
Abstract
We compared the outcomes of two groups of patients with scaphoid nonunion treated with arthroscopic cancellous bone grafting. In group 1, K-wires were introduced beforehand and in group 2 after debridement and packing bone grafts in the nonunion site. Our hypothesis was that the percentage of unions would be higher in group 2. We conducted a retrospective, single-centre comparative study of two consecutive series of patients. Seventeen patients in group 1 were operated between 2011 and 2015 and 25 patients in group 2 between 2015 and 2022. At 3 months, there was already a significant difference in consolidation, with three fractures united in group 1 and 21 in group 2. At 6 months, 10 patients (59%) united in group 1 and 24 (96%) in group 2. Debridement of the nonunion site without K-wires in place may allow a more thorough debridement and extensive filling of the defect with bone graft. If an arthroscopic technique is used for scaphoid nonunion, we do not recommend prior fixation with K-wires.
Introduction
If scaphoid nonunion is untreated, it may progress to osteoarthritis of the wrist, known as scaphoid nonunion advanced collapse (SNAC) (Vender et al., 1987). Several surgical strategies have been developed to achieve union. The methods include non-vascularized bone graft (Carpentier et al., 1995), vascularized pedicled bone graft (Gras and Mathoulin, 2011; Sawaizumi et al., 2004; Waitayawinyu et al., 2008) and vascularized free bone graft (Jones et al., 2009; Pulos et al., 2018). In 2011, Wong and Ho, (2011) described an arthroscopic cancellous bone grafting technique, and several recent studies have since reported union percentages ranging from 86 to 100% using similar techniques (Burnier et al., 2024; Cognet et al., 2017).
Currently many different surgical techniques for arthroscopic management of scaphoid nonunions exist without evidence of superiority of one technique over another. In this study, we compared two different arthroscopic surgical techniques to treat scaphoid nonunions as our initial surgical method did not produce the expected results, and we found a higher incidence of nonunions than found in the literature. The study surgeon (ML) decided to modify the technique by placement of K-wires at the end of the surgical procedure instead of at the beginning. Our hypothesis was that a technique with debridement of the nonunion site followed by cancellous bone grafting and finally K-wire fixation would produce a a higher incidence of union than our initial sequence of debriding and grafting the nonunion site with the osteosynthesis material in place. The main objective of this study was to measure the incidence of union after performing arthroscopic cancellous bone grafting for the treatment of scaphoid nonunion with and without K-wires before debriding and grafting.
Methods
A retrospective, single-centre study was conducted that compared two consecutive patient cohorts who underwent arthroscopic treatment of scaphoid nonunion by the same surgeon (ML) (classified level V (Tang and Giddins, 2016)). Ethical approval for this study was obtained from an institutional review board, and written informed consent was obtained from all participating patients. In group 1, 17 patients were treated between 2011 and 2015 with the first surgical technique. In group 2, 25 patients were treated between 2015 and 2022 with the second surgical technique. The study flowchart is presented in Figure 1. We included patients aged 18–65 years who presented with scaphoid non-union that was diagnosed by plain radiograph and confirmed by CT scan (Figure 2). All were treated arthroscopically and had a minimum follow-up of 6 months. Exclusion criteria included missing data, non-compliance with immobilization, and the intraoperative discovery of osteoarthritis. We chose not to include patients with radioscaphoid osteoarthritis to avoid selection bias and to homogenize our cohorts. We excluded three patients owing to missing data, two patients who did not maintain immobilization for 3 months and one patient with an intraoperative discovery of SNAC.
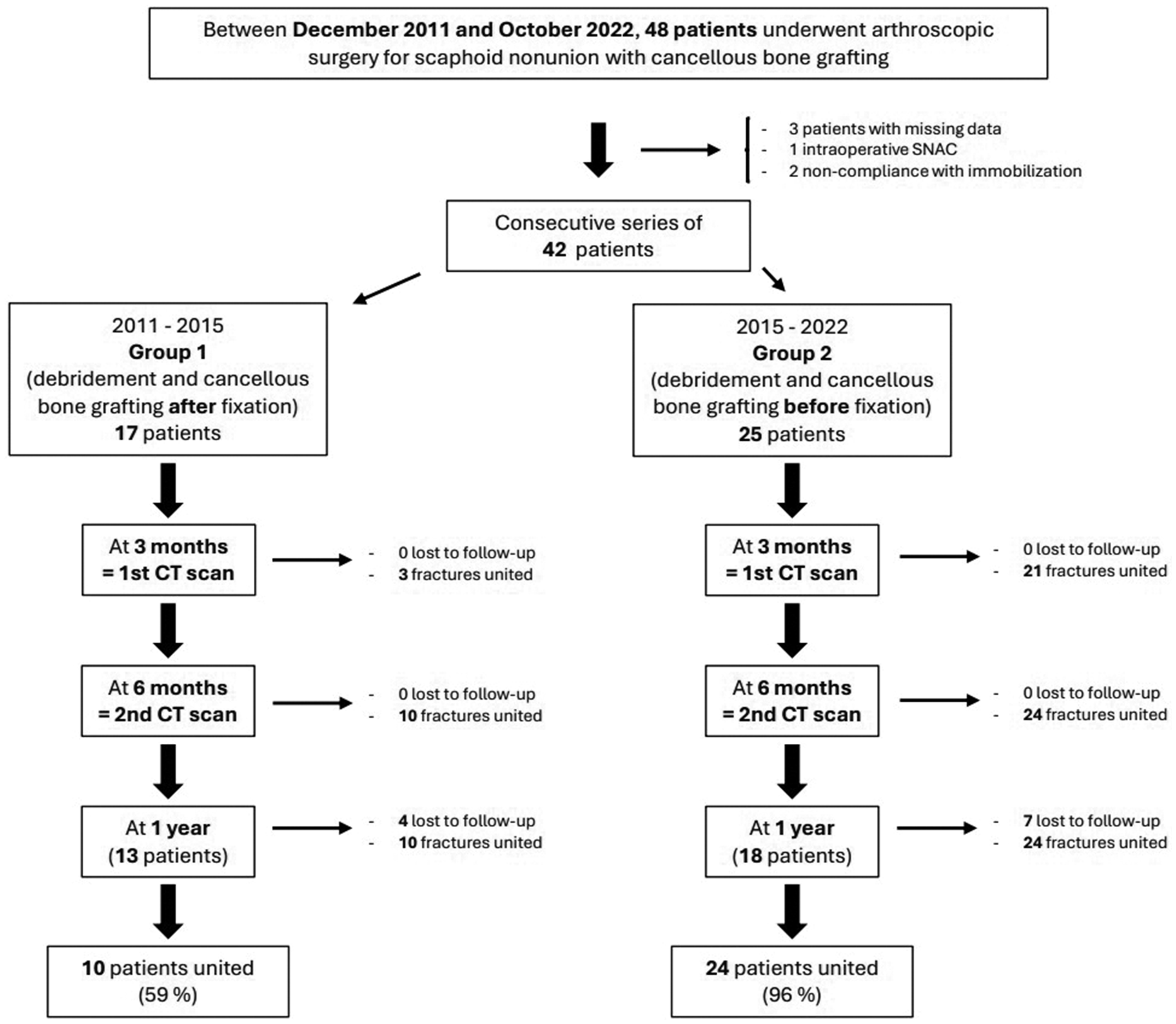
Flowchart.
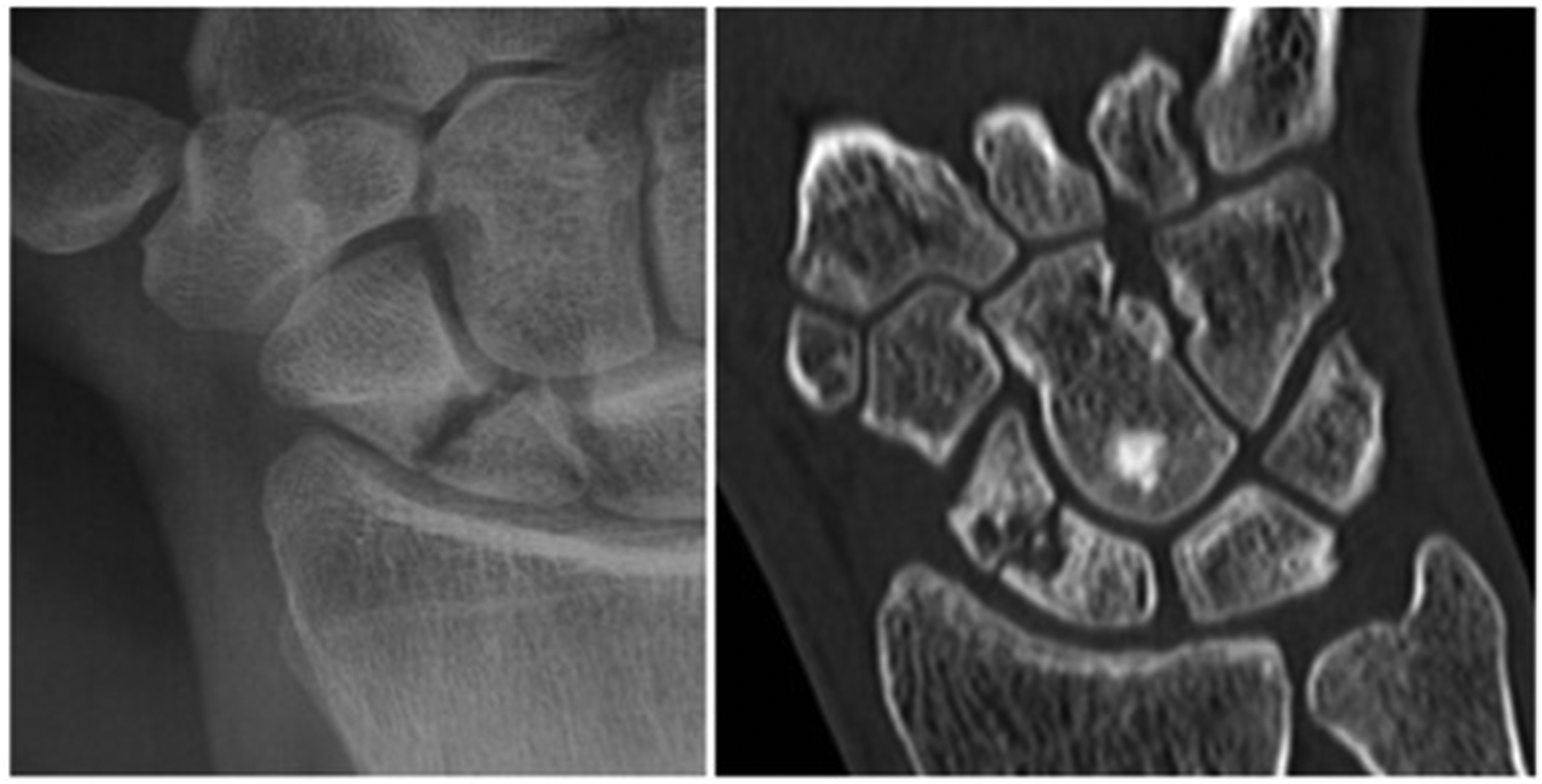
Radiographs and CT scan of a scaphoid nonunion.
Surgical technique of group 1
The operations were performed under regional anaesthesia with a tourniquet. The steps of the operation are shown in Figure 3. The first phase of the surgery consisted of percutaneously placing two or three 1 mm K-wires retrograde from the distal pole of the scaphoid. This was under fluoroscopic control with the wrist in hyperextension and ulnar deviation in order to reduce the scaphoid deformity. After applying a 4 kg vertical forearm traction with brachial counter-pressure, the surgeon performed an arthroscopic synovectomy of the wrist and then inspected the radiocarpal space via the 3–4 and 4–5 portals and the radial midcarpal (MCR) and ulnar midcarpal (MCU) portals. The nonunion site was debrided under dry arthroscopy with a curette and then with a motorized burr with the K-wires in place, and this continued until spontaneous bleeding of the bone was visible. Under short-term general anaesthesia, a 2 cm approach was made above the anterior superior iliac crest to harvest ten autologous cancellous bone cylinders with a bone marrow aspiration needle. Again under dry arthroscopy, the bone cores were positioned in the nonunion site (de Villeneuve Bargemon et al., 2022) via the MCR and MCU portals. Then, the grafts were packed with the probe around the K-wires. After releasing traction, the surgeon placed one additional K-wire in the scaphoid through its distal pole under fluoroscopic control to stabilize the site of the grafted nonunion. For proximal nonunions or major bone loss after debridement, the fourth K-wire was placed across the scapholunate joint to stabilize the proximal fragment. The exposed K-wires were then cut, bent and buried under the skin. An anterior forearm plaster splint was applied, and it was replaced between days 5 and 10 following surgery with a resin sleeve that left the thumb free. The duration of immobilization was 3 months.
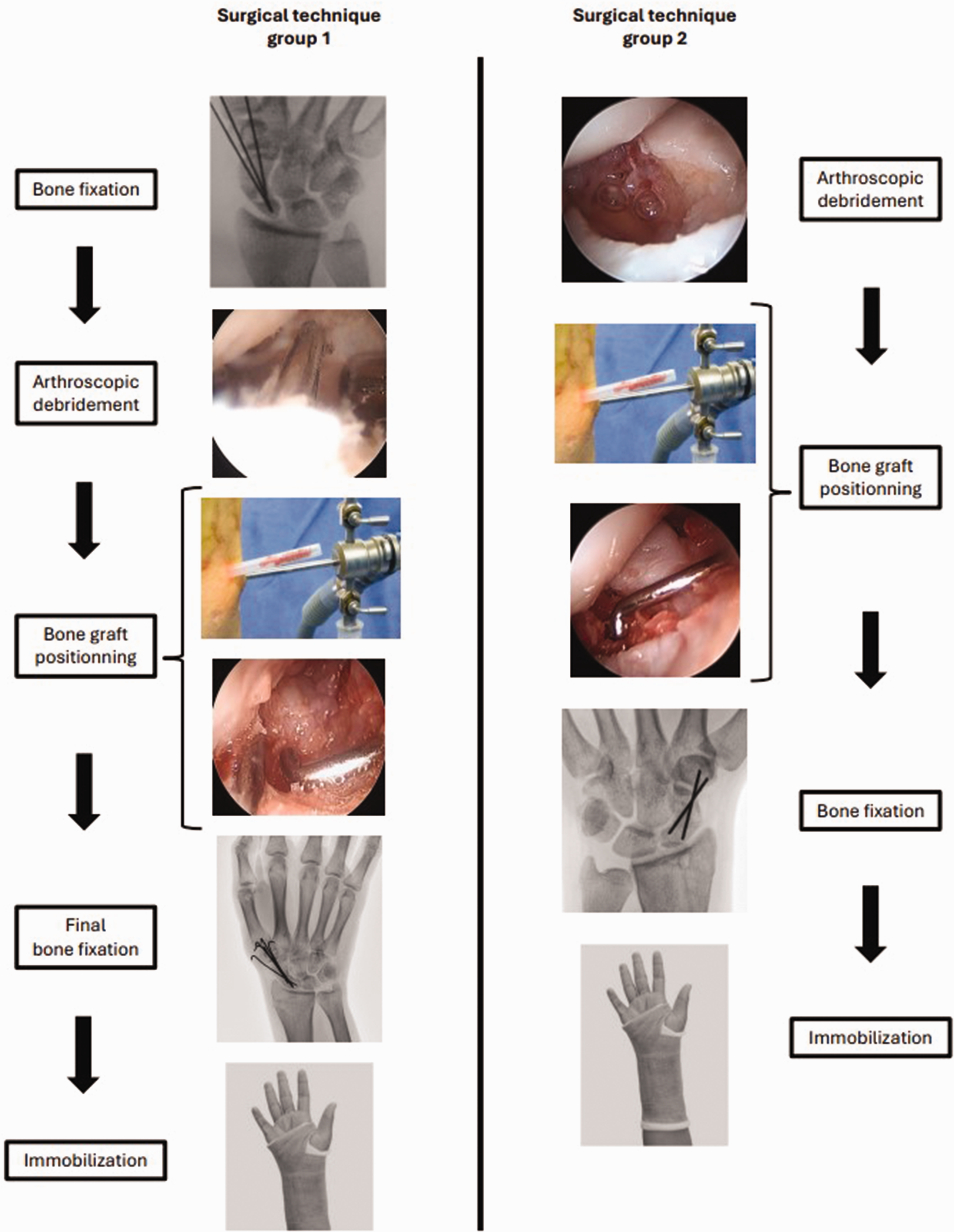
Comparison of the two surgical methods. In the group 1 (left side), debridement and bone grafting are carried out with the K-wires in place. In group 2 (right side), debridement and bone grafting are carried out before any K-wires are inserted.
Surgical technique of group 2
The installation protocol and arthroscopic exploration of the wrist were the same as for group 1 except that they were performed without the presence of any K-wires. The steps are presented in Figure 3. In the second stage of the operation, the nonunion site was debrided with a curette and then with a motorized burr until bleeding bone was obtained. During the third stage, cancellous bone for grafts was harvested from the radial styloid via a lateral approach to the first compartment between the tendons of the abductor pollicis brevis and extensor pollicis brevis. Trepanation was carried out using a bone marrow biopsy needle to harvest about ten cylinders of cancellous bone. The amount of bone harvested from the radial styloid has always been found to be adequate by the surgeon. In the fourth stage, through the MCR and MCU portals, the bone cores were positioned in the nonunion site and then compacted using a probe. After releasing traction for the fifth stage, in the same way as for group 1, the surgeon placed two or three 1 mm diameter K-wires in the scaphoid through its distal pole under fluoroscopic control and checked for good reduction and satisfactory recovery of the scaphoid’s height. For proximal nonunions or instances of major bone loss after debridement, the third K-wire was placed across the scapholunate joint to stabilize the proximal fragment. The K-wires were then cut, bent and buried beneath the skin. The immobilization protocol was the same as in group 1.
Postoperative protocol
The patients were seen in consultation on the first postoperative day and further at 15 days, at 1, 3 and 6 months and at 1 year postoperatively. For the final consultation, at 1 year, four patients from group 1 and seven from group 2 did not wish to attend, as they were experiencing no pain or discomfort in their daily and professional lives.
A control CT scan of each patient was performed 3 months postoperatively and then a second scan was performed at 6 months. Additionally, the CT scan allowed us to verify the absence of migration of the bone grafts out of the fracture site. For the last consultation at 1 year, standard posteroanterior radiographs with scaphoid view (posteroanterior view with ulnar deviation, oblique view and lateral view) were performed. Union was defined when bone callus was visible in more than 50% of the CT scan slices (Burnier et al., 2023) (Figure 4). We also compared the time taken to achieve scaphoid union in both groups.
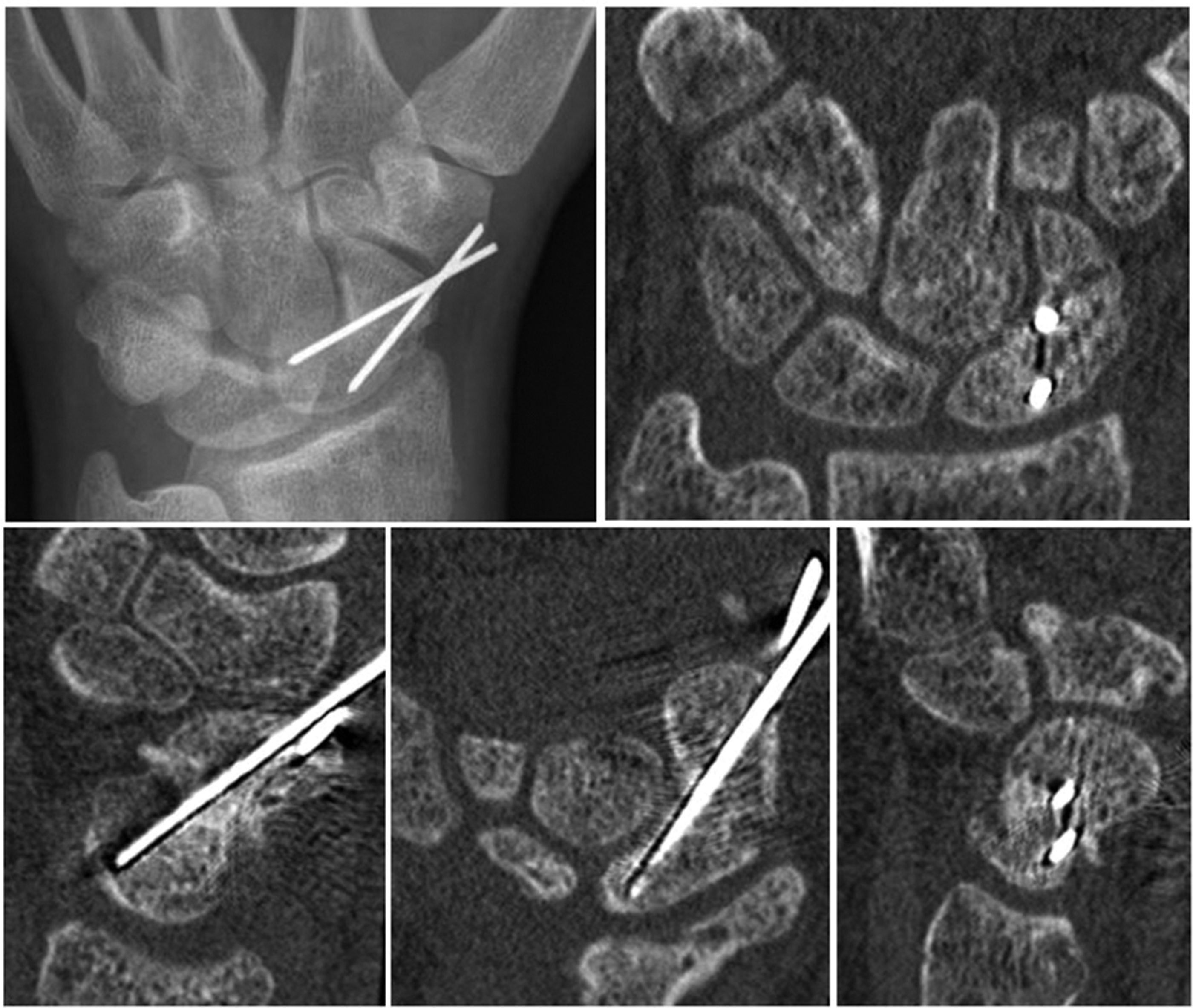
Radiographs and CT scan of a scaphoid union after arthroscopic bone grafting.
Scaphoid nonunions were classified according to Schernberg (1988) into six zones: proximal pole (zone I), proximal waist (zone II), central waist (zone III), distal waist (zone IV), distal pole (zone V) and tubercle (zone VI). The K-wires were removed within a month after the consolidation was noted on CT.
A functional assessment preoperatively was carried out and at each follow-up consultation based on a visual analogue scale score for pain and measurement of the ranges of wrist joint motion using a goniometer (extension, flexion, radial deviation, ulnar deviation, pronation and supination) and grip strength in kilograms (Jamar dynamometer). All patients were examined, and data were written in the patient’s files by the surgeon (ML). In patients with persistent non-union at the last follow-up, range of motion and grip strength were not measured.
Epidemiological data including sex, age at surgery, dominant side involvement, smoking status and time between the fracture and the arthroscopic repair were collected from the patients’ medical records. The study data were compiled by a researcher not involved in the surgery (AQT).
The two patients who did not maintain immobilization for the full 3 months (less than one 1 month) were in group 1 and did not achieve union. They were followed up like the other patients with CT scans at 3 and 6 months. These two patients were excluded from the analysis to avoid confounding factors. For the three patients with missing data, follow-up via ML was not possible as they had moved. After a phone call, it was confirmed that all three had achieved union but had only undergone radiographs during follow-up, and we were unable to retrieve their clinical information.
Statistical methods
The distribution of the data was normal. Normality of continuous data was assessed using the Shapiro–Wilk and Levene tests. Numerical variables were expressed as mean (SD), and dichotomous variables were expressed as absolute and relative frequencies (%). The similarity of the two groups was assessed by comparing their baseline demographics and durations of follow-up. Continuous outcomes, including visual analogue scale score, angles, grip strength and the intervals between fracture and arthroscopic treatment and time to union, were compared using a Student’s t-test to determine whether quantitative variables measured before and after treatment differed. Dichotomous outcomes such as consolidation were compared using a chi-squared or Fisher’s exact test. The alpha risk was set at 5% and bilateral tests were used.
Results
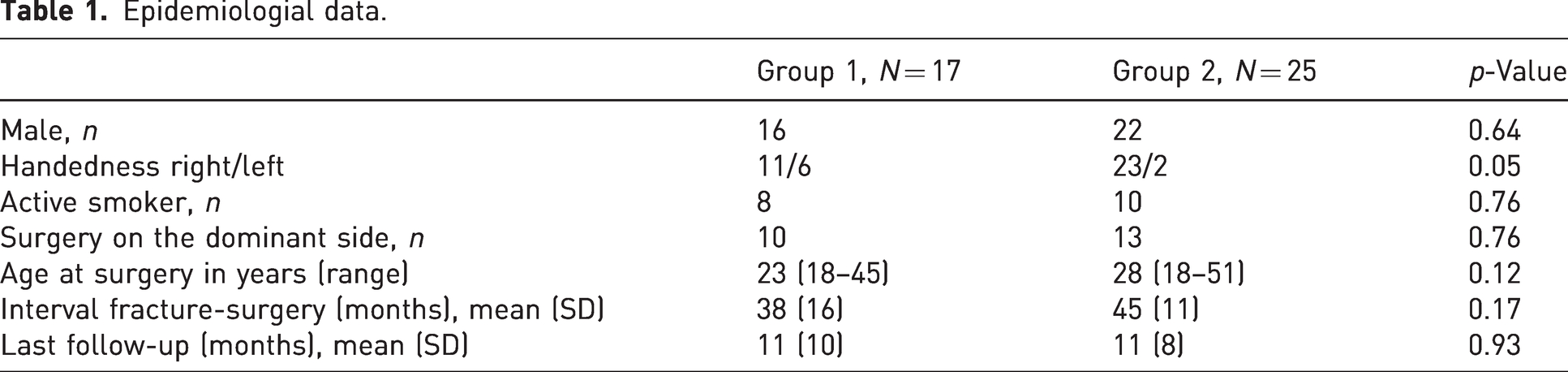
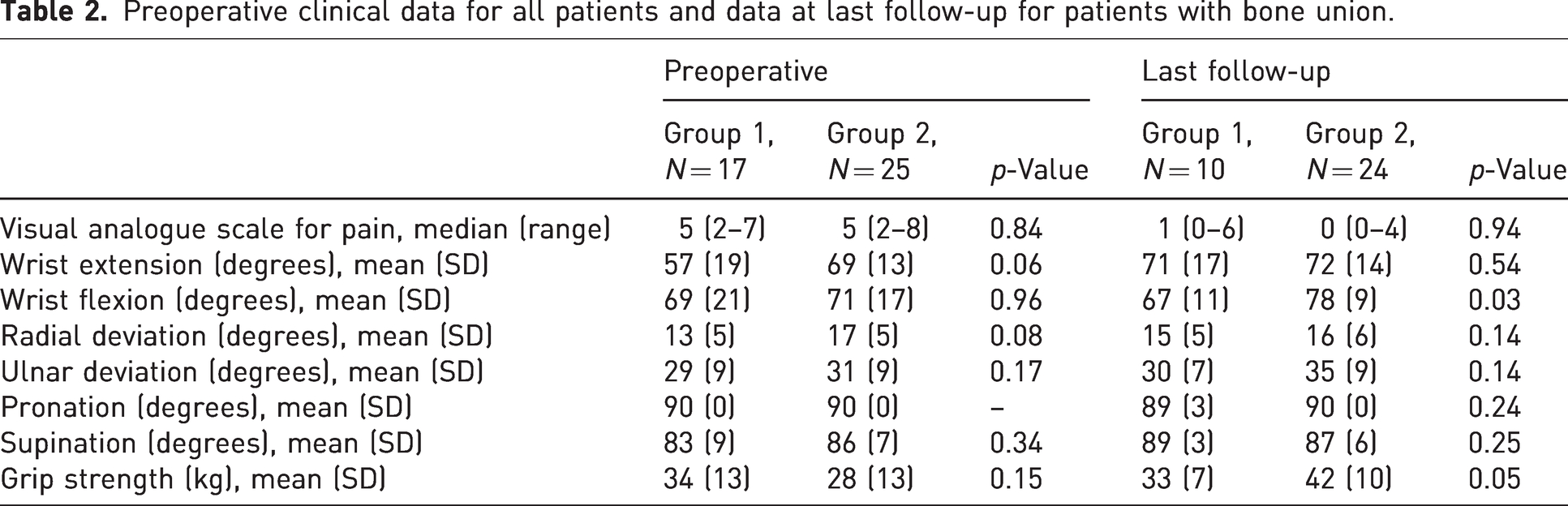
The epidemiological data of the patients are presented in Table 1. There was no significant difference between the two groups in sex, age, follow-up, the time between fracture and surgery, the operated dominant side, and number of smokers. Preoperatively, there was no difference between the two groups for the clinical data presented in Table 2.
Epidemiologial data.
Preoperative clinical data for all patients and data at last follow-up for patients with bone union.
Thirty-eight of the 42 patients were men, and the mean time between the fracture and surgery was 41.5 months. According to the Schernberg classification, four patients had a nonunion in part I, nine had a nonunion in part II, 20 had a nonunion in part III and nine patients had a nonunion in part IV.
At 3 months, there was already a significant difference in consolidation between group 2 (21 patients united) and group 1 (three patients united) (p < 0.001). At 6 months, the union was also significantly better in group 2 than in group 1. Union was obtained in 24 out of 25 patients in group 2 compared with in ten out of 17 patients in group 1 (p = 0.02). At 1 year, there were no newly consolidated patients in either group. Group 1 presented one union failure in zone II, three union failures in zone III and three union failures in zone IV of the Schernberg classification. For group 2 there was only one union failure, which was in zone III. There was no migration of cancellous bone graft outside the nonunion site. All 11 patients who could not be reviewed at 1 year had healing noted at 6 months.
The time to union was significantly shorter in group 2, with a mean of 3 months (SD 0.4) compared with 5 months (SD 1.4) for group 1 (p < 0.001). Range of motion and grip strength of the 24 patients whose scaphoid fracture was united are presented in Table 2.
Among the patients in group 2, eight nonunions were at the proximal pole (I and II according to the Schernberg classification), and all eight in these locations united.
Discussion
The main objective of our study was to compare the outcomes of two different arthroscopic sequences for scaphoid nonunion. The number of unions at 6 months following surgery was significantly higher in the group in which the nonunion site was debrided and grafted before K-wire insertion. In our study in group 1, union was obtained in ten patients (59%), whereas Wong and Ho (2011) reported union in 62 out of 68 patients (91%). In their study, the screw placed at a previous operation was left in place if it was stable during debridement and grafting. If the previous osteosynthesis was unstable or if it was a nonunion without hardware, the nonunion was debrided without hardware in place and, after positioning the K-wires, cancellous grafting was done. This approach can be likened to our surgical sequence of group 1 because the K-wires are already present at the time of grafting. We believe that the presence of K-wires or screws in the nonunion site before the debridement and positioning of the graft notably compromised filling and thereby limited the ability of the fracture to heal.
The groups in the current study differed in two ways: the timing of K-wire insertion and the site of graft harvesting. Cognet et al. (2017) mentioned the inconvenience caused by the presence of internal fixation material during inserting cancellous bone grafts arthroscopically. They recommend osteosynthesis with screws or K-wires after debridement and packing cancellous bone graft, as in our group 2. At 4 months, all 23 patients in their study showed union. In our study, the K-wires were inserted at the start of the procedure in group 1. Thus, we attribute the higher incidence of union failure in group 1 to partial, and probably incomplete, debridement of the non-union site owing to the presence of K-wires. In our opinion, the difference in bone graft harvest site cannot explain the difference in union between the two groups. It is difficult to say that iliac bone grafts are better than those taken from the distal radius. In a literature review by Basso et al. (2023), more unions were obtained with iliac cancellous bone grafts, but the authors could not draw conclusions regarding its superiority to distal radial grafts. Although it is not certain that iliac cancellous bone grafting produces a better result, its harvesting requires general anaesthesia and a second surgical site, unlike radial grafting, which is done at the same surgical site as the nonunion treatment.
All eight proximal scaphoid nonunions united in our study. Burnier et al. (2023) described 42 patients with nonunion at the proximal pole or waist. They found that arthroscopic treatment seemed to be an effective technique, although they did not isolate this population to establish a specific union percentage. However, Burnier et al. (2023) noted that proximal nonunions were not a risk factor for failure of union. In open, non-vascularized techniques with proximal-to-distal screw fixation as described by Alnot et al. (1988), there were two poor results and one failure out of seven patients. Furthermore, in a meta-analysis (Fujihara et al., 2022) bringing together 16 studies with a total of 1674 patients, nonunions treated by vascularized grafts (pedicled or free) had a higher union percentage than those treated by non-vascularized open techniques. There were 36% proximal scaphoid nonunions for which open non-vascularized, pedicled, or free vascularized techniques were associated with 18, 15 and 10% failures, respectively.
Burnier et al. (2023) stated that the use of K-wires or screws for the internal fixation did not impact scaphoid union. In our study, the surgeon prefers fixation with K-wires because the use of screw fixation in cases of pseudarthrosis with bone loss can lead to a humpback deformity owing to compression. However, we believe that centrally located screw fixation is entirely feasible in cases of pseudarthrosis without bone loss. Some surgeons secure the graft as the final step (Burnier et al., 2023; Cognet et al., 2017), which is similar to our surgical sequence in group 2, whereas others insert at least one K-wire before positioning the cancellous graft (Lamon et al., 2021). With a follow-up of 13 months, the study by Burnier et al. (2023) reported union in 72 out of 77 patients (94%) at 3.4 months. In the work by Lamon et al. (2021), which has a follow-up of 18 months, 37 out of 42 patients achieved union (88%) at 3 months. Burnier et al. (2024) published a systematic review of 17 studies evaluating the arthroscopic technique on 457 wrists with an average follow-up between 6 and 39 months. The authors reported a union percentage of 86–100%, with a time to union ranging from 2.3 to 7.8 months. There are few comparative studies on the ‘technical methods’ of arthroscopic management of scaphoid nonunions.
The fact that the scaphoid deformity was not reduced first (group 2) did not seem to have any impact on the quality of the nonunion reduction, but we did not assess anatomical reduction. In a recent study, De Bie et al. (2022) described correcting the humpback deformity and achieving a notable improvement of the scapholunate angle after arthroscopic treatment of scaphoid nonunion in 47 patients by inserting the K-wires only after carrying out the debridement of the nonunion site and after inserting the cancellous graft. Moreover, Schriever and Wilcke (2023) compared two cohorts: a control group without scaphoid deformity and another group with humpback deformity. Scaphoid deformity was assessed using CT scans to measure the height–length ratio difference between the operated and uninjured scaphoid. The authors noted a higher prevalence of radiographic osteoarthritis in the deformity group; however, all cases were mild, and no association between osteoarthritis and worse outcomes was found. Residual scaphoid deformity did not seem to have a notable adverse impact on mid-term wrist function.
The limitations of this study are its retrospective nature with associated information bias and the small sample size. The single-centre and single-surgeon nature of this study reduces the external validity of our results but limits ‘centre effect’ bias. Another limitation is that patients were not examined by an independent observer. A critique of our technique might be that the interpretation of consolidation is made difficult by the introduction of four K-wires. The use of two or three K-wires appears to be sufficient to allow for bone consolidation. We reserve the introduction of a third or fourth K-wires for complex cases, notably for scapholunate pinning in very proximal nonunions or for major bone loss after debridement. Other limitations were the difference in the bone graft donor site between the groups that the reduction of the scaphoid was not assessed.
A comparison of these two groups, analysing the reduction of scaphoid deformity with long-term clinical and radiological evaluation, would be of interest for future research.
Footnotes
Declaration of conflicting interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects.
Ethical approval
Ethical approval for this study was obtained from an Institutional of Review Board.