
Abstract
Maintaining an appropriate balance between mobilization and immobilization is a central challenge in hand rehabilitation and has a decisive impact on tissue healing, functional recovery and patient outcomes. This narrative review examines the concept of balance in the hand by outlining risks that threaten this balance, reviewing the available evidence comparing mobilization and immobilization strategies, and highlighting the strength of the evidence and existing research gaps. The practical achievement of balance is explored with particular emphasis on the timing of mobilization, effective communication among clinicians and patients, and the maintenance of balance throughout the rehabilitation process. Three clinical case reports are included to illustrate how hand therapists navigate the daily challenge of adapting rehabilitation strategies to evolving biological, functional and contextual factors. The review further addresses how much balance is sufficient, how balance can be maintained after formal rehabilitation and the longer-term implications for hand function and participation. Successful rehabilitation in hand care relies on individualized, collaborative decision-making involving the therapist, surgeon and patient, and the patient’s environment, with the overarching goal of optimizing functional outcomes while minimizing complications.
Keywords
Introduction
Restoring balance is fundamental to improving hand function. Before we can explore how to restore balance, we must first define what balance means and recall what constitutes balance in the human hand.
The term ‘balance’ has multiple definitions. It can refer to ‘placing something in a steady position so that it does not fall’, or to ‘a state in which all parts are equal in strength or importance’. Applied to the human hand, balance is maintained by an intricate biomechanical and neurological system operating under both conscious and unconscious control of the central and peripheral nervous systems. This complex interplay between sympathetic, sensory and motor nerves, muscles, tendons, pulleys, ligaments, bones and joints enables the hand to perform an astonishing variety of movements – on average over 4700 different grasps per day (Bullock et al., 2013; Feix et al., 2016).
Risks to balance in the hand
The balance of the human hand can be compromised by a variety of factors, most notably caused by trauma and disease affecting the hand or upper limb. These factors include bony non-unions and malunions, joint instability, pulley insufficiency, impaired tendon gliding, neuromas, nerve adherence, vascular insufficiency and unstable scar tissue. Each of these conditions may lead to an imbalance. Wound healing leading to scar formation and skin adhesions, for example, may result in joint contractures. Imbalance of the hand, for example after peripheral nerve injuries, may further lead to muscle atrophy, cartilage damage, sensory loss and subsequent reduced motor skills, dexterity and strength, and increased pain.
Hand surgeons and therapists – if available for the ‘patient’ (the term originating from the Latin word ‘patiens’, meaning ‘enduring’ or ‘suffering’) – can greatly support restoring the balance of the hand. On the other hand, surgery can create more ‘suffering’ to the patient and, thus, be a risk to the restoration of balance. For example, the use of medical hardware such as screws, plates and sutures – although indispensable for structural stability – may contribute to complications including adhesions impairing tendon gliding, reduced muscle force, ligamentous instability and scar contracture.
After referral to hand therapy, overly enthusiastic therapists who mobilize the hand prematurely or excessively risk provoking oedema and pain, which can compromise joint motion and delay healing. This over-treatment can result in serious complications such as tendon rupture, joint instability, and inflammation – often resulting in decreased patient adherence owing to pain. In contrast, therapists who exercise excessive caution may prolong immobilization unnecessarily, leading to joint stiffness, decreased range of motion, loss of function and strength, as well as the formation of restrictive scars, adhesions and joint contractures. A third cause of imbalance occurs when the surgeon, therapist or patient fails to recognize a threatening loss of balance, particularly in cases of slowly progressive contracture.
Another factor that may jeopardize balance in the human hand is the patient’s own coping strategies during rehabilitation. Therefore, hand surgeons and therapists should screen a patient for ‘yellow flags’, indicators of potential psychological and social barriers to recovery (Stearns et al., 2021). Examples of yellow flags are fear-avoidance beliefs, catastrophizing, passive coping strategies, social- and work-related problems or low self-efficacy (Luomajoki and Schesser, 2021).
Mobilization vs. immobilization – where’s the evidence?
It is evident that restoring hand function requires a carefully calibrated balance between mobilization and immobilization, making rehabilitation a complex process. However, achieving this balance after a hand injury is a critical determinant of recovery and overall functional outcomes. For example, the surgical technique can affect whether a patient is able to mobilize the injured hand, depending on factors such as fracture stability, suture durability and surgical skill. Striking the right balance is further complicated by the lack of consensus of immobilization time post-surgery and the often vague definitions of ‘safe zones’ for early active motion (EAM). Rigid, protocol-driven rehabilitation approaches may overlook individual patient needs, highlighting the limitations of a one-size-fits-all model in hand therapy. Patient-specific factors, including body image, sensory perception and pain tolerance, are crucial in defining the appropriate degree of mobilization. Some patients may be unable to mobilize effectively without applying excessive force, while others require very gentle guidance. In digits that are particularly sensitive or have lost sensation, mobilization may need to be guided visually, for example through mirror therapy, to ensure safe and effective movement (Deconinck et al., 2015; Tofani et al., 2022).
Current evidence regarding extensor tendon injuries of the hand is moderate to low in quality, with best support for early mobilization after repairs in zones IV–VIII (Collocott et al., 2023; Wong et al., 2017). In these zones, moderate evidence supports early controlled or active mobilization over immobilization for improved short-term outcomes, faster recovery, reduced adhesions and earlier return to function, but long-term differences are unclear (Bojnec et al., 2025; Collocott et al., 2018). Early active motion is delivered via controlled active motion or relative motion extension splinting, both showing similar range of motion outcomes and low complication rates (Bojnec et al., 2025; Collocott et al., 2018; Hirth et al., 2021; Wong et al., 2017). Dynamic splinting and static splinting with early motion are both used, with EAM protocols being simpler and more convenient (Collocott et al., 2018; Wong et al., 2017).
Immobilization of extensor tendons is reserved for specific cases such as non-compliance, complex injuries or distal zones (I–II). In these zones, immobilization remains standard owing to thin tendons and higher risk of rupture, because they are less amenable to strong repair and early motion (Wong et al., 2017). Insufficient evidence is available to determine when surgical intervention is indicated (Lin and Samora, 2018). Zone III extensor tendon injuries are most often managed with splinting and immobilization, but early active motion protocols and relative motion orthoses are increasingly used, especially after surgical repair (van Strien and van Zwieten, 2023). Recent case reports and retrospective studies show that, after surgical repair, early controlled motion (e.g. short arc motion protocols) can yield excellent range of motion and functional outcomes, with low rates of extension lag or boutonnière deformity (Ecker et al., 2020; Johnson et al., 2021).
For the treatment of flexor tendon injuries, there is broad consensus that early mobilization results in better functional outcomes than immobilization, supported by major advances in surgical techniques and rehabilitation protocols in the past decades (Neiduski and Powell, 2019; Peters et al., 2021; Silva et al., 2003; Tang et al., 2021; Wada et al., 2001). Pulley venting and the use of multi-strand core sutures are considered safe and effective, although the evidence is largely based on expert consensus and retrospective studies (Douwes et al., 2025). However, the optimal method of mobilization remains controversial (Douwes et al., 2025; Khor et al., 2016; Newington et al., 2021). For example, in a randomized controlled trial comparing controlled active motion with early passive mobilization in flexor tendon injuries in zone 2, both protocols improved hand function, with early advantage in digital range of motion and hand function favouring the controlled active protocol (Ahmed et al., 2025).
Most studies on flexor tendon injuries are limited by low methodological quality, including high risk of bias, small sample sizes and inconsistencies in study design – particularly regarding rehabilitation protocols and surgical technique (Neiduski and Powell, 2019; Peters et al., 2021). No consensus exists on the optimal repair technique for the various anatomical zones, and direct comparisons are hindered by heterogeneity in outcome measures and reporting (Shaw et al., 2022). Systematic reviews underline the urgent need for adequately powered randomized controlled trials and standardized outcome measures (Deshmukh et al., 2025).
Across metacarpal, finger and distal radius fractures, starting protected, pain-free motion as soon as stability allows improves early function and stiffness without clear evidence of higher complication rates, although caution is warranted in unstable patterns and in fixation at risk of loosening. For example, randomized trials and meta-analyses in distal radius fracture fixation consistently demonstrate that immediate or very early mobilization after open reduction internal fixation (ORIF) leads to improved wrist range of motion, grip strength and patient-reported outcomes during the early postoperative period (up to 6 weeks to 6 months) (Deng et al., 2021; Laohaprasitiporn et al., 2022; Quadlbauer et al., 2021). At 1 year, these differences are generally small or absent, although some studies report modest persistent advantages in motion and strength (Quadlbauer et al., 2017, 2021). Meta-analyses show that early mobilization after volar plating improves functional scores, pain, and forearm rotation without an overall increase in complications, although a possible increased risk of implant loosening or re-displacement has been reported, underscoring the importance of appropriate case selection (Daher et al., 2025; Deng et al., 2021). Comparisons with short-term splinting followed by home exercise show no clinically relevant long-term differences, and early motion appears safe (Clementsen et al., 2019; Laohaprasitiporn et al., 2022).
The evidence base for early mobilization after metacarpal fractures, while limited in overall quality, is broadly consistent across fracture types and treatment modalities (Vikhe et al., 2024). Randomized trials in stable metacarpal fractures, especially fifth metacarpal neck fractures, demonstrate that immediate or early motion results in less early stiffness, reduced swelling, improved functional scores and faster return to work compared with immobilization, without compromising fracture alignment (Martínez-Catalán et al., 2020; Retrouvey et al., 2022). After operative fixation, both comparative and observational studies indicate that rigid fixation strategies permitting early motion are associated with improved early functional recovery and similar union rates and complication profiles compared with prolonged immobilization (Siriwittayakorn et al., 2023; Vasilakis et al., 2019).
For most adult finger phalangeal fractures that are acceptably aligned or securely fixed, early controlled mobilization within a protective splint is favoured over prolonged immobilization, mainly to reduce stiffness and restore motion, provided fracture stability is not compromised (Kynaston et al., 2025; Zhang et al., 2024). A recent scoping review of extra-articular proximal phalangeal fractures found no high-quality RCTs; conservative studies typically immobilized for 3–7 weeks but started active exercise immediately, while surgical series began exercises between 5 days and 3 weeks; all reported good total active motion (TAM) (240–259°) but with high risk of bias (Vervloesem et al., 2023).
Strength of evidence and research gaps
The current literature supports early mobilization for most hand injuries and surgeries, provided that fixation or repair is stable and patient compliance can be ensured (Barrett et al., 2022; Chevalley et al., 2022; Deng et al., 2021; Kynaston et al., 2025; Sultana et al., 2013; Talsma et al., 2008). Immobilization is preferable in selected scenarios, such as unstable repairs or complex injuries, or in patients unable to reliably participate in therapy (Axenhus and Schmidt, 2025; Barrett et al., 2022; Kynaston et al., 2025; McCarron et al., 2025). The evidence base is strongest for early mobilization in extensor and flexor tendon repairs and after stable fracture fixation, but is less robust for complex injuries (Chevalley et al., 2024; Talsma et al., 2008).
Despite the trend towards early mobilization, significant practice variability persists, often driven by surgeon preference, local protocols and patient factors rather than high-level evidence (Axenhus and Schmidt, 2025; Barrett et al., 2022, 2025). Although the evidence base is growing, important gaps remain in defining precise indications for both mobilization and immobilization, particularly in complex injuries, pediatric patients and individuals with comorbidities. There is a clear need for standardized guidelines and additional high-quality randomized controlled trials to define optimal protocols for specific clinical scenarios (Axenhus and Schmidt, 2025; Barrett et al., 2022; Deng et al., 2021).
However, recruitment into surgical randomized controlled trials is often hindered by limited clinical equipoise, which contributes to the relative scarcity of large, definitive trials in this field. The evidence base is further limited by several recurring methodological challenges. Many studies are constrained by small sample sizes and considerable heterogeneity in surgical techniques, rehabilitation protocols and outcome measures. Definitions of key interventions, such as ‘early’ mobilization, vary widely across studies, reducing comparability and limiting meta-analytic synthesis. These limitations should be considered when interpreting current recommendations and underscore the need for high-quality, multicentre collaborative research.
Achieving balance in the hand
Balancing the timing of mobilization
Finding the right starting point for mobilization is not without its challenges, especially during the early stage of recovery. The timing of mobilization following hand surgery should be carefully balanced against the biological progression of tissue healing, the mechanical strength of the repair and patient-specific factors such as body image, sensory perception and tolerance to soft tissue loading. For example, delayed mobilization for up to 3–5 days allows inflammation and oedema to subside (Cevetello et al., 2025; Zhao et al., 2004). Early active motion must be initiated only when the integrity of the repair and the surrounding soft tissues can support controlled movement. On the other hand, it is well established that the negative effects of joint immobilization begin within the first few days with biochemical changes and can lead to movement restrictions after only 2 weeks (Schomacher, 2005). Therefore, rehabilitation should proceed in structured phases, guided by both objective markers (e.g. range of motion, grip strength) and subjective indicators (e.g. pain levels, patient-reported function), all matching the patient’s rehabilitation goals.
Effective communication
For rehabilitation to be successful, the patient’s values and preferences should be considered alongside medical evidence in a collaborative process where patients, hand therapists and surgeons work together. This continuous monitoring of the rehabilitation progress helps ensure that activity progression aligns with healing milestones and minimizes the risk of complications (Figure 1). Effective communication between surgeons and hand therapists is essential to prevent postoperative issues, including misunderstandings of surgical instructions, delayed or inappropriate therapy referrals, incorrect immobilization prior to therapy, and barriers related to insurance coverage or authorization (Valdes et al., 2019).
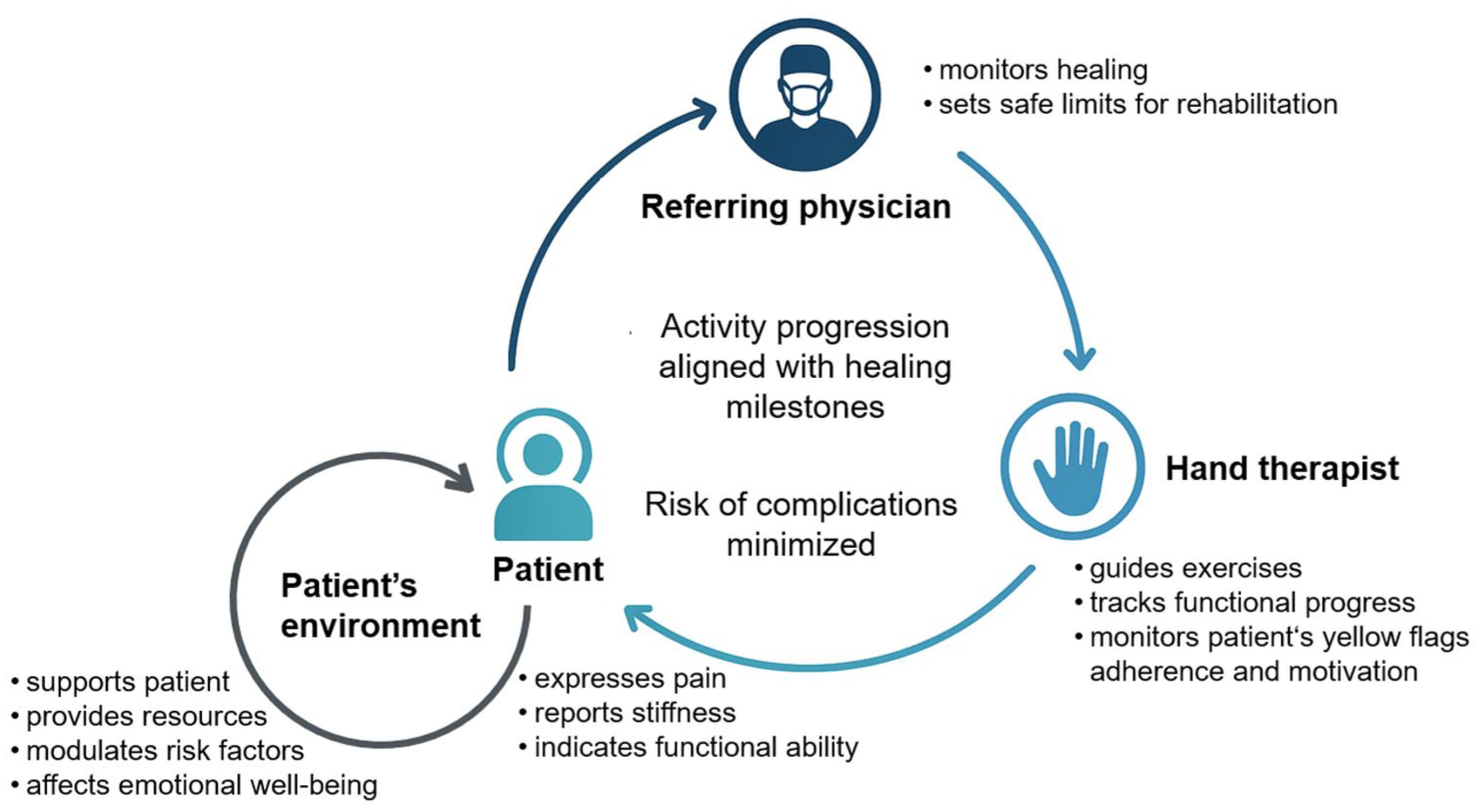
Shared decision-making process to monitor hand balance during rehabilitation. Continuous monitoring of balance through a feedback loop involving the referring physician, hand therapist, the patient and patient’s environment ensures that the progression of activity aligns with healing milestones and minimizes the risk of complications.
Challenges arise when therapists do not work directly with specialized hand surgery teams, limiting opportunities for clear communication. Similarly, referrals from general surgeons or non-specialized physicians may include rehabilitation instructions that diverge from evidence-based standards, reducing alignment between prescribed interventions and therapist judgment (Valdes et al., 2019). In these situations, therapists must base clinical decisions on information obtained during the patient’s initial appointment. A key consideration is whether the hand injury or disease is stable enough to allow early motion (Figure 2). Therefore, it is crucial that surgeons clearly explain how strong the fixation is and how confident they are in permitting EAM – or not. From there, potential risks – such as joint stiffness or surgical failure – should be weighed against the available therapeutic interventions. Regardless of circumstances, ongoing communication between the referring clinician and hand therapist remains central to optimizing patient care.
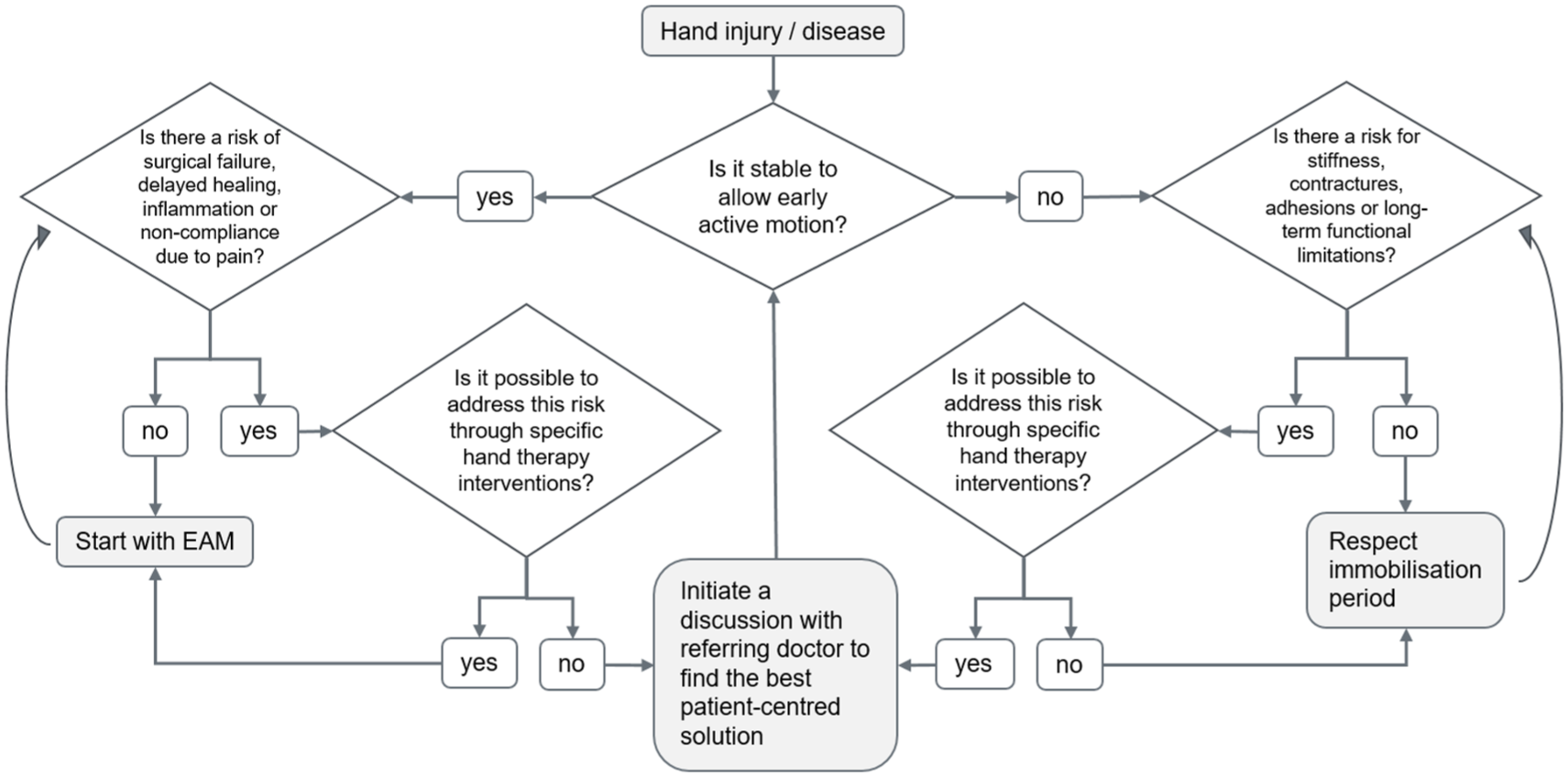
Clinical reasoning path for achieving balance in hand therapy.
Maintenance of balance during rehabilitation
Once hand rehabilitation has begun, it is the hand therapist’s responsibility to closely monitor the patient’s progress to maintain balance during recovery. Therapy protocols can serve as guidelines for staging progress week-by-week, helping therapists determine whether the patient’s recovery aligns with the expected course. However, hand therapists are often the first to identify complications and factors that influence patient decision-making. In this role, they play an important part in managing expectations, addressing fears and incorporating social and financial contexts through a tailored communication strategy (Lui and Jerosch-Herold, 2024). Therefore, understanding patient preferences and experiences helps adapt protocols to the individual, rather than relying solely on procedure-specific timelines, and is key to achieving successful hand therapy outcomes. During this itinerary, continuous reassessment of specific hand therapy outcomes – both clinician and patient-reported measures – is indispensable (Marks, 2020).
Building on ongoing assessment, hand therapists must continuously balance mobilization and immobilization, a process influenced by multiple interacting factors. The type and severity of the injury, as well as whether treatment is conservative or surgical, determine which structures need protection and which can tolerate early movement (Figure 2). Patient-specific factors – such as pain perception, functional ability, and engagement – interact with environmental influences, including social support, therapy setting and daily activity demands. The autonomic nervous system also plays a role, modulating swelling, muscle tone and pain responses, which in turn affects motion. Coordination with the surgeon ensures that clinical interventions – ranging from orthoses, taping, oedema and scar management, to electrotherapy – promote healing without overloading vulnerable tissues (Gordon and English, 2016; Harvey and Taylor, 2025; Taylor et al., 2025). Each factor can either support or hinder mobilization, and the combined effects are often unpredictable. Moreover, the patient’s body may employ compensatory mechanisms to restore functional balance, even when optimal conditions are not present (Browne et al., 2025). This dynamic interplay highlights that achieving balance is not a fixed outcome but a continuous negotiation shaped by injury, therapy, patient and environmental factors (Figure 1). The following case reports illustrate how hand therapists navigate the daily challenge of maintaining balance during rehabilitation.
Case report 1
A 24-year-old electrician sustained a metal cutter injury to his dominant right hand with subtotal amputation of the thumb at the metacarpophalangeal (MCP) level (type III), subtotal index finger amputation at the MCP level (type V), complete transection of the flexor digitorum profundus in zone II of the ring finger and 40% in the little finger. Both ring and little finger suffered a complete transection of the digital nerves and digital arteries. On the dorsal side of the hand, there was an 80% transection of the extensor digitorum communis tendon of the middle finger, and a pronounced dorsoradial soft-tissue defect of the hand (Figure 3a). He was surgically treated on the day of the injury with a primary policization (replantation of the proximal phalanx of the index finger to the proximal phalanx of the thumb) as well as nerve and flexor tendon sutures on the little and ring fingers, and extensor digitorum communis tendon suture of the middle finger. A full-thickness skin graft using residual skin from the thumb was placed on the back of the hand (Figure 3b), which was replaced by an interosseus-posterior flap 10 days later owing to necrosis (Figure 3c).
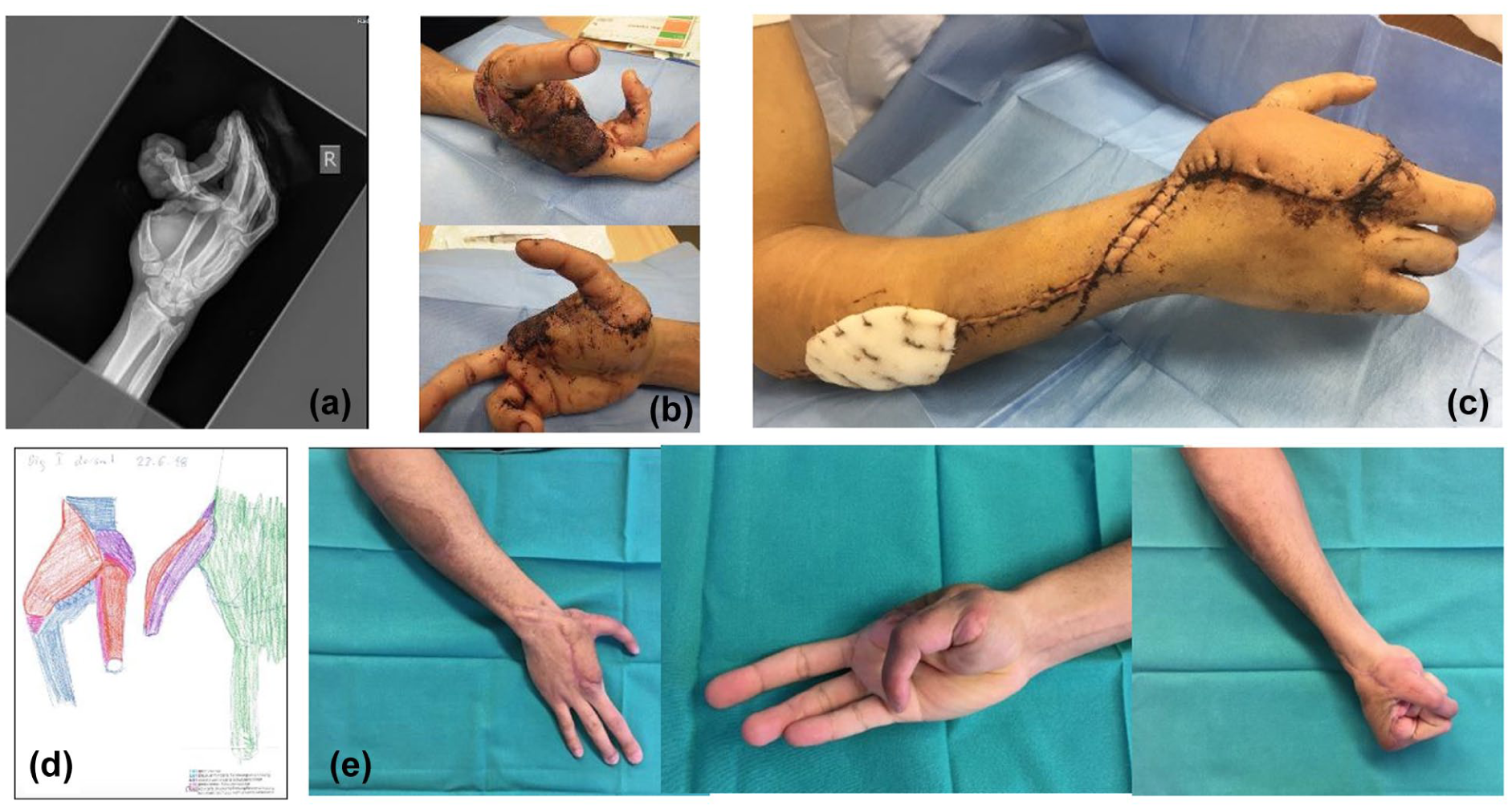
Case report 1.X-Ray of the injury, showing the extent of the bony injuries (a). Necrotising full thickness-graft nine days after surgery (b) and subsequent interosseus posterior-flap (c). Semmes-Weinstein Monofilament testing three months after surgery (d); green: 0.07g (normal light touch); blue: 0.4g (diminished light touch); purple: 2.0g (diminished protective sensation); pink: 4.0g (loss of protective sensation); red: 300g (deep pressure sensation only). Restored hand function at discharge eight months postoperatively (e).
In the acute immobilization phase, the balance between immobilization and graded mobilization had to be found to enable tissue healing while avoiding severe adherences and joint stiffness. Different rehabilitation protocols were combined to address all injuries: a dorsal splint with a palmar support in the palm of the hand was fitted, allowing for protected active mobilization. Ring and little fingers were treated following the controlled active motion protocol for flexor tendons (Giesen et al., 2017), while a Slater protocol was used for the middle finger (Slater and Bynum, 1997). The neo-thumb was mobilized actively without loading. Wound and scar treatments, as well as sensory re-learning were also part of the therapeutic interventions. Once loading was allowed at 8 weeks postoperatively, the re-training of fine motor skills in hand-coordination and strength was the main focus of therapy.
At 3 months postoperatively, the patient had difficulties using his neo-thumb for grasping and compensated with the use of his fingers, also because of lack of skin sensation (Figure 3d). At 6 months, the hardware (plate) was removed from the thumb, and a tenolysis of the extensor pollicis longus tendon was performed as well as a scar correction in the first web-space and thinning of the flap. Postoperatively, the thumb was immediately actively mobilized, and therapy continued on a regular basis. The MCP flexion improved significantly, allowing him to get better function. The patient was discharged 8 months after the accident after approximately 35 therapy sessions, having re-gained protective sensation (2.0 g) in the neo-thumb and reporting only a few limitations in everyday life (Figure 3e).
Case report 2
A 66-year-old right-handed male, a retired truck driver, presented with septic arthritis of the right wrist against the background of an undifferentiated rheumatic disease. Relevant comorbidities included hyperlipidemia, hypertension, aortic sclerosis, and chronic obstructive pulmonary disease with bronchiectasis owing to nicotine abuse.
The patient underwent multiple surgical interventions between March and May 2025, including synovectomy, proximal row carpectomy, repeated wound revisions with vacuum-assisted closure (VAC) therapy, and finally defect coverage with a radial rotation flap (15 × 5 cm²) and a full-thickness skin graft (13 × 4 cm²) (Figure 4a). Additional wound revision and debridement with placement of a biodegradable temporizing matrix were later required.
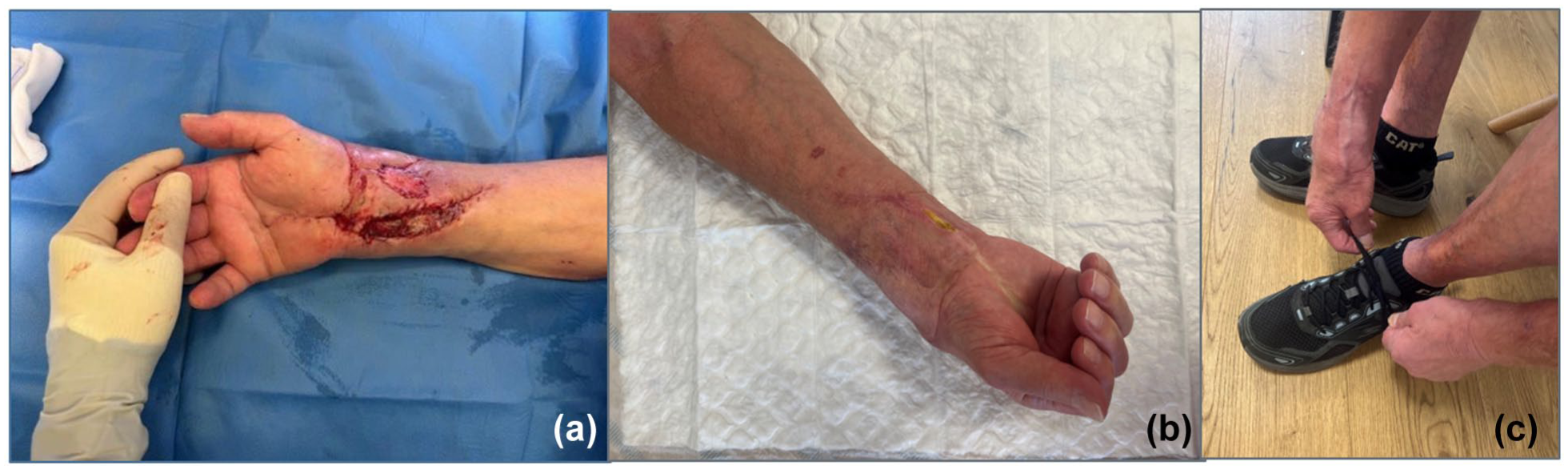
Case report 2: intraoperative image from May 2025, after rotational flap and full-thickness skin graft (a). Wound situation (b) and hand use in daily life (c) three months later.
Rehabilitation began with daily inpatient physiotherapy and continued with outpatient occupational therapy at weekly intervals. A key therapeutic challenge was to maintain a delicate balance between mobilization and immobilization following flap coverage, as early protection of the flap conflicted with the need to restore joint mobility. The right hand initially presented in a spontaneous intrinsic-plus posture, an unusual finding compared with the more common intrinsic-minus position seen after such injuries. Both active and passive range of motion were markedly restricted, and the patient was unable to use his dominant hand in daily life, effectively functioning as one-handed.
Through individualized splinting, active and passive mobilization, task-oriented exercises and continuous wound monitoring, gradual improvements were achieved (Figure 4b). The patient has regained the ability to perform essential activities such as eating and tying his shoes with the affected hand (Figure 4c). Nevertheless, maintaining his motivation has been challenging. This appears to be less related to the duration of the condition and more to the demands of frequent therapy sessions and medical appointments, which, combined with recent retirement and the resulting discrepancy between his anticipated and actual daily life, have contributed to reduced motivation and frustration, significantly affecting his quality of life.
Case report 3
A 62-year-old right-hand-dominant woman presented for therapy 2.5 weeks after carpometacarpal (CMC) joint arthroplasty of the dominant thumb. She reported severe constant pain (8/10), disturbed sleep, and avoidance of limb use. Active range of motion (AROM) at 2.5 weeks was 10° of flexion in the CMC I joint, 40° in the MCP (painful), and 20° in the interphalangeal joint. She was unable to perform grooming, cooking or opening containers. The initial examination showed swelling at the thenar base, shiny dorsoradial skin, hypersensitivity along the superficial radial nerve and a Disabilities of the Arm, Shoulder and Hand (DASH) score of 68.18 points (Hudak et al., 1996).
The rehabilitation programme emphasized pain modulation and sensory input before strengthening, with all interventions performed pain-free. During the initial phase (2.5 – 3.5 weeks), hand therapy interventions included light vibration, Kinesio Taping, poly pellet desensitization, splint fabrication and pain-free AROM only (Supplementary Video 1). At 3.5 weeks, focal vibration was introduced with tuning forks. The patient followed a home exercise programme with hourly AROM, daily vibration/heat and joint protection strategies. She attended therapy once weekly with excellent adherence. At 5.5 weeks postop (three visits, discharge), pain was resolved (0/10), full AROM and activities of daily living were restored, and the DASH score improved to 4.55 points (Supplementary Video 2). At 8 weeks, the hand surgeon recommended strengthening with yellow Theraputty with the consequence of pain recurrence up to 6/10 and limited thumb function at 9 weeks. After discontinuation of the Theraputty exercises, pain was resolved again, full activities of daily living restored and the patient was satisfied with treatment outcomes.
This case demonstrates that a sensory-first, multilayered, pain-free approach to CMC I arthroplasty rehabilitation can produce rapid recovery. Protocols are helpful for time frames, but not patient-specific, and may not account for motivation, comprehension or psychosocial factors. This intervention emphasized layered systems – skin, fascia, nerves and joint alignment – consistent with biotensegrity principles (Scarr, 2020; Swanson, 2013). The patient’s rapid recovery and regression with premature strengthening highlight the need for individualized dosing of care. A tailored, sensory-first, biotensegrity-informed rehabilitation programme led to complete pain resolution, full range of motion and near-complete functional recovery by 5.5 weeks postop. When strengthening was introduced prematurely, pain recurred but resolved upon return to sensory-based therapy. This case suggests that protocol-based care should be balanced with patient-specific, layered interventions for optimal outcomes.
How much balance is enough?
As the three case reports have shown, hand therapists apply a great variety of interventions to restore balance of the hand during rehabilitation. Yet a fundamental question remains: how much balance is enough? In most cases, hand injuries or diseases prevent full restoration to pre-injury function. Therapists must therefore weigh the potential benefits of continued intervention against the risks of overuse, patient burden and diminishing returns. The timing of discontinuing therapy is influenced by factors such as the natural course of recovery, the potential for surgical intervention and the patient’s functional goals. Therapy may be concluded when pre-set functional goals are achieved, progress plateaus despite continued intervention or patient motivation and adherence no longer support further gains (Cole et al., 2019). Decisions are guided not only by objective measures of mobility, strength and pain, but also by the patient’s priorities, functional needs and quality of life. Recognizing these limits and incorporating regular assessment and patient-centred planning is essential to ensure rehabilitation remains both effective and realistic.
Maintaining balance after rehabilitation
The ultimate goal of hand therapy is to enable patients to regain function and participate fully in daily and professional life. Achieving lasting balance depends not only on therapy but also on the patient’s active engagement: performing exercises, following recommendations, and taking responsibility for ongoing ‘hand health’. Surgeons and therapists alone cannot restore or maintain hand balance without the patient’s commitment. Unfortunately, determining whether therapy has been fully successful is often uncertain, as patients are frequently discharged while recovery is still ongoing – when further gains cannot be accelerated or improved through hand therapy interventions anymore. Some patients return for new hand issues, suggesting prior success, while others return for the same problem, indicating that the intended balance was not fully restored. This underscores that hand rehabilitation is a collaborative process (Figure 1), where the goal is to find a new balance, rather than striving to restore the balance to what it was before the hand disease or injury.
Conclusion
The choice between mobilization and immobilization depends on the specific injury, surgical technique, individual patient needs and performance demands. However, complications such as sympathetically driven pain or complex regional pain syndrome, or patient-related factors like emotional stress and pressure, may limit the possibility of early mobilization. Early mobilization after hand surgery is generally safe, improves short-term functional outcomes and speeds up recovery without increasing complications. Although long-term functional results are generally similar to those achieved with delayed mobilization, evidence supports minimizing immobilization when possible. However, there is often no clear consensus on the optimal timing to start postoperative mobilization. Some evidence suggests that more aggressive early rehabilitation may yield better results, but definitive guidelines are lacking (Cevetello et al., 2025; Lee et al., 2023; Mehta et al., 2024). These inconsistencies in practice highlight the need for clearer guidelines and further research to establish optimal rehabilitation strategies.
Hand therapy should be individualized based on injury type and patient factors, with protocols tailored to the patient rather than the procedure. Effective rehabilitation relies on clear communication and collaboration between the patient, the referring physician, and the hand therapist, as achieving optimal balance is a dynamic, ongoing process. Setting priorities together with the patient, combined with the therapist’s commitment to lifelong learning, is essential for delivering evidence-based, goal-oriented, and patient-centred care that is both effective and meaningful. Only when all factors are considered can the patient truly regain ‘balance’.
Footnotes
Acknowledgements
We would like to thank Professor E. Vögelin, MD, and Privatdozent P. Honigmann, MD, for giving us the opportunity to contribute to this Special Issue of the Journal of Hand Surgery (European Volume) in collaboration with FESSH.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This position paper does not require ethical approval.
Informed consent
Not applicable.
Artificial intelligence statement
Artificial intelligence was used in this manuscript for English proofreading and for drafting Figure 1.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.