and Chang, 2000; Simic et al., 2006).
Historically, anterior plating has been the preferred approach for malunions characterized by excessive apex-anterior angulation due to its relative ease of access and management at the osteotomy site (Shea et al., 1997; Thivaios and McKee, 2003). The use of locking plates has made anterior plating more popular in dorsally angulated DRM corrective osteotomy procedures. This is because it allows for the placement of a fixed-angle device that can effectively reinforce the articular surface placed anteriorly (Koh et al., 2006). In addition, the anterior approach provides improved soft tissue coverage, potentially resulting in a lower incidence of hardware-related complications. However, when applying this approach for an opening wedge osteotomy for a dorsally angulated DRM, there is limited visualization of the osteotomy site before and after correction and an increased risk of median nerve injury, and extensor tendon injury due to screws penetrating dorsally (Arora et al., 2007).
Existing studies regarding the choice between anterior and posterior plating have yielded mixed results and are often hindered by small sample sizes. The aim of this meta-analysis was to compare the complication, revision and hardware removal incidence associated with anterior and dorsal plating in the context of extra-articular corrective osteotomy for dorsally angulated DRMs.
Methods
The meta-analysis was conducted following the Preferred Reporting Items for Systematic reviews and Meta-analysis (PRISMA) guidelines. The Methodological Index for Non-Randomized Studies (MINORS) scale, a validated tool for evaluating non-randomized surgical studies, was used to assess the methodological quality of each study (Slim et al., 2003).
Search strategy
A search was conducted on electronic databases (Embase, MEDLINE, CINAHL and Cochrane) for articles evaluating extra-articular dorsal or anterior corrective osteotomy for dorsally angulated DRMs. The search was limited to articles in the English language from the earliest entry dates to 3 December 2023. The search terms used for each database are described in Online Supplementary Table S1.
Inclusion criteria
The inclusion criteria for studies were as follows: (1) prospective or retrospective study design; (2) patients aged over 18 years; (3) primary treated entity is a dorsally angulated DRM; and (4) surgical intervention is limited to extra-articular osteotomy, either dorsal or anterior with plating. Studies that did not report the incidence of complications or revisions were excluded. Studies involving cadaveric, laboratory or animal subjects were also excluded. Additional details can be found in the PRISMA flow chart (Online Figure S1).
Data extraction
Two independent readers (JP and SK) manually reviewed the retrieved data for both abstract and full-text information. Relevant data were extracted and compiled into a Comma-Separated Values (CSV) file. The data extracted from the study included the first author’s name, type of study, date of publication, country of origin, number of patients in each study, patients’ characteristics, number of patients in each surgical intervention, complications, reoperation incidences, indication for reoperations, hardware removal, and the presence and type of bone graft used. Disagreements were resolved through discussion.
Outcomes
The co-primary outcomes measured were the occurrence of major complications, minor complications, reoperations and hardware removal. Complications were classified as major or minor. Major complications included infection, nonunion, bone graft failure, adhesions requiring tenolysis, hardware failure, hardware loosening, intraoperative tendon injury, complex regional pain syndrome and other fixation failure. Minor complications included pain and stiffness not requiring surgery, transient median nerve neuropathy not requiring surgery and continued bone graft donor site pain. Hardware removals were performed because of postoperative tendon irritation, prominent hardware or wrist discomfort.
Statistics
Descriptive statistics were calculated for the variables collected and reported as means with standard deviations (SD) for continuous variables and counts with proportions for categorical variables. A meta-analysis of proportions using a generalized linear mixed-model approach with logit transformation was used to pool proportions across included studies. Forest plots and pooled estimates with 95% confidence intervals (CI) were calculated for each outcome. For each outcome, we built a multivariable meta-analysis regression model using the ‘metareg’ function, which was adjusted for selected potential confounders. The results of each multivariable model were reported as adjusted odds ratios (OR) with 95% CIs. Heterogeneity was assessed using Q-tests and I 2 statistics. If p ≤ 0.1 or I 2 > 50%, significant heterogeneity was assumed, and the random-effects model was used to evaluate the system. Conversely, if p > 0.1 or I 2 < 50%, the common-effects model was used.
Results
A total of 1789 studies was found. After a title and abstract screening, 60 studies remained. After a full-text review, 19 studies (15 retrospective and 4 prospective) met the eligibility criteria and were included in the meta-analysis. Further details and characteristics are presented in Online Figure S1.
Patient characteristics
In total, 403 patients (65% women; age range 32–61 years) from 19 studies were included. Among them, 253 (63%) underwent anterior osteotomy and 150 (37%) underwent dorsal osteotomy. The mean time from initial injury to osteotomy was 10 months (range 2–24) and the mean preoperative dorsal angulation was 24° (SD 7°). The mean follow-up was 30 months (SD 26, range 8–84). Additional characteristics and perioperative parameters are shown in Table 1 and Online Table S2.
Included studies demographic and perioperative variables.
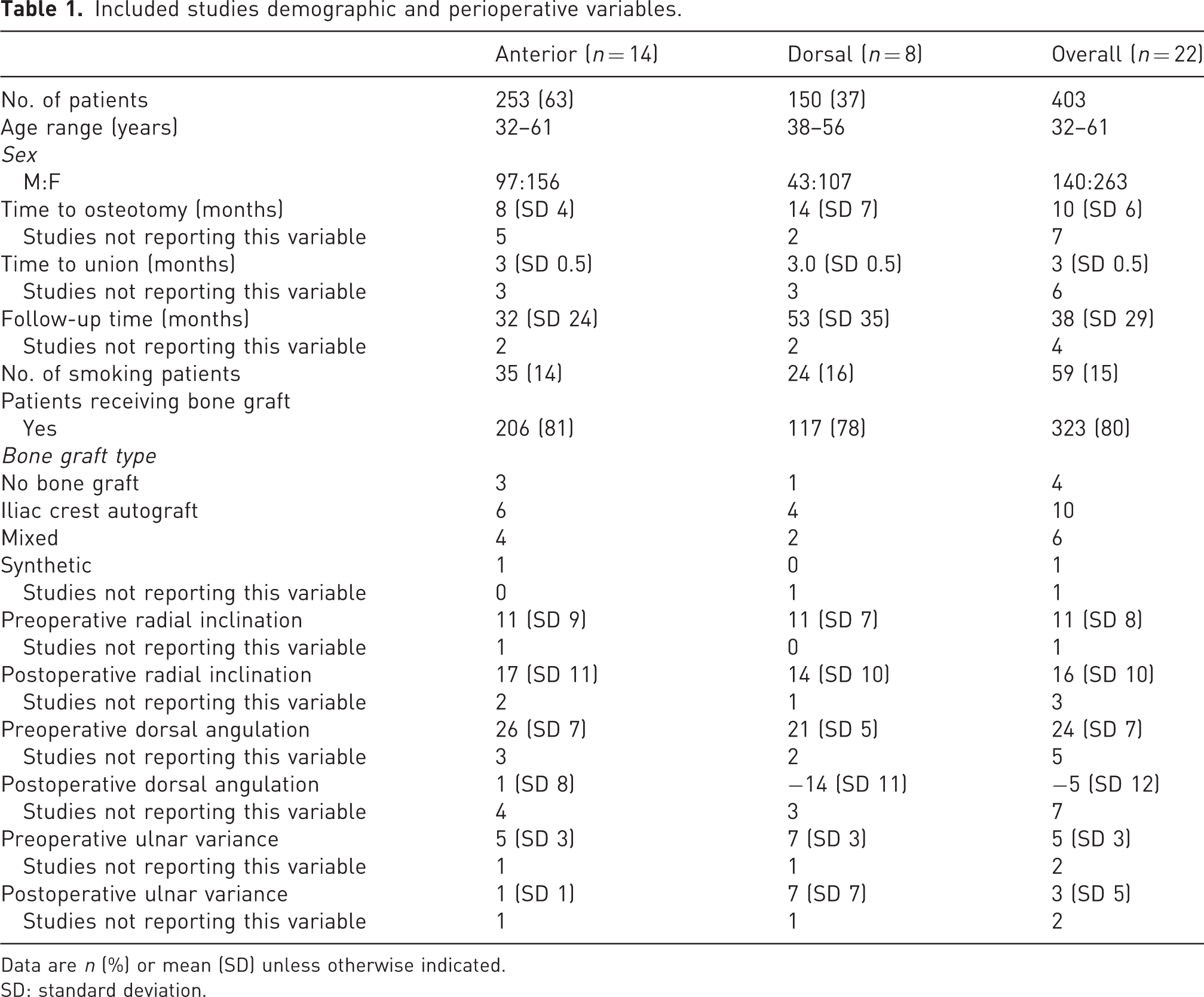
Data are n (%) or mean (SD) unless otherwise indicated.
SD: standard deviation.
Implants
The included studies describe the use of both anterior and dorsal plating techniques, using both locking and non-locking plates. All studies in the anterior plating group used locking plates only. Regarding dorsal plating, the specifics of the plates used varied across studies. Regarding dorsal plating, three studies did not disclose the type of dorsal plate implemented (Elmi et al., 2014; Kovjanić et al., 2010; Krukhaug and Hove, 2007), three studies reported employing exclusively non-locking plates (Oka et al., 2018; Ring et al., 2002; Rothenfluh et al., 2013), one study documented the utilization of both locking and non-locking plates (Schurko et al., 2020) whereas Tiren and Vos (2014) exclusively mentioned the use of locking plates.
Three studies specifically described using low-profile plates in the dorsal group, as defined by the manufacturer’s specifications (Oka et al., 2018; Schurko et al., 2020; Tiren and Vos, 2014).
Major complications
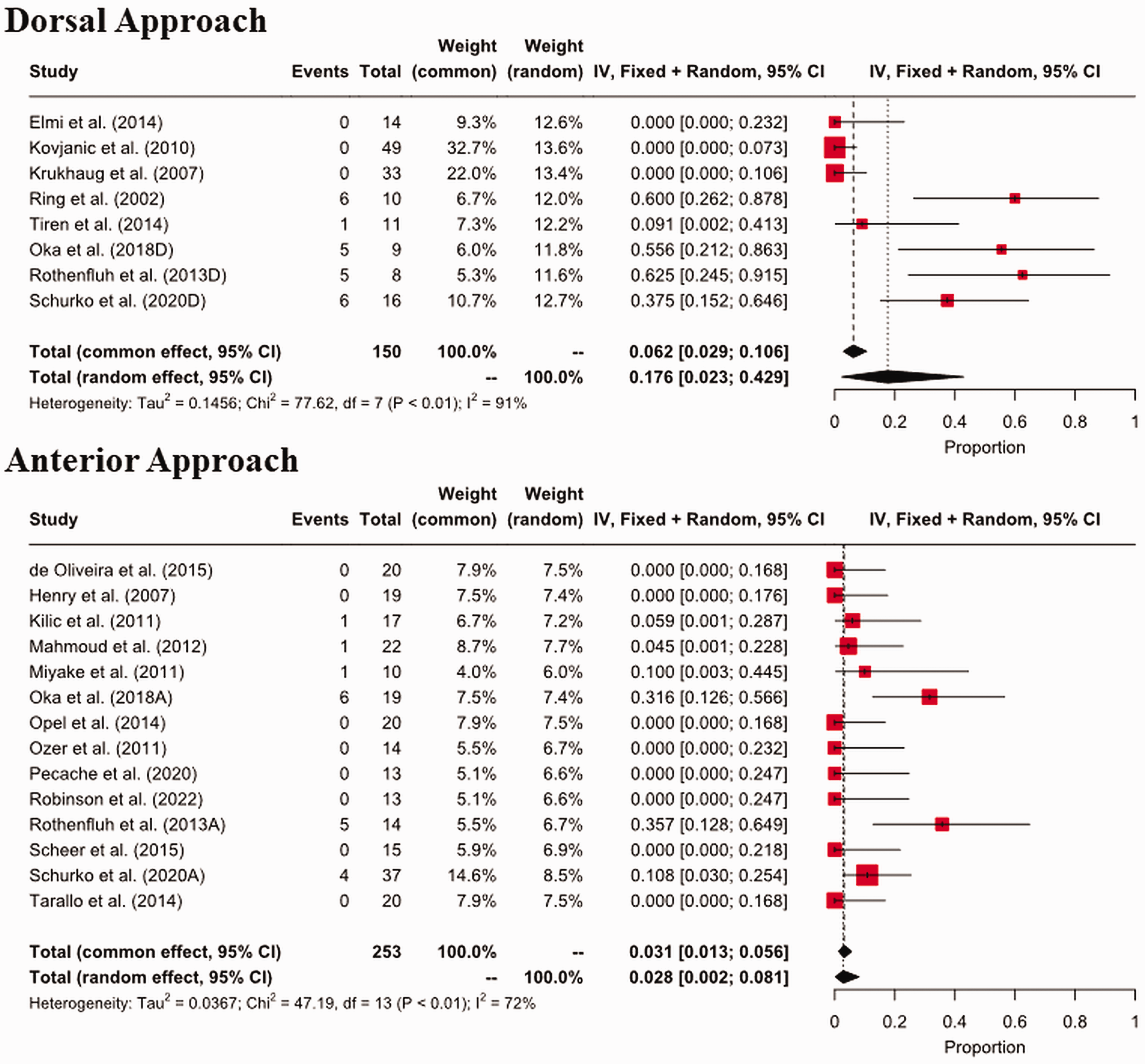
In total, 13 studies reported major complications, including bone graft-related complications in 10 of 35 patients, hardware/fixation failure in 6 of 35 patients and nonunion in 5 of 35 patients. The included studies for each surgical group were heterogeneous, thus random effects models were used (p < 0.1, I 2 > 50%). The pooled estimate for the incidence of major complications after corrective osteotomy with dorsal plating was 6% (95% CI: 2 to 13), compared to 5% (95% CI: 2 to 11) after corrective osteotomy using anterior plating (Figure 1). In the multivariable meta-regression model adjusted for age, follow-up time, preoperative dorsal angulation and time to osteotomy from original injury showed comparable odds for the occurrence of major complications in the anterior plating group compared to the dorsal plating group (OR 0.46, 95% CI: 0.1 to 2) (Table 2).
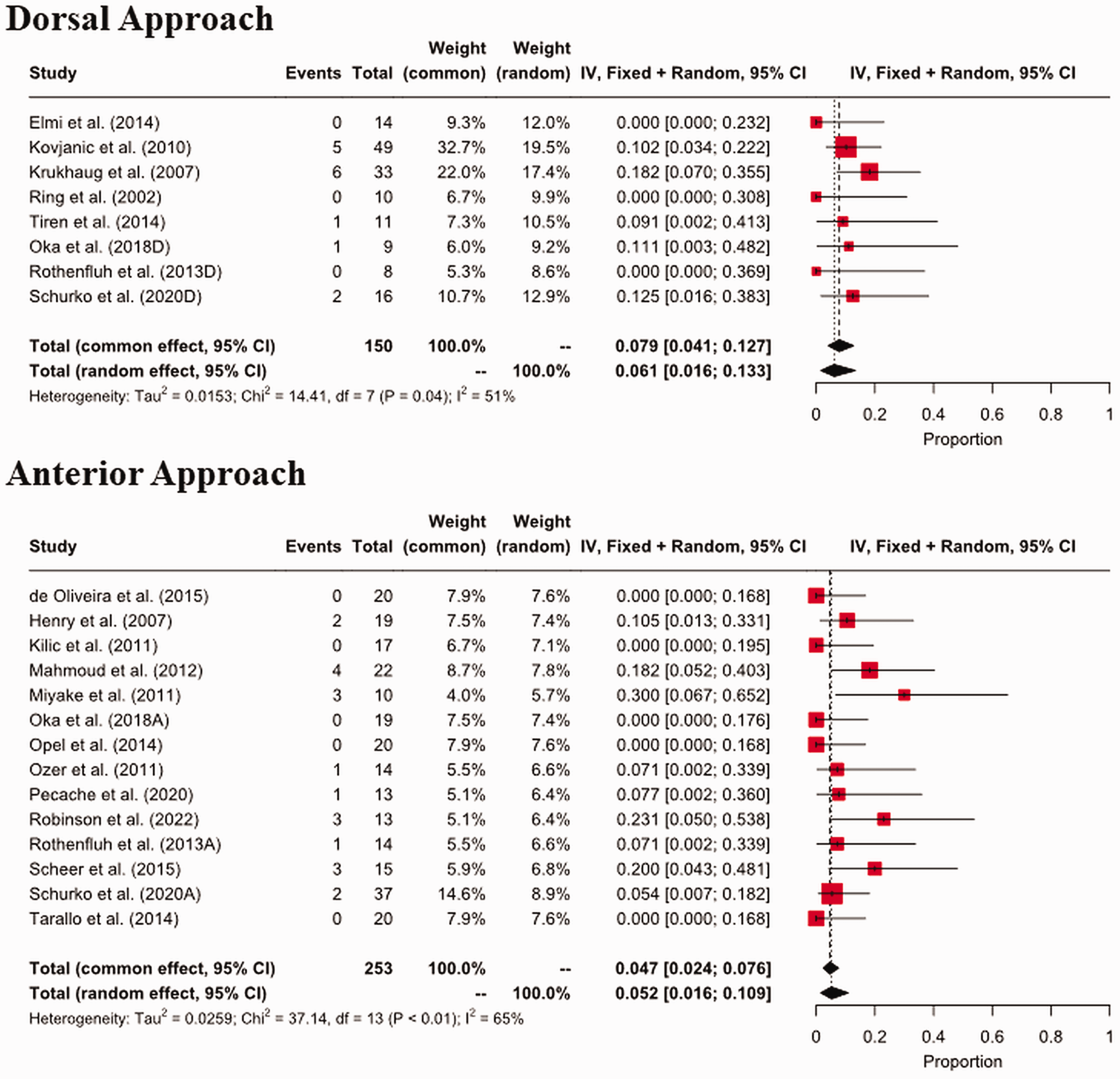
Forest plots for major complications.
Outcomes based on surgical approach with calculated adjusted odds ratios.
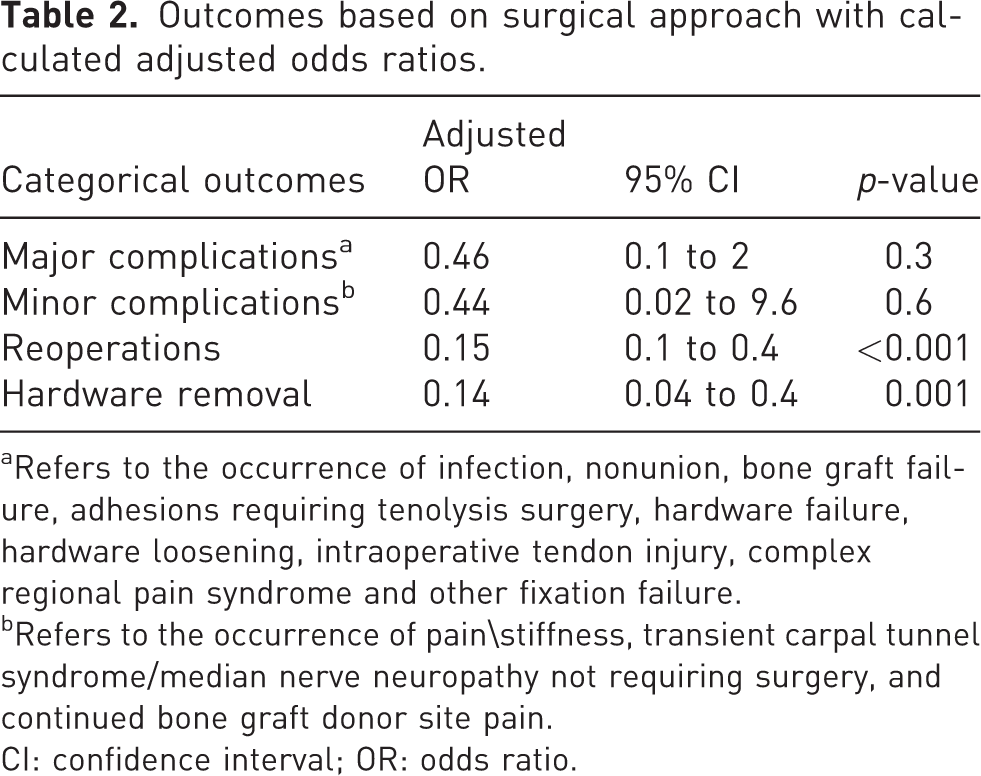
Refers to the occurrence of infection, nonunion, bone graft failure, adhesions requiring tenolysis surgery, hardware failure, hardware loosening, intraoperative tendon injury, complex regional pain syndrome and other fixation failure.
Refers to the occurrence of pain\stiffness, transient carpal tunnel syndrome/median nerve neuropathy not requiring surgery, and continued bone graft donor site pain.
CI: confidence interval; OR: odds ratio.
Minor complications
Six studies reported minor complications, with the most common being transient median nerve neuropathy (3/8). The included studies for each surgical group were homogeneous, thus common effects models were used (p > 0.1, I 2 < 50%). The pooled estimates for minor complications following dorsal plating were 0.3% (<0.1%–2%) compared to 0.7% (<0.1%–2%) for the anterior plating group (Online Figure S2) The analysis showed no significant difference in minor complications between the surgical groups in both the crude and multivariable adjusted models (Table 2).
Reoperations
Among the reviewed literature, 14 studies elucidated the requirement for revision surgeries, predominantly ascribed to complications associated with the hardware. Specifically, the primary indications for these revision procedures were tendon irritation and wrist discomfort, constituting 38% of the incidents necessitating reoperation. The included studies for each surgical group were heterogeneous, thus random effects models were used (p < 0.1, I 2 > 50%) (Figure 2). The dorsal plating group had a higher proportion of reoperation (28%; 95% CI: 11 to 49) compared to the anterior group (9%; 95% CI: 3 to 18). In the multivariable meta-regression model, adjusting for age, follow-up time, preoperative dorsal angulation and time to osteotomy from original injury, the anterior osteotomy group demonstrated significantly reduced odds of reoperation compared to the dorsal group (OR 0.15, 95% CI: 0.1 to 0.4) (Table 2).
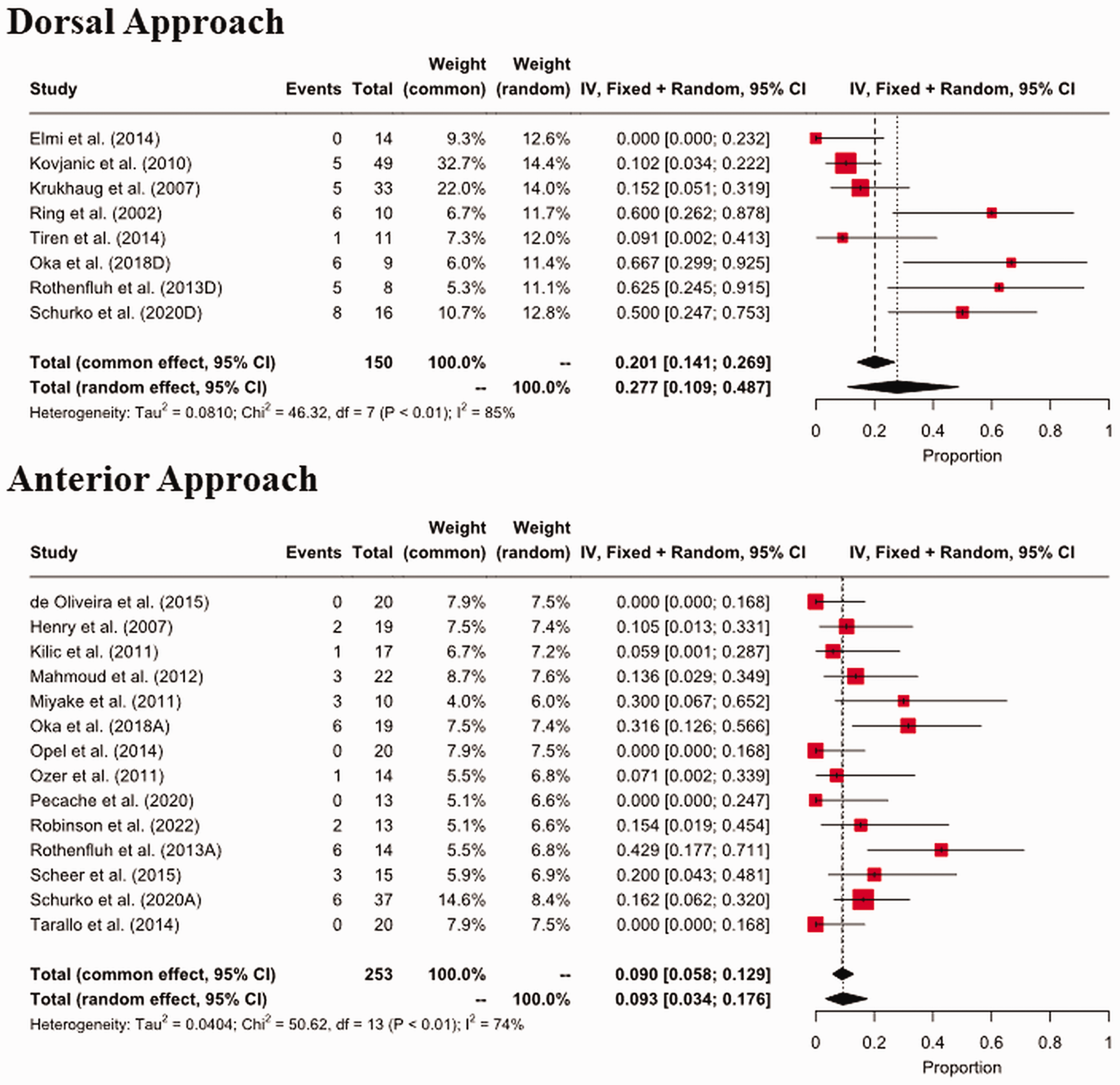
Forest plots for reoperations.
Hardware removal
Eight studies reported on hardware removal procedures. The included studies for each surgical group were heterogeneous, thus random effects models were used (p < 0.1, I 2 > 50%). (Figure 3) The incidence of hardware removal was nearly six times higher in the dorsal plating group (18%; 95% CI: 2 to 43) compared to the anterior group (3%; 95% CI: 0.2 to 8). This difference remained statistically significant in the multivariable adjusted model with 86% less odds of plate removal in the anterior group (OR 0.14, 95% CI: 0.04 to 0.4) (Table 2).
Forest plots for hardware removal.
Dorsal plate selection
Five studies provided information on dorsal plate selection for patients, and three, including 36 patients, explicitly incorporated ‘low-profile plates’ as defined by the manufacturer’s specifications (Oka et al., 2018; Schurko et al., 2020; Tiren and Vos, 2014). Among these 36 patients, there were 6 major complications and 12 hardware removals.
Discussion
This meta-analysis shows that patients undergoing an anterior corrective osteotomy with plate fixation for a dorsally angulated DRM have significantly reduced odds of reoperation and hardware removal compared to a dorsal corrective osteotomy with plate fixation. Both surgical techniques had similar odds of major and minor complications.
The increased incidence of extensor tendon-related complications associated with dorsal plating of the distal radius was previously attributed to the use of older generation plates, which were bulky and did not anatomically conform to the irregular shape of the dorsal aspect of the distal radius (Wei et al., 2013). Yu et al. (2011) suggested that the new generation of ‘low-profile’ plates would solve this problem. In this meta-analysis, data from five studies detailed the types of plates used for dorsal plating, with three studies specifically documenting the use of ‘low-profile’ plates as specified by the manufacturer. When examining the data related to the use of low-profile plates in dorsal plating, a slightly higher incidence of complications (6/36) and plate removal (12/36) was reported. These findings support the notion that, despite the use of ‘low-profile’ plating, the close anatomical relationship between the extensor tendons and the dorsal distal radius, as well as the restricted space of the extensor compartments, are likely to be the major factors contributing to the increased susceptibility to tenosynovitis and hardware-related complications. Based on the results of this study, susceptibility appears to be independent of the specific type of hardware used.
Anterior plating also has its limitations, which include the potential for tendon irritation, particularly of the flexor tendons if the plate is placed too distally. To reduce this risk, it is advisable to place the plate proximal to the watershed line (Orbay, 2005). In addition, protrusion of the distal screws beyond the dorsal cortex can result in injury to the extensor tendons, with the extensor pollicis longus tendon being the most commonly affected (Arora et al., 2007; Sato et al., 2018). Attritional rupture of multiple extensor tendons along the extensor pollicis longus has also been reported lately (Paul et al., 2023). To address these concerns, various intraoperative fluoroscopic views, such as the dorsal horizon (DH) and carpal shoot-through (CST) views, have been developed to detect screw protrusion on the dorsal side (Joseph and Harvey, 2011; Marsland et al., 2014).
Median nerve neuropathy and the development of carpal tunnel syndrome as a result of forceful retraction and/or dissection during the anterior approach is a less common complication that has warranted a carpal tunnel release either at the time of the osteotomy or later (Rein et al., 2007). In a recent cadaveric study, Heifner et al. (2023) evaluated the differences in distal exposure between the extended flexor carpi radialis (EFCR) approach and the traditional Henry’s approach. Specifically, the study quantified the force on the median nerve and flexor tendons required to achieve a standardized 60° angle of retraction. The EFCR approach required significantly less retraction force to achieve superior distal exposure. These findings provide support the consideration of the EFCR approach in anterior distal radial corrective osteotomies to reduce the risk of traction-related injuries (Heifner et al., 2023).
The main limitation of our study is the variation in sample size between the included studies, which may introduce bias. To minimize this effect, the data were pooled in a meta-analysis model that adjusted for the weight of each study sample. Although a meta-regression model was built to adjust for several patient demographic and perioperative confounders, several unadjusted variables may have confounded the results. Furthermore, the inclusion of studies conducted at different centres over a wide range of years, with different surgical protocols, plate designs and levels of surgical experience, could potentially affect the overall consistency and generalizability of the results.
Finally, this study cannot account for specific variations in surgical technique. The potential for hardware complications can be mitigated with modifications to each exposure. For example, in the anterior approach, plate placement proximal to the watershed line and use of newer hardware designed to contour appropriately in this area may offer protection from flexor tendon irritation. In addition, repair of the pronator quadratus may provide a protective interface to minimize flexor tendon adhesions, tenosynovitis and attritional rupture. For the dorsal approach, the transposition of a portion of the extensor retinaculum deep to the extensor tendons may prevent plate irritation (Devaux et al., 2018). Oka et al. (2018) used this technique to protect the extensor tendons, while Tiren and Vos (2014) used the extensor retinaculum to protect the extensor pollicis longus tendon alone.
This study shows that anterior plating for dorsally angulated distal radial osteotomy significantly reduces the odds of reoperation and hardware removal compared to dorsal plating, even after careful adjustment for potential confounders.
Supplemental Material
sj-pdf-1-jhs-10.1177_17531934241254962 - Supplemental material for A meta-analysis comparing complications of anterior versus dorsal osteotomy and plating for distal radial malunions
Supplemental material, sj-pdf-1-jhs-10.1177_17531934241254962 for A meta-analysis comparing complications of anterior versus dorsal osteotomy and plating for distal radial malunions by Ahmad Essa, Ryan Paul, Shawn Khan, Erez Avisar, Andrea Chan and Jonathan Persitz in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-2-jhs-10.1177_17531934241254962 - Supplemental material for A meta-analysis comparing complications of anterior versus dorsal osteotomy and plating for distal radial malunions
Supplemental material, sj-pdf-2-jhs-10.1177_17531934241254962 for A meta-analysis comparing complications of anterior versus dorsal osteotomy and plating for distal radial malunions by Ahmad Essa, Ryan Paul, Shawn Khan, Erez Avisar, Andrea Chan and Jonathan Persitz in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-3-jhs-10.1177_17531934241254962 - Supplemental material for A meta-analysis comparing complications of anterior versus dorsal osteotomy and plating for distal radial malunions
Supplemental material, sj-pdf-3-jhs-10.1177_17531934241254962 for A meta-analysis comparing complications of anterior versus dorsal osteotomy and plating for distal radial malunions by Ahmad Essa, Ryan Paul, Shawn Khan, Erez Avisar, Andrea Chan and Jonathan Persitz in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-4-jhs-10.1177_17531934241254962 - Supplemental material for A meta-analysis comparing complications of anterior versus dorsal osteotomy and plating for distal radial malunions
Supplemental material, sj-pdf-4-jhs-10.1177_17531934241254962 for A meta-analysis comparing complications of anterior versus dorsal osteotomy and plating for distal radial malunions by Ahmad Essa, Ryan Paul, Shawn Khan, Erez Avisar, Andrea Chan and Jonathan Persitz in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-5-jhs-10.1177_17531934241254962 - Supplemental material for A meta-analysis comparing complications of anterior versus dorsal osteotomy and plating for distal radial malunions
Supplemental material, sj-pdf-5-jhs-10.1177_17531934241254962 for A meta-analysis comparing complications of anterior versus dorsal osteotomy and plating for distal radial malunions by Ahmad Essa, Ryan Paul, Shawn Khan, Erez Avisar, Andrea Chan and Jonathan Persitz in Journal of Hand Surgery (European Volume)
Footnotes
Declaration of competing interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.