
Abstract
Wrist arthrodesis in spastic patients combined with proximal row carpectomy and ostectomy of the distal radius to allow a position of slight flexion (COF technique) results in a better outcome when compared to arthrodesis after proximal row carpectomy only technique.
Tranchida and Van Heest (2020) viewed the wrist flexion/clenched fist deformity in spastic patients as either mild or advanced. Mild cases could be managed with tendon surgery. Advanced cases require wrist arthrodesis with or without tendon surgery. The surgical management for advanced wrist/finger flexion deformity varies among different authors (Supplementary Table S1). Our approach for this problem depends on the severity of the deformity (Supplementary Table S2).
Before the year 2020, we had been performing wrist arthrodesis with proximal row carpectomy (PRC) for moderate cases as the first step, with soft tissue rebalancing procedures done as a secondary procedure tailored to the residual finger/thumb deformity. The technique before 2020 involved performing a PRC first, followed by removal of the articular surfaces of the capitate and hamate. The head of the capitate was not excised and was left protruding as a peg. The articular surface of the distal radius was then removed and the central part of the medullary cavity of the radius was curetted to provide a slot for the head of the capitate to sit in. Internal fixation was done using a straight wrist fusion plate. The curetted bone from the distal radius was impacted around the capitate.
Since 2020, the author has modified the wrist arthrodesis technique by combining PRC, removing a segment of the distal radius (ostectomy) and positioning the wrist in 10–20 degrees of flexion (COF technique) (Figure 1). After performing the PRC and the preparation of the capitate/hamate as previously described, ostectomy of the distal radius was performed just proximal to Lister’s tubercle using a saw. This created a wide medullary cavity in the distal radius. The slot in the distal radius for the capitate to sit in was made towards the dorsal aspect of the medullary cavity of the radius. This allowed the wrist to be positioned in 10–20 degrees of flexion. The ulnar head was partially resected to prevent distal ulna becoming too prominent. A straight wrist fusion plate was used for internal fixation. The wrist flexion position created a gap between the plate and the wrist fusion site, which was accepted. The wrist was immobilized for 6 weeks in a below-elbow cast in both PRC and COF groups.
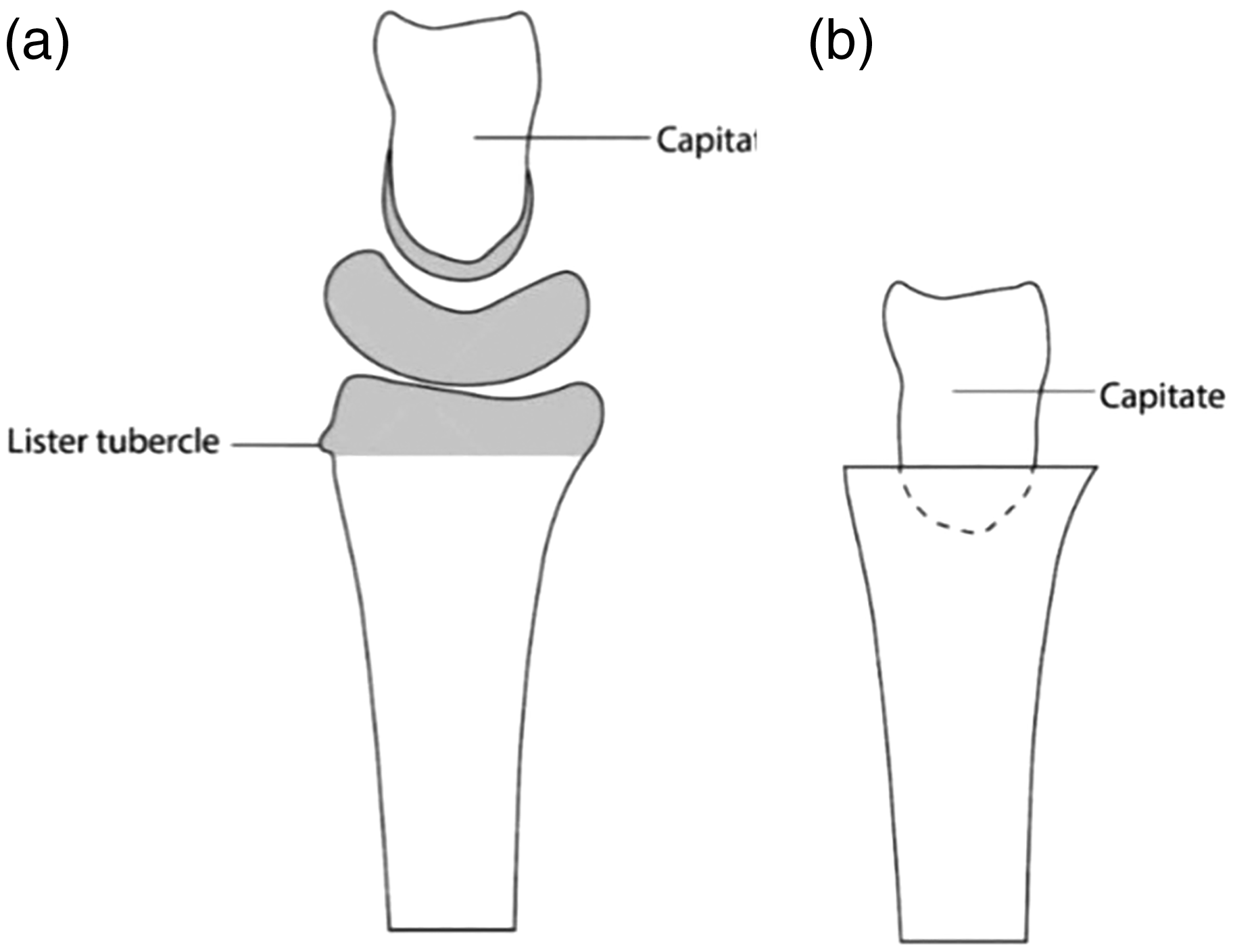
Illustration of the technique of proximal row carpectomy, ostectomy of distal radius and positioning of capitate into distal radius to achieve flexion of wrist prior to fusion. (a) Lateral view illustration showing the shaded areas that are excised and (b) the head of the capitate is inserted into the slot in the medullary cavity of the distal radius.
We conducted a retrospective comparative study of 10 patients who underwent wrist arthrodesis using the PRC technique (operated before the year 2020) and 10 patients who underwent wrist arthrodesis using the COF technique (operated from the year 2020 onwards). Ethical approval was obtained from the Research Committee at the author’s private clinic. The inclusion criteria used for both groups were as follows: consecutive patients with moderate spasticity; those who had no prior soft tissue procedures and no simultaneous soft tissue rebalancing procedures performed at the time of arthrodesis; adequate data were available for review; and those who had a minimum follow-up for 1 year. Hand function was assessed before and after surgery using the functional scoring system shown in the supplementary Table S3. The number of patients requiring secondary finger flexor tendon lengthening was also documented. Mann–Whitney test was used to compare the functional scores, and Fisher’s exact test was used to compare the need for secondary finger flexor tendon lengthening. P-values <0.05 were considered significant.
Both groups were similar in demographics (Supplementary Table S4). No postoperative complications were encountered. The follow-up range was 14–25 months (mean 18 months) in the PRC group and 13–26 months (mean 18 months) in the COF group.
Bone union was obtained in all patients. The mean preoperative functional scores between both groups were not significantly different indicating that the degree of deformity (before the arthrodesis) was similar in both groups (Supplementary Table S5). However, the postoperative scores were significantly better in the COF group indicating a better functional outcome (p = 0.011) (Supplementary Table S6, Figure S1 and S2). Five patients in the PRC group required flexor tendon lengthening as a secondary procedure while none of the patients in the COF group required this, which was statistically significant (p = 0.033).
Performing a PRC before wrist fusion has become the standard of care in spastic patients, as it allows shortening of the wrist and helps to relieve some of tension across the flexor tendons. In a biomechanical study, Carrazana-Suárez et al. (2022) found that the mean digit flexor tendon resting length increment was 1.88 cm across all flexor tendons after the PRC technique of wrist arthrodesis. Combining the PRC with an ostectomy of the distal radius and positioning the wrist in slight flexion in the COF technique will allow further reduction in the tension across the flexor tendons and improve outcomes as confirmed in our study.
Supplemental Material
sj-zip-1-jhs-10.1177_17531934241275478 - Supplemental material for Wrist arthrodesis in flexed position combined with proximal row carpectomy and ostectomy of the distal radius for spastic patients
Supplemental material, sj-zip-1-jhs-10.1177_17531934241275478 for Wrist arthrodesis in flexed position combined with proximal row carpectomy and ostectomy of the distal radius for spastic patients by Mohammad M. Al-Qattan in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-zip-2-jhs-10.1177_17531934241275478 - Supplemental material for Wrist arthrodesis in flexed position combined with proximal row carpectomy and ostectomy of the distal radius for spastic patients
Supplemental material, sj-zip-2-jhs-10.1177_17531934241275478 for Wrist arthrodesis in flexed position combined with proximal row carpectomy and ostectomy of the distal radius for spastic patients by Mohammad M. Al-Qattan in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-3-jhs-10.1177_17531934241275478 - Supplemental material for Wrist arthrodesis in flexed position combined with proximal row carpectomy and ostectomy of the distal radius for spastic patients
Supplemental material, sj-pdf-3-jhs-10.1177_17531934241275478 for Wrist arthrodesis in flexed position combined with proximal row carpectomy and ostectomy of the distal radius for spastic patients by Mohammad M. Al-Qattan in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-4-jhs-10.1177_17531934241275478 - Supplemental material for Wrist arthrodesis in flexed position combined with proximal row carpectomy and ostectomy of the distal radius for spastic patients
Supplemental material, sj-pdf-4-jhs-10.1177_17531934241275478 for Wrist arthrodesis in flexed position combined with proximal row carpectomy and ostectomy of the distal radius for spastic patients by Mohammad M. Al-Qattan in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-5-jhs-10.1177_17531934241275478 - Supplemental material for Wrist arthrodesis in flexed position combined with proximal row carpectomy and ostectomy of the distal radius for spastic patients
Supplemental material, sj-pdf-5-jhs-10.1177_17531934241275478 for Wrist arthrodesis in flexed position combined with proximal row carpectomy and ostectomy of the distal radius for spastic patients by Mohammad M. Al-Qattan in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-6-jhs-10.1177_17531934241275478 - Supplemental material for Wrist arthrodesis in flexed position combined with proximal row carpectomy and ostectomy of the distal radius for spastic patients
Supplemental material, sj-pdf-6-jhs-10.1177_17531934241275478 for Wrist arthrodesis in flexed position combined with proximal row carpectomy and ostectomy of the distal radius for spastic patients by Mohammad M. Al-Qattan in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-7-jhs-10.1177_17531934241275478 - Supplemental material for Wrist arthrodesis in flexed position combined with proximal row carpectomy and ostectomy of the distal radius for spastic patients
Supplemental material, sj-pdf-7-jhs-10.1177_17531934241275478 for Wrist arthrodesis in flexed position combined with proximal row carpectomy and ostectomy of the distal radius for spastic patients by Mohammad M. Al-Qattan in Journal of Hand Surgery (European Volume)
Supplemental Material
sj-pdf-8-jhs-10.1177_17531934241275478 - Supplemental material for Wrist arthrodesis in flexed position combined with proximal row carpectomy and ostectomy of the distal radius for spastic patients
Supplemental material, sj-pdf-8-jhs-10.1177_17531934241275478 for Wrist arthrodesis in flexed position combined with proximal row carpectomy and ostectomy of the distal radius for spastic patients by Mohammad M. Al-Qattan in Journal of Hand Surgery (European Volume)
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was obtained from Medical Consultants Polyclinic, Riyadh, Saudi Arabia.
Informed consent
Informed consent was not required (retrospective study) and the illustrations do not identify the patients.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.