
Abstract
We examined whether treatment utilization for Dupuytren’s contracture varied with the presence of adverse socioeconomic determinants of health in the United States. After propensity score matching, the presence of adverse socioeconomic determinants of health was associated with decreased treatment utilization.
Treatment utilization in Dupuytren’s contracture is sensitive to patient factors, including socioeconomic determinants of health (SDOH), since there is no clear best treatment. Although increasing social deprivation was associated with increased incidence of surgery for Dupuytren’s contracture in the UK (Stirling et al., 2020), this effect may differ in the United States population, given the differences in healthcare systems and socioeconomic environments.
This study evaluated whether treatment utilization for Dupuytren’s contracture varies with the presence of adverse SDOH factors in the United States population. Using the PearlDiver Mariner Patient Claims Database, a large administrative database of insurance claims from over 165 million American patients, we identified patients diagnosed with Dupuytren’s contracture between 2012 and 2020. Patients were required to be actively enrolled in the database for at least 1 year before and 2 years after diagnosis. Patients with private, Medicare Advantage and Medicaid managed care plans were included. In the Medicare Advantage and Medicaid managed care plans, the American government pays a per-capita rate to a private insurer to manage care for eligible patients. We identified adverse SDOH factors across five domains: economic; educational; social; healthcare; and environmental. This algorithm has previously been used to measure SDOH in administrative claims data (Agarwal et al., 2023). Patients were divided into cohorts; those with at least one adverse SDOH factor and those without. Each patient in the adverse SDOH group was propensity score-matched with a patient in the non-adverse group on a 1:1 ratio based on age, sex, geographic region, insurance plan and Elixhauser co-morbidity score with a calliper width of 0.2. We then used a multivariable logistic regression model to adjust for differences in age and insurance plan between the groups. We identified patients in each cohort who received percutaneous needle aponeurotomy (PNA), open fasciotomy, limited fasciectomy or collagenase injection within 2 years after diagnosis, measured every 3 months.
After propensity score matching, cohorts consisting of patients with no adverse SDOH factor (n = 32,973) or at least 1 adverse SDOH factor (n = 32,973) were obtained. At 2 years after diagnosis, 5989 (18.2%) patients without adverse SDOH had received treatment compared with 4829 (14.6%) patients with adverse SDOH (p < 0.001). Fewer patients with at least one adverse SDOH factor underwent collagenase injection, open fasciotomy or fasciectomy compared with patients with no adverse SDOH factors across all timepoints (Figure 1). After adjustment for potential confounding factors, patients with adverse SDOH experienced a decreased odds of treatment for Dupuytren’s contracture at all timepoints, including PNA, collagenase injection, open fasciotomy and fasciectomy. At 24 months after diagnosis, the adjusted odds ratios for treatment utilization in patients with at least one adverse SDOH factor compared to those without were 0.86 (95% confidence interval [CI]: 0.77 to 0.97) for PNA, 0.76 (95% CI: 0.66 to 0.87) for open fasciotomy, 0.75 (95% CI: 0.72 to 0.79) for fasciectomy and 0.88 (95% CI: 0.81 to 0.96) for collagenase injections.
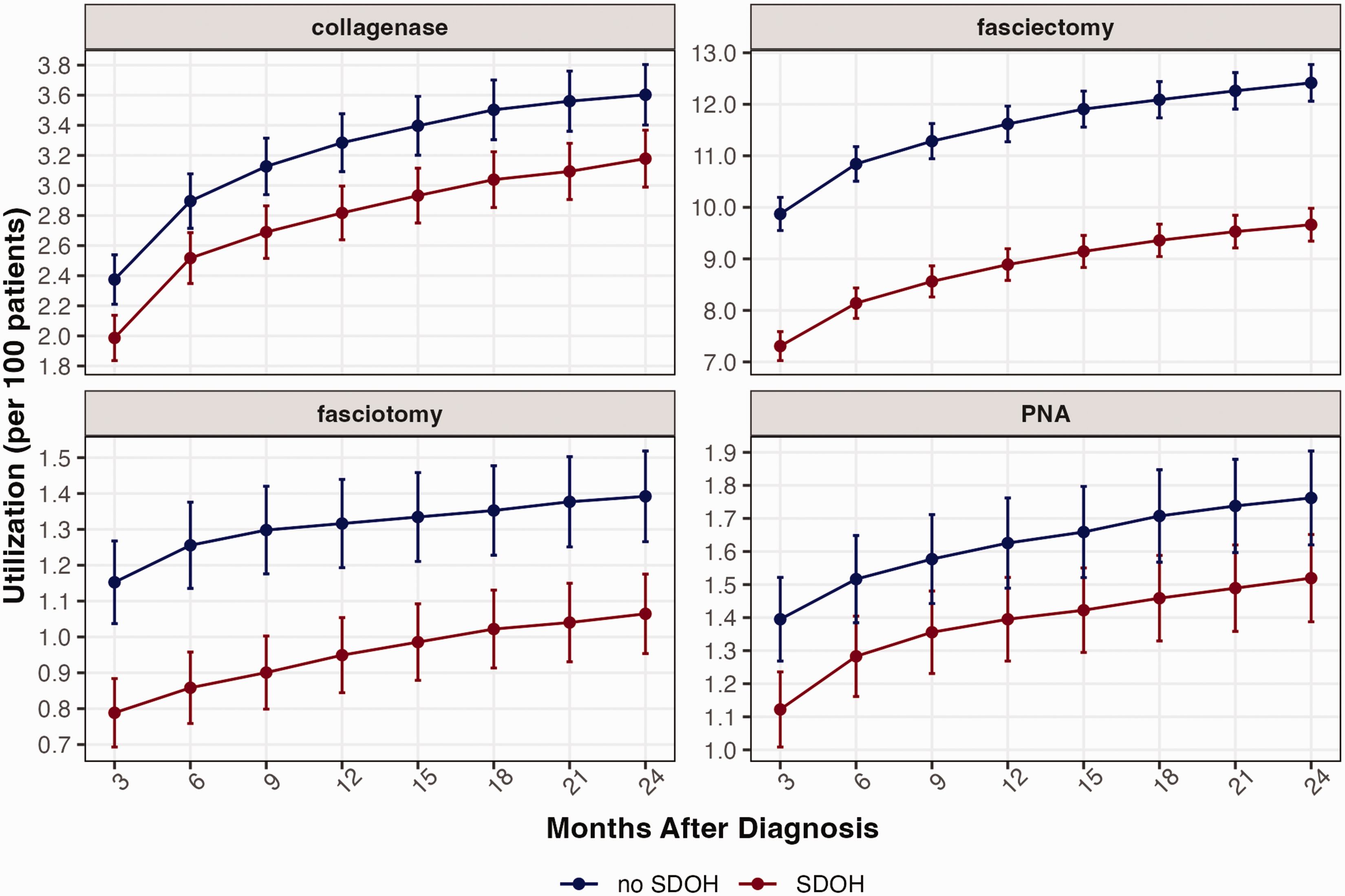
Cumulative incidence of individual Dupuytren’s contracture treatments by time period (treatment utilization per 100 patients with Dupuytren’s contracture). PNA: percutaneous needle aponeurotomy; SDOH: socioeconomic determinants of health.
Due to its elective nature and variety of discretionary treatment options, Dupuytren’s contracture provides a valuable opportunity for evaluating variations in care based on SDOH. Socioeconomically disadvantaged patients may face barriers to care in the United States. Potential mechanisms include difficulty obtaining appointments, work restrictions, prohibitive costs or limitations from insurance. Our findings contrast with a prior study in a UK population, in which socioeconomic deprivation was associated with increased incidence of surgery for Dupuytren’s contracture (Stirling et al., 2020). This discrepancy could be attributable to the different funding systems between these countries. In a government-sponsored universal healthcare system, socioeconomically disadvantaged patients face few financial barriers to care, leading to a higher utilization of care for conditions where treatment options are choice sensitive. In contrast, patients with limited access to care due to socioeconomic factors in non-universal healthcare systems may reduce care utilization.
Several strategies may reduce the impact of adverse SDOH factors in non-universal healthcare systems. Given that the costs of treatment for Dupuytren’s contracture vary (Yoon et al., 2020), patients should be well informed about the financial aspects of treatment, including the out-of-pocket component. Financial counselling can be provided for disadvantaged patients to mitigate the economic impact of care. Since treatment choice is based on personal preference, decision aids outlining the benefits and risks of all treatments can be useful in order to facilitate shared decision-making (Making a decision about: Dupuytren’s contracture, 2022). Furthermore, SDOH can be integrated into clinical decision support tools across health systems, where patients’ adverse SDOH factors can be addressed during shared decision-making.
The present study has some limitations. Our findings rely on complete and accurate coding, an assumption inherent to administrative database analyses. Patients who did not seek medical evaluation for Dupuytren’s contracture at all due to socioeconomic barriers were not captured, potentially underestimating the true disparity. Due to limitations of claims data, we were unable to assess severity of contracture at presentation, although patients with adverse SDOH might be expected to present at a more advanced disease stage due to barriers to care. Although the treatment decision for Dupuytren’s contracture is sensitive to patient preference, we assumed that systematic differences in preferences independent from SDOH are unlikely to exist between matched cohorts. Further, patients with adverse SDOH had lower utilization of all interventions, suggesting that a true disparity exists.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethical approval
Because this study used only deidentified data, this study was exempt from institutional review board approval.
Informed consent
All procedures were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008(5).