
Abstract
Introduction:
Wrist arthroscopy is a technically demanding procedure with a long learning curve, and many trainees report limited exposure during their surgical education. Simulation offers an accessible and ethical alternative to cadaver training. The objective of this study was to create a three-dimensional printed wrist arthroscopy simulator and to evaluate its ability to improve surgical performance.
Methods:
A wrist CT scan was segmented to extract the anatomical structures, which were then modelled and printed. The wrist was produced using soft or rigid resin depending on each structure, with replication of the major intercarpal and radiocarpal ligaments. A vertically adjustable support was designed to hold the artificial wrist on standard work surfaces for ergonomic training. An otoscope camera was selected for its video quality and effectiveness. Twenty-two surgeons of varying experience levels (residents, fellows and attending surgeons) completed a training programme composed of an initial assessment on a cadaver wrist, three sessions on the simulator, and a final assessment on the same cadaver wrist. Technical performance, procedure time, involuntary camera removals and perceived workload were assessed. Simulator fidelity and educational value were evaluated via questionnaires.
Results:
All participants improved their performance between the initial and final cadaver assessments. Improvements were greatest among residents. Participants completed procedures faster, with fewer errors and reduced perceived workload. The simulator was rated highly for anatomical realism and educational value.
Conclusion:
The quality and the low cost of this wrist arthroscopy simulator tend to encourage educational teams to use it in the training of surgeons.
Introduction
Arthroscopic procedures can be technically demanding and are associated with a long learning curve. Surgical skills can be developed over many years of training through cadaveric courses and the use of simulators. Nevertheless, residents and young surgeons report gaps in their wrist arthroscopy training (Pioger et al., 2019). A survey published in 2022 highlighted these challenges, showing that 36% of residents did not have the opportunity to observe a wrist arthroscopy procedure during their residency (De Villeneuve Bargemon et al., 2022). Such lack of exposure and hands-on learning opportunities may lead to iatrogenic complications, the incidence of which decreases with increasing surgical experience (Leclercq et al., 2016).
Artificial joint arthroscopy simulators offer several advantages over cadavers or real patients, including lower costs and fewer ethical concerns. They also allow surgeons to train on a variety of joints, such as the knee, elbow or shoulder. However, simulation on another joint does not appear to improve the skills of residents in wrist arthroscopy (Ode et al., 2018), emphasizing the need for joint-specific training to achieve adequate surgical competency. In this context, the present study aimed to create a wrist arthroscopy simulator using three-dimensional (3D) printing and to evaluate the transferability of surgical skills following its use.
Methods
We designed a synthetic specific 3D-printed wrist arthroscopy simulator. The research and development work was done between April 2021 and March 2023. The segmentation, modelling and printing steps were done in collaboration with clinical engineers specialized in 3D printing. A CT scan of the right wrist of a 34-year-old man without a history of trauma was segmented. Materialise Mimics software (v 23.0, Materialise, Leuven, Belgium) was used to isolate the various anatomical structures and generate a 3D file from the two-dimensional CT scan slices. The file was then imported into Materialise 3-matic® software for the complete computer-aided design process. The CT scan was adjusted to closely replicate the position of the wrist and forearm under traction during a surgical procedure. Among the ligaments encountered during wrist arthroscopy, we chose to represent the scapholunate and lunotriquetral ligament, triangular fibrocartilage complex and the palmar ligaments (radioscaphocapitate, radioscapholunate, short and long radiolunate, ulnolunate and ulnotriquetral). Each bone insertion was positioned based on published anatomic and biomechanic studies (Kijima and Viegas, 2009; Nagao et al., 2005). The extensor tendons were segmented to allow placement of the following portals: 3–4, 5–6, 6R, midcarpal ulnar and midcarpal radial. A base was designed to hold the wrist vertically with the fingers at the zenith. This base can be secured to most tables, and its height can be adjusted to suit a surgeon’s preferences (Figure 1). The wrist was printed using either soft or rigid resin, depending on the anatomical structure, on Form2 and Form3+ printers (Formlabs, Somerville, MA, USA) guided by Preform 3.27.1 software (Formlabs). The bones were printed using a rigid resin, connectors and skin with firm resin (80 Shore), and ligaments and tendons with elastic resin (50 Shore). The base was printed in polylactic acid using Ultimaker S3® and Ultimaker S5® printers (Ultimaker, Geldermasen, Netherlands) guided by Cura 4.10.0 software (Ultimaker).
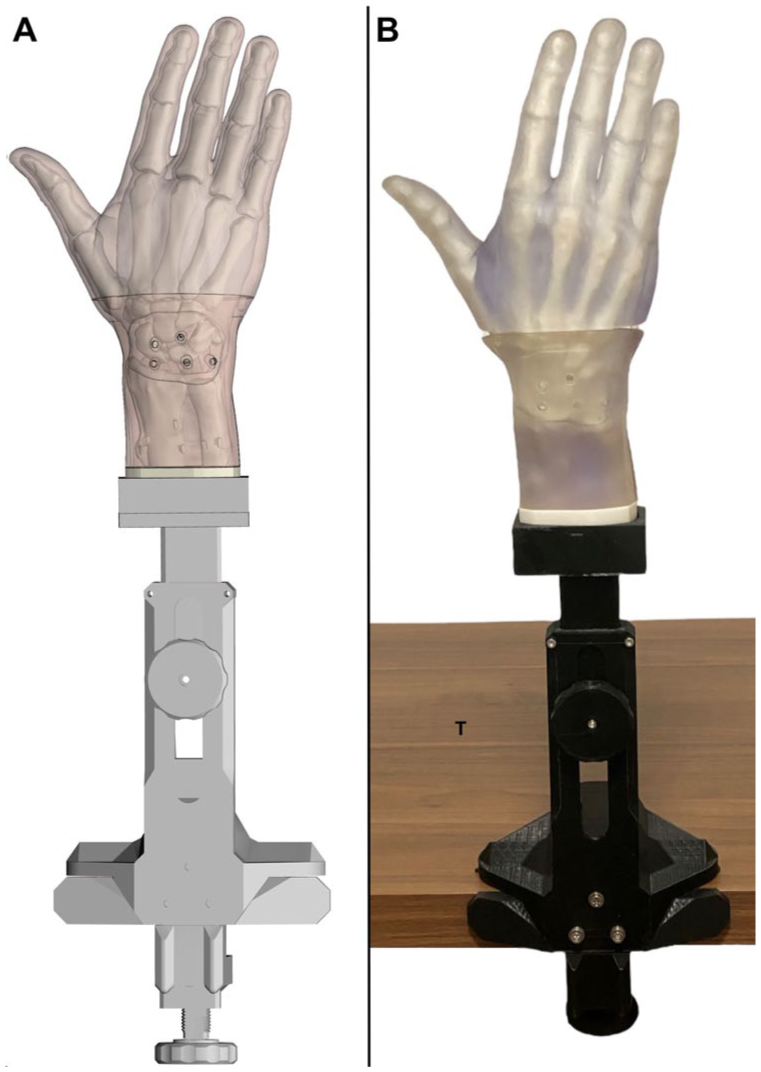
Modelling (a) and printing, and (b) of the wrist arthroscopy simulator with its base positioned on a table (T).
We chose to use the Visual earpick (found on lightinthebox.com), a camera originally designed for otoscopy. Although it differs from conventional surgical equipment, it has been shown to perform comparably to dedicated arthroscopic cameras for fundamental training tasks (Ling et al., 2019). The device features light emitting diode illumination integrated at its distal tip, which has a diameter of 3.9 mm. It is connected to a portable computer (MacBook Air 5.2, Apple, Cupertino, California, USA) to display images with the Quick Camera application (version 1.4.3, Simon Guest, App Store). A 2 by 4 cm probe (Karl Storz SE & Co., Tuttlingen, Germany) was used by the surgeons to examine anatomical structures in the wrist (Figure 2). The estimated cost for printing one model is approximately £200 in raw materials (including resin and the camera), excluding additional expenses such as software licences, printer usage, company fees and engineering time.

Wrist arthroscopy simulator with camera and computer screen showing the 3–4 portal view of internal wrist structures.
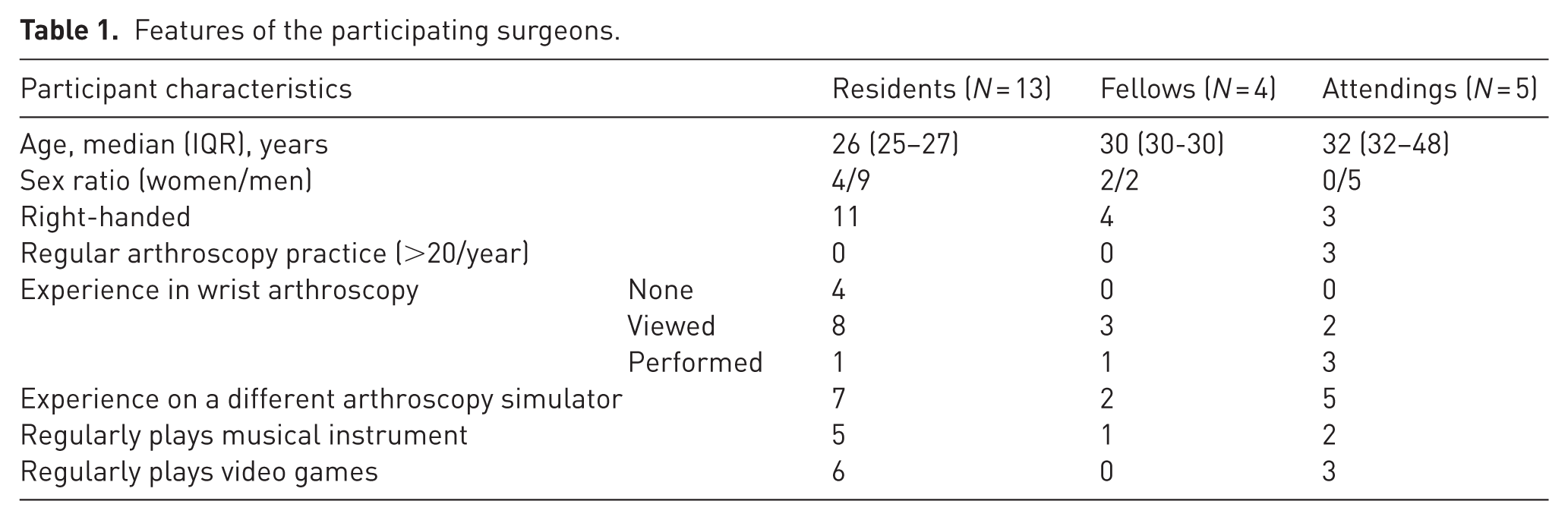
Participants’ demographics were collected before the first simulation session (Table 1). Participation in the simulation programme was mandatory for residents and fellows, whereas attending surgeons took part on a voluntary basis. A total of 13 residents, four fellows and five attending orthopaedic surgeons from the same university hospital participated in the simulation programme between April and June 2023. None of the participants were involved in the development of the simulator. The resident group comprised four residents in their first semester, four in their third semester, three in their fifth semester and two in their seventh semester.
Features of the participating surgeons.
The objectives of the simulation sessions were to familiarize participants with the arthroscopic anatomy of the wrist, including the main portals, and to develop basic wrist arthroscopy skills. Each participant received a document prior to the first session, containing the aims, methods, anatomical and technical descriptions, as well as access to an eLearning platform.
The first test session was done on a fresh cadaver wrist (C1) followed by three sessions on the simulator (S1, S2, S3), then a final test session on the cadaver wrist (C2) with the same instruments (probe, camera, computer). Intervals between sessions are reported as median (IQR). The first simulator session (S1) occurred 21 (14–30) days after the cadaver session (C1). The time between S1 and S2 was 7 (5–15) days, and that between S2 and S3 was 4 (1–9) days. A mean of 5 (1–6) days elapsed between S3 and C2, and a mean of 42 (37–49) days elapsed between C1 and C2.
The Skills in Wrist Arthroscopy (SWA) grid (Figure 3) was developed for this study to evaluate participant ability. Participants were instructed to use a palpation probe through a second portal to identify and centre the arthroscope on key anatomical structures, pausing for 1 s. The SWA scoring system comprises 30 items, each corresponding to a specific anatomical structure or arthroscopic task. Each correctly identified or executed item was scored one point, for a maximum score of 30. The examiner, a specialist highly experienced in wrist arthroscopy (level 4 according to Tang and Giddins, 2016), queried the portal placements and items in a random order to prevent predictable sequencing. No feedback was provided regarding the correctness of the identified anatomical elements to avoid reasoning by elimination.
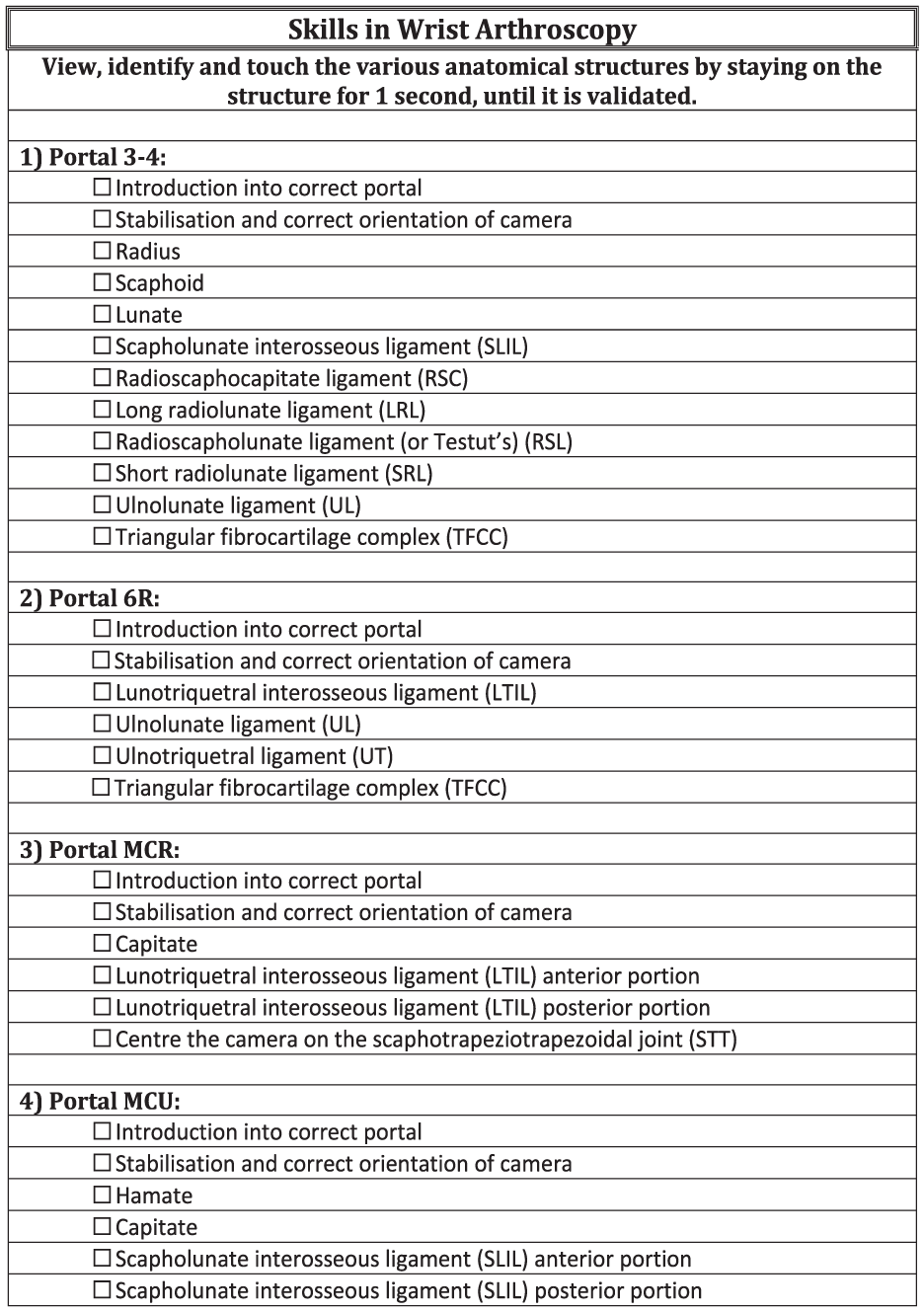
Skills in Wrist Arthroscopy measurement grid.
The procedure time for each simulation session was recorded and rounded to the nearest 5 s, with a maximum duration of 600 s (10 min). In addition, the number of involuntary camera removals during each simulation session was also documented.
The cadaver specimen was a right wrist, cut at the distal portion of the forearm, from a 72-year-old male. The examiner created the portals (3–4, 4–5, 6R, midcarpal radial and midcarpal ulnar) corresponding to the same portals as the simulator. The same cadaver wrist was used for the C1 and C2 sessions. During the initial assessment, a grade IV lesion of the scapholunate ligament was observed (Geissler, 2006), and the triangular fibrocartilage complex was rated as R4W2D2 (Herzberg et al., 2021). The short radiolunate and ulnolunate ligaments in the 3–4 portal and the lunotriquetral ligament in the 6R portal could not be identified by the examiners, so they were removed from the testing criteria. Consequently, the total number of testing criteria in the SWA grid was reduced to 27 for the C1 and C2 sessions.
The Arthroscopic Surgery Skill Evaluation Tool (ASSET) is a validated scoring system ranging from 0 to 100, used to assess a surgeon’s arthroscopic skills, including safety, dexterity, efficiency, procedural flow and autonomy. Higher scores indicate superior technique and proficiency, whereas lower scores reflect technical difficulties or less experience in wrist arthroscopy. During the cadaver sessions C1 and C2, each participant’s ASSET score was calculated as the average of the scores independently assigned by two expert examiners, each performing more than 20 wrist arthroscopy procedures per year.
Originally developed for aviation, the National Aeronautics and Space Administration Task Load Index (NASA-TLX) (Hart and Staveland, 1988) was used to estimate surgical difficulty and track skill progression (Bell et al., 2022). A debriefing was conducted at the end of each session to assess perceived workload using the NASA-TLX, which provides a weighted score based on six subscales: mental demands (NASA 1), physical demands (NASA 2), temporal demands (NASA 3), own performance (NASA 4), effort (NASA 5) and frustration (NASA 6).
A fidelity and satisfaction questionnaire was developed to compare the 3D printed simulator with the cadaveric wrist (Figure 4). The questionnaire used a five-point Likert scale ranging from −2 (strongly disagree) to +2 (strongly agree). Participants were asked to evaluate the external and intracarpal appearance and anatomical fidelity of the simulator, including the colours of bone and ligamentous structures. Technical aspects were also rated, such as the reliability of the arthroscopic equipment (camera, light, cables, probe) and the quality of the arthroscopic image.
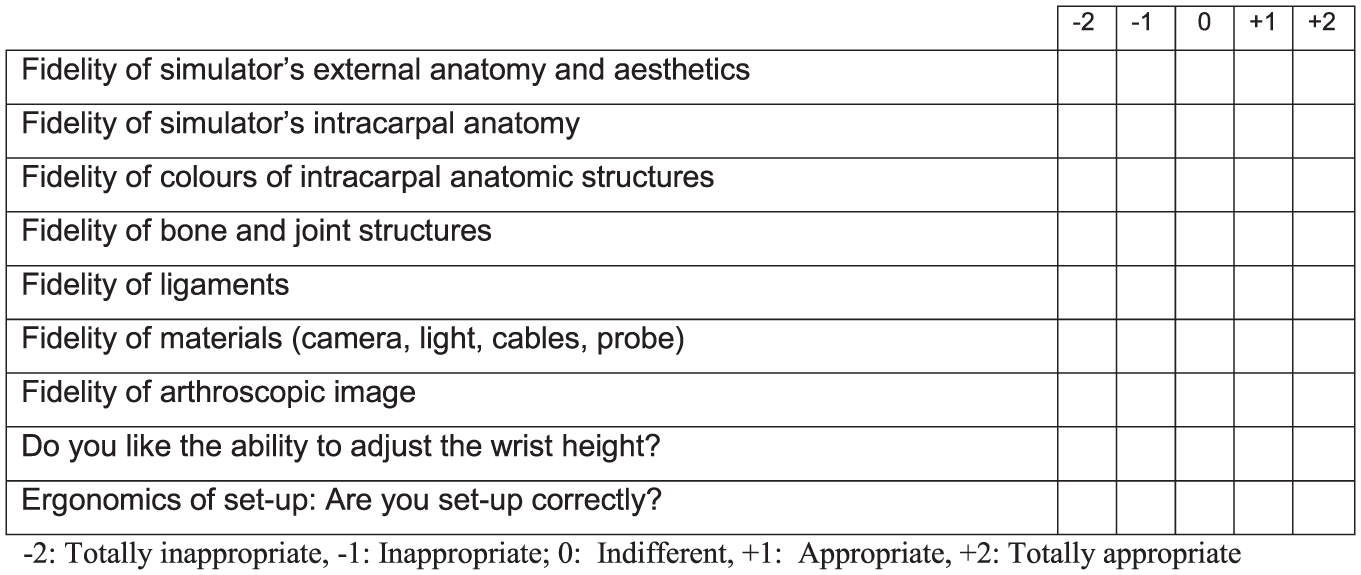
Measurement grid for simulator.
The participants also rated the usefulness of the simulation sessions in improving their professional practice on a scale from 0 to 10.
Statistical analyses
To assess the normality of the distributions, the Kolmogorov–Smirnov test was applied to detect deviations from a Gaussian distribution. Although some variables were normally distributed, non-parametric tests were used for group comparisons to account for potential violations of normality assumptions across the dataset. Variables are presented as median (IQR). The SWA, ASSET, and NASA-TLX scores during the simulation sessions were rounded to the nearest 0.1 and mean procedure times were rounded to the nearest second.
The Wilcoxon signed-ranks test was employed to compare scores and values within each group across the different sessions. The Mann–Whitney U-test was used to compare residents at the start and end of the training, considering their arthroscopy experience as well as whether they played musical instruments or videogames. Interrater reliability of the ASSET scores was assessed to ensure consistency between the two independent examiners, using Kendall’s Tau correlation coefficient to quantify the degree of agreement. The significance threshold was set at 5%.
Results
Table 2 presents the scores and metrics, including SWA, procedure time, involuntary camera removals, ASSET score and NASA-TLX for all participants and subgroups, illustrating the progression of performance across the initial cadaver session (C1), simulation sessions (S1–S3) and the final cadaver session (C2). All participants demonstrated significant improvements, especially residents. SWA and ASSET scores increased, procedure times and errors decreased, and perceived workload (NASA-TLX) was reduced following training.
Scores and performance metrics (SWA, procedure time, involuntary camera removals, ASSET and NASA-TLX) for all participants and subgroups across the initial cadaver session (C1) simulation sessions (S1–S3) and the final cadaver session (C2).
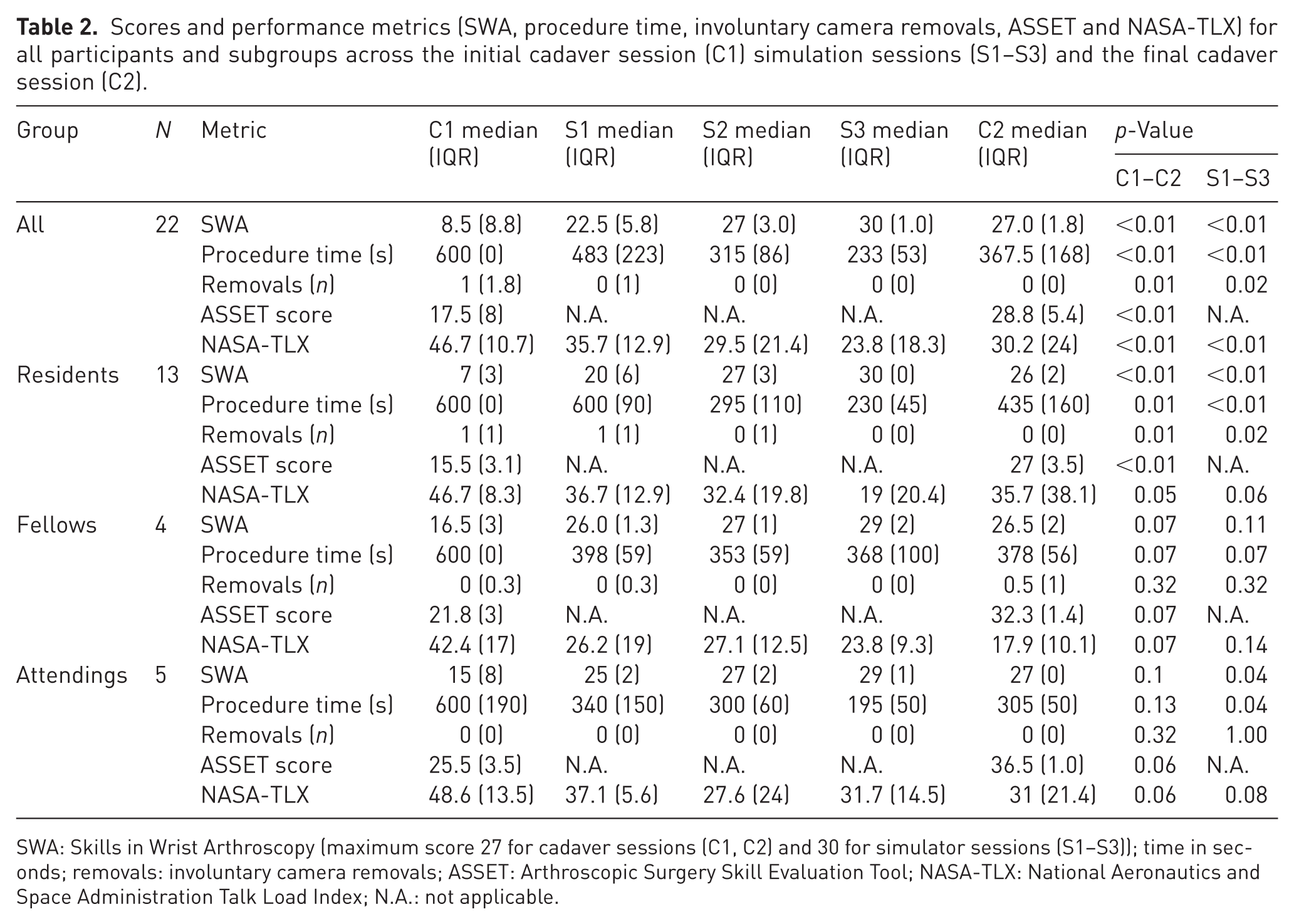
SWA: Skills in Wrist Arthroscopy (maximum score 27 for cadaver sessions (C1, C2) and 30 for simulator sessions (S1–S3)); time in seconds; removals: involuntary camera removals; ASSET: Arthroscopic Surgery Skill Evaluation Tool; NASA-TLX: National Aeronautics and Space Administration Talk Load Index; N.A.: not applicable.
There was strong agreement between examiners, with Kendall’s Tau values of 0.73 (p < 0.001) for C1 and 0.76 (p < 0.001) for C2, confirming the consistency of the ASSET tool in evaluating the participants’ skills.
Perceived workload was lower during C2 than C1 across all groups (Figure 5). There was no relationship between the performance on the simulator and having previously done wrist arthroscopy or played a musical instrument or regularly playing video games. All participants completed the simulation programme and none did additional sessions. The participants stated that they did not perform or see any wrist arthroscopy in the operating room during the study period.
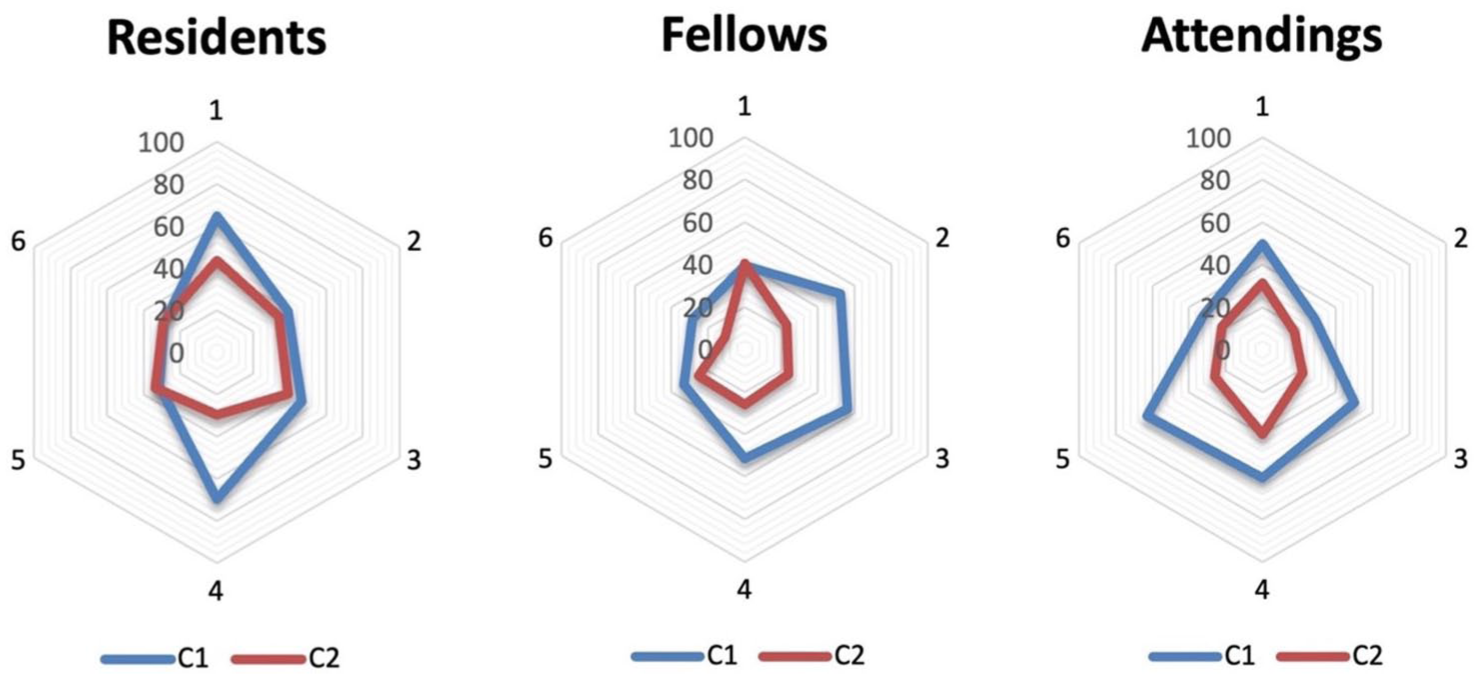
National Aeronautics and Space Administration Task Load Index (NASA-TLX) of C1 (first cadaveric session, blue) and C2 (second cadaveric session, red) across three groups of orthopaedic surgeons: residents (surgical trainees), fellows (postgraduate specialty trainees) and attendings (fully qualified surgeons).
Assessment of simulator and simulator sessions
The fidelity of the simulator was considered appropriate or even totally appropriate, with a score of 2 out of 2 (1–2). The accuracy of the bone and joint structures received the highest ratings (2 (2–2)) while the colours of the anatomical structures were rated less favourably (1 (1–1.8)). The sessions on the simulators were deemed ‘formative’ or even ‘very formative’ by participants with a score of 2 (2–2) for residents, 2 (1.8–2) for fellows and 2 (1–2) for attendings surgeons.
The simulator was considered helpful for improving professional practice, with a usefulness score of 9 (8–9) out of 10 for residents, 9 (7.8–10) for fellows and 8.5 (7.3–9) for attending surgeons.
Discussion
This study demonstrated that the use of a wrist arthroscopy simulator improved technical performance across all participant groups, with the most notable gains observed among residents. Participants achieved higher SWA and ASSET scores, completed procedures faster, made fewer errors and reported a reduction in perceived workload over time. The simulator was also rated highly for fidelity and educational value.
As the SWA score is an original tool developed for this study, it could not be directly compared with other published series, but it captured improvements in anatomical recognition and procedural steps. Performance varied by experience level. Residents showed the greatest improvements in our study, while more experienced surgeons benefited less in relative terms, particularly for less frequently performed joints such as the wrist and elbow, as demonstrated by Chuang et al. (2024).
Other in-house arthroscopy simulators developed for the shoulder (Dau et al., 2022), the knee (Milcent et al., 2021) and small joints (Mizera et al., 2024) have demonstrated improvements in basic technical performance. Although a direct comparison with commercial simulators was not performed, our findings are consistent with the broader simulation literature. For example, Li and George (2017) conducted a systematic review of low-cost surgical simulators and reported that these devices, both commercial and non-commercial, consistently improved fundamental procedural skills and showed acceptable validity for training purposes. However, the SWA score does not evaluate iatrogenic risks or procedural quality dimensions captured by the ASSET score. The ASSET score, previously validated for shoulder and knee arthroscopy (Koehler et al., 2013; Koehler and Nicandri, 2013), has also shown improvement in other arthroscopic training studies. Camp et al. (2016) demonstrated that cadaveric skills laboratories significantly improved resident performance in knee arthroscopy compared with matched controls, with progress occurring twice as fast as with a high-fidelity simulator. However, the authors noted that the simulator may become more cost-effective if used for at least 300 hours per year. One of the objectives of the simulator is to complement cadaveric laboratory training by providing a more accessible and readily available platform for learners to practice, enabling more frequent repetition and consistent skill progression.
In terms of design, the simulator included practical and cost-saving innovations. An increasing number of health care centres and surgery department now possess 3D printers and integrate them into their daily practice (Kermavnar et al., 2021). Three-dimensional printing is considered environmentally and economically advantageous owing to reduced material waste, the possibility of on-demand production and localized manufacturing, particularly when production volumes are relatively low (Jung et al., 2023). In this context, the elements distal to the region of interest (phalanges, tendons and soft tissues of the fingers) can be omitted to reduce cost. High-fidelity simulators enhance user motivation and engagement, encouraging repeated practice and deeper cognitive involvement, which in turn leads to better learning outcomes (Sauer and Sonderegger, 2009).
This study has several limitations. The sample size was relatively small, particularly for fellows and attending surgeons, and potential bias may have arisen from the use of subjective evaluations. Another limitation is that the scoring systems employed, particularly the SWA score, have not been formally validated. While the reduction in time required to complete tasks in our study may indicate improved efficiency, previous research has shown that speed alone does not adequately reflect surgical competency (von Bechtolsheim et al., 2022). The next version of this work will take these points into account in order to optimize both training and assessment. Despite these limitations, our results support the integration of such simulators into orthopaedic training programs.
Footnotes
Acknowledgements
The authors sincerely thank those who donated their bodies to science so that anatomical research could be performed. Thanks to the Anatomy Laboratory and the Radiology Department of the Besançon University Hospital. Thanks are due to Camille Coussens and Benjamin Billotet, engineers, and to Joanne Archambault, PhD for language support. The authors used ChatGPT (OpenAI) during the revision phase to assist with language and phrasing. No content was generated from scratch, and all modifications were reviewed and validated by the authors.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LO: Medartis, Elsevier. FL: Medartis, Arthrex, Evolutis. The other authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
The study was carried out in accordance with French regulations and was approved by our local ethics committee in accordance with the ethical standards defined in the 1964 Declaration of Helsinki.
Informed consent
Not applicable.