
Abstract
Introduction
High peripheral nerve injuries disrupt the balance between flexor and extensor muscle groups and result in significant impairment of strength, coordination and dexterity. Primary nerve repair is widely accepted as the optimal treatment following transection injury, but outcomes after high-level nerve reconstruction remain unpredictable. Prolonged denervation commonly leads to irreversible muscle atrophy, limiting the potential for meaningful distal functional recovery despite technically successful nerve repair.
Reconstructive strategies:
Different surgical strategies are available to restore motor function after high peripheral nerve injuries. Tendon transfers have long been regarded as the reference standard for reconstructing lost muscle function, offering predictable and relatively early restoration of key movements. However, tendon transfers may compromise muscle balance, excursion, and fine motor control. Nerve transfers have emerged as an alternative strategy, aiming to prevent motor loss by reinnervating native muscles. While nerve transfers may better preserve physiological patterns of movement, they require prolonged periods for reinnervation and depend on patient factors, timing, and access to rehabilitation.
Review focus
More recent reconstructive strategies seek to combine the advantages of both techniques, offering ‘the best of both worlds’ through hybrid approaches that integrate tendon and nerve transfers. This expert opinion review discusses the current opportunities and challenges associated with these hybrid strategies in the management of high upper extremity peripheral nerve injuries. The biomechanical principles, indications and limitations of tendon transfers, nerve transfers and combined approaches are compared, with particular attention to timing, patient selection, and functional goals.
Keywords
Introduction
Peripheral nerve injuries, particularly high (i.e. above-elbow) lesions of the ulnar, median and radial nerves, are challenging for hand surgeons (Padovano et al., 2022). High peripheral nerve injuries disrupt the delicate balance between flexor and extensor muscles, affecting not only strength but also coordination and dexterity. Balanced hand function is defined by multiple factors, including but not limited to proprioception (Heroux et al., 2022), motor and sensory function (Duraku et al., 2024), and the synergy of agonist and antagonist muscles. Primary nerve repair is widely accepted as the best way to achieve neural and muscle recovery after transection injury (Dahlin and Wiberg, 2017). In above-elbow peripheral nerve injuries, however, the likelihood of permanent muscle loss is high despite timely nerve repair, particularly for distal muscles, such as those intrinsic to the hand. From a biological point of view, denervation leads to muscle degeneration with eventual irreversible loss of the potential for reinnervation within approximately a year (Gordon, 2020).
While the regeneration of proprioception and sensation is complex and hard to predict, motor recovery is directly related to the timing, strategy and quality of surgical treatment. Originally developed for the sequelae of polio, tendon transfers are the reference standard for reconstructing lost motor function, relying on predictable muscle mechanics and rapid rehabilitation (Meals and Meals, 2013, Seiler et al., 2013). For sequelae after a particular high peripheral nerve injury, specific combinations of tendon transfers are available to replace motor function and hand balance. There are, however, specific disadvantages of tendon transfers, such as the risk of biomechanical imbalance, reduced excursion, loss of strength and limited fine motor control (Wilbur and Hammert, 2016).
Nerve transfers offer an alternative method for restoring motor function and their utility has been evaluated in the management of proximal peripheral nerve injuries. During these procedures, expendable motor nerves in the vicinity of denervated muscles are used for rapid re-innervation. While the idea of transferring nerves is not new and goes back to the German surgeon Stoffel (Lurje, 1948, Vulpius, 1913), its use for high peripheral nerve injuries was popularized and refined through the clinical work of Mackinnon (Lowe et al., 2002, Mackinnon et al., 2007). There is now increasing evidence that nerve transfers can provide strength outcomes equivalent to tendon transfers, but also incorporate the benefit of restoring the original muscle physiology and balance (Bertelli, 2020). It is likely that motor nerve transfer facilitates both efferent and afferent fibre recovery, enhancing muscle control. In addition, the original muscle is reinnervated without altering the resting sarcomere length or changing its vector of action. Important disadvantages of nerve transfers are longer time to recovery and potential donor deficits.
Given the strength of both tendon and nerve transfer outcomes, it follows that hand surgeons should incorporate both techniques to achieve better outcomes in patients with peripheral nerve injuries. Decision-making for this ‘next-level’ hybrid approach must consider injury timing and location, as well as patient age and rehabilitation capacity. This approach combines the advantages of both techniques: rapid functional return after tendon transfer and restored muscle physiology after nerve transfers. This review discusses current opportunities and challenges of hybrid approaches to high upper extremity peripheral nerve injuries, critically comparing biomechanical principles, indications, and functional outcomes with the goal of restoration of balanced hand function.
Preoperative considerations and indications
Multiple factors contribute to the decision-making process when considering reconstruction of peripheral nerve injuries. In practice, preoperative planning is undertaken within a multidisciplinary team, typically involving the surgeon, hand therapist, neurologist/neurophysiologist and neuroradiologist (Shin et al., 2022). This team establishes baseline function and documents neurological deficit, in addition to agreeing a surgical strategy. Collaboration with a skilled hand therapist is helpful in assessing patient expectations and appropriateness for tendon transfer, nerve transfer, or a combined strategy (Lieberdorfer et al., 2023). The biggest variables that influence the decision to pursue a tendon or nerve based reconstructive strategy are the time from injury to surgery, the patient’s desired timeline for return to activity and the physiological likelihood of reinnervation related to the patient’s age and general health.
The amount of time elapsed between injury and evaluation will ultimately influence which options are available. Absence of detectable motor units on electromyography by 4 months is specific for lack of spontaneous recovery (Steenbeek et al., 2023), providing the opportunity to pursue reinnervation-based strategies if desired. If spontaneous recovery is not expected, options are discussed with the patient, including whether to continue observation (with the options of tendon transfers at a later date) or to proceed with nerve reconstruction, i.e. nerve transfers. For patients presenting greater than 1 year from injury with lack of function, nerve reconstruction is less predictable and tendon transfers alone may be the best option. If a rapid return to work is essential, tendon transfers are also favored over nerve transfers.
The patient’s age is critical when opting for or against nerve transfer reconstruction. Young patients (< 40 years), and particularly children, are excellent candidates for nerve transfer surgery since the reinnervation potential and central plasticity for motor relearning are high. In older patients (> 60 years), nerve transfer procedures should be indicated with caution and tendon transfers are a predictable and straightforward motor reconstruction. Other patient factors that have to be taken into account when discussing nerve transfers are uncontrolled diabetes and heavy smoking. Both medical conditions can negatively affect outcomes of nerve transfer-based reconstructions in our experience. Optimization of comorbidity, in addition to realistic goal-setting, should form part of the preoperative multidisciplinary team assessment.
Radial nerve
While there is continued enthusiasm regarding the potential benefits of using nerve transfers in the management of high radial nerve injury, the published scientific literature does not provide clear evidence of superiority over tendon transfer (Jain et al., 2024). Tendon transfers have the benefit of a shorter recovery period and typically provide the most reliable result for wrist extension but cannot provide independent finger extension and do not reliably restore thumb metacarpophalangeal or interphalangeal extension. Nerve transfers can provide independent extrinsic finger extension but require a longer period of recovery. Bertelli’s modification to target the deep branch of the posterior interosseus nerve has demonstrated promise to improve thumb metacarpophalangeal and interphalangeal extension, but results have not yet been reported beyond this single-surgeon experience (Bertelli, 2020). Given the lack of clear guidance from the published literature, surgeons are left to make individual decisions for each patient based on their own experience.
If a patient presents in a suitable window for nerve reconstruction (i.e. less than 6 months from injury) a combined strategy for radial nerve reconstruction can be pursued. For wrist extension, a pronator teres to extensor carpi radialis brevis tendon transfer and flexor digitorum superficialis to extensor carpi radialis brevis nerve transfer can be chosen (Figure 1). The tendon transfer provides immediate support for the wrist and allows the patient to transition out of an orthosis/brace sooner, while the additional nerve transfer gives an opportunity to augment wrist extension strength once reinnervation occurs (Davidge et al., 2013). For finger extension, a flexor carpi radialis to posterior interosseus nerve transfer is performed to allow independent extrinsic finger extension. Intraoperative evaluation can ensure that a second branch to the flexor carpi radialis is present to provide the options of a tendon transfer should the nerve transfer not provide adequate reinnervation. Similarly, preoperative examination can discern whether flexor carpi ulnaris is available as a backup donor tendon.
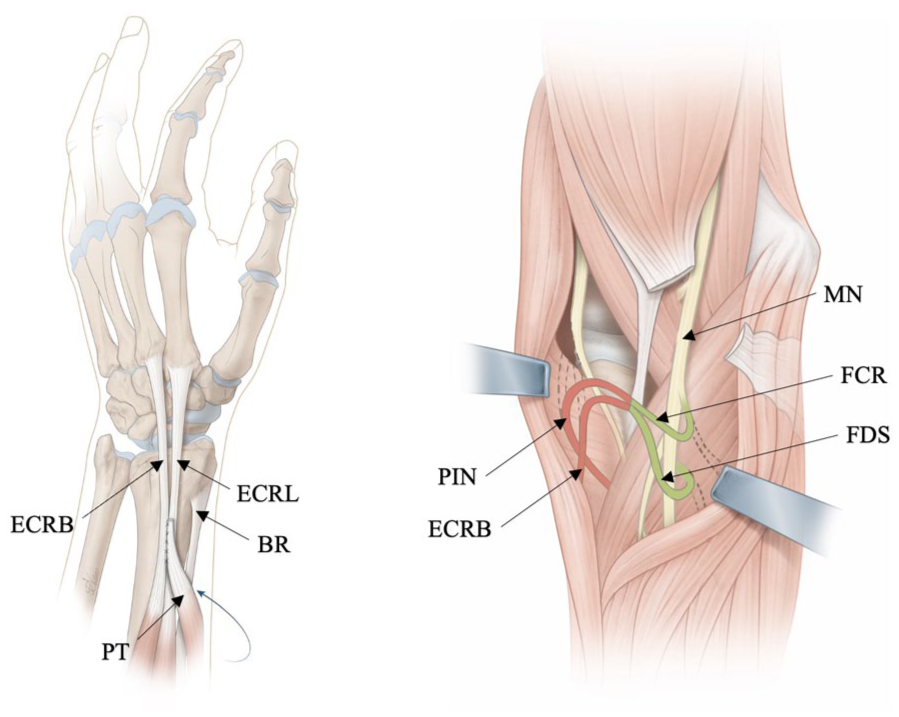
Hybrid option for high radial nerve injury.
For thumb extension, the pronator quadratus branch of the anterior interosseus nerve can be transferred to the deep radial branch of the posterior interosseus nerve to target thumb metacarpophalangeal and interphalangeal extension, given the shortcomings seen both in tendon transfers and in the original nerve transfer described by Ray and Mackinnon (Bertelli, 2020). For an overview on radial nerve tendon and nerve transfers see Table 1.
High radial nerve reconstructive options.
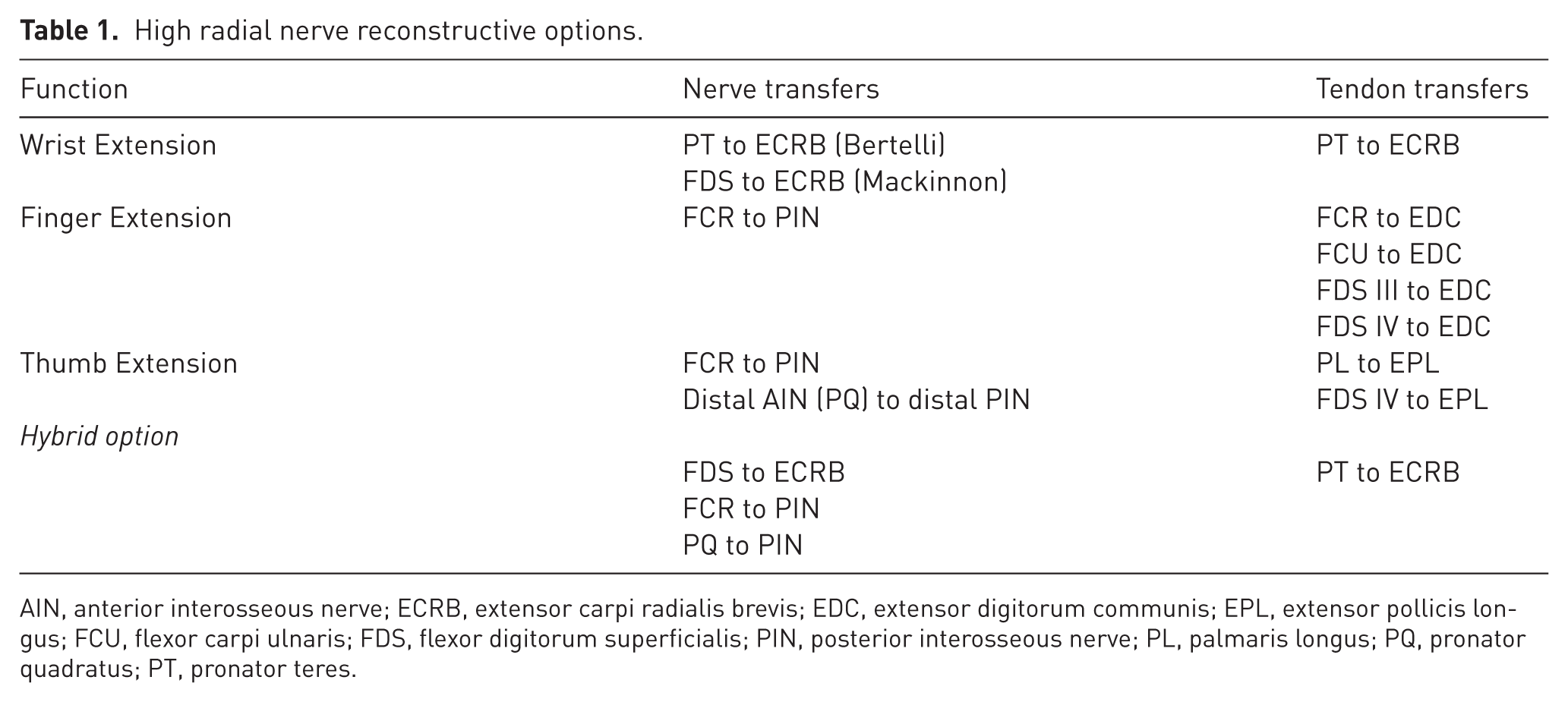
AIN, anterior interosseous nerve; ECRB, extensor carpi radialis brevis; EDC, extensor digitorum communis; EPL, extensor pollicis longus; FCU, flexor carpi ulnaris; FDS, flexor digitorum superficialis; PIN, posterior interosseous nerve; PL, palmaris longus; PQ, pronator quadratus; PT, pronator teres.
Ulnar nerve
Ulnar nerve injuries are classified into high and low lesions (Mannerfelt, 1966). High ulnar nerve injuries result in loss of ulnar wrist flexion from flexor carpi ulnaris, flexor digitorum profundus function of the little and ring fingers and loss of intrinsic function of the hand usually with a slight claw deformity. Low ulnar nerve lesions are defined as injuries distal to the innervation of the flexor carpi ulnaris and the flexor digitorum profundus to the ring and little fingers. They typically result in a more pronounced ulnar claw deformity compared with high nerve injuries owing to loss of intrinsic muscle action to balance extrinsic muscle forces, leading to metacarpophalangeal joint hyperextension and interphalangeal joint flexion of the ring and little fingers. Additional deficits include loss of key pinch strength (20–25% of normal) owing to paralysis of the adductor pollicis and first dorsal interosseous, and ulnar drift of the little finger, also called the Wartenberg sign. Restoring intrinsic muscle function and key pinch in ulnar nerve palsy remains challenging with tendon transfers, because of the complex biomechanics of the intrinsic muscles.
Claw deformity can often be managed with static and dynamic procedures such as volar plate advancement at the metacarpophalangeal joint or a Zancolli lasso, as long as there is no central slip attenuation from longstanding claw posture. The integrity of the extensor mechanism can be assessed using Bouvier’s manoeuvre (Bourrel, 1985). Dynamic tendon transfers include flexor digitorum superficialis to lateral bands and extensor carpi radialis brevis or longus transfer to the lateral bands with a two- or four-tailed tendon graft. Both tendon transfers require significant physiotherapy to achieve best results. High ulnar nerve lesions may be addressed by side-to-side tendon transfers of flexor digitorum profundus of the ring and little fingers to flexor digitorum profundus of the middle finger. Pinch restoration can be performed using an extensor indicis proprius tendon transfer to the adductor pollicis. Pinch may also be augmented by an abductor pollicis longus tendon transfer, lengthened with a tendon graft, to the first dorsal interosseous. Lastly, correction of ulnar drift can be performed with targeted tenodesis or tendon redirection albeit at a risk of little finger stiffness.
Despite these options, tendon transfers and static procedures such as volar plate advancement often improve the posture of the hand, but do not reliably restore intrinsic balance. Because of these limitations, primary nerve repair or grafting remains the first-line treatment whenever feasible. In proximal ulnar nerve lesions, particularly those proximal to the flexor carpi ulnaris, primary repair can restore wrist and finger flexion, but seldom leads to intrinsic reinnervation of the hand. In such cases, distal nerve transfers offer a means of restoring functional recovery while preserving the possibility of later tendon transfer procedures. Unlike tendon transfers, which merely replicate isolated movements, nerve transfers have the advantage of reanimating the original muscles. However, expectations must be tempered as the nerve donors are limited in fibre count to power the abundant needs of the intrinsic muscles of the hand.
The most well-known distal nerve transfer to reconstruct intrinsic muscle function is the anterior interosseous nerve to the motor branch of the ulnar nerve. This procedure can be performed in an end-to-end, end-to-side or hemi end-to-end fashion, all directed to the motor branch of the ulnar nerve. To optimize the axonal contribution, some authors have proposed dissecting the motor branch out of Guyon’s canal and excluding the abductor digiti minimi branch before coaptation. Despite its widespread use, the anterior interosseus nerve transfer remains controversial. There is ongoing debate regarding the ideal coaptation technique, and while several studies have reported that augmentation of proximal ulnar nerve repair with anterior interosseus nerve transfer improves strength and function regardless of the specific method, other studies have shown that end-to-end or end-to-side nerve transfers, when combined with proximal repair, do not reliably correct claw deformity or restore strength (Arami and Bertelli, 2021, Gross et al., 2023).
An additional distal transfer more recently described is the opponens pollicis nerve of the median nerve transfer to the ulnar branch innervating the adductor pollicis and first dorsal interosseous to restore pinch. Bertelli demonstrated encouraging results with this technique, particularly in restoring pinch without compromising thumb function (Bertelli et al., 2019, Bertelli, 2024). Since the anterior interosseus nerve transfer alone may not provide sufficient axonal input to reinnervate both the intrinsic muscles and the adductor/first dorsal interosseous, a double nerve transfer combining the anterior interosseus nerve and the opponens pollicis branch of the median nerve can be performed at the time of proximal ulnar nerve repair (Figure 2). Hybrid reconstructions are also possible, for instance as single-stage procedures in which primary ulnar nerve repair is combined with metacarpophalangeal volar plate advancement or side-to-side flexor digitorum profundus tendon transfer and double nerve transfers using both the anterior interosseus nerve and opponens. Sensory deficits are generally limited to the volar ulnar aspect of the hand and the little finger. Primary repair, even in high ulnar nerve injuries, may restore some protective sensation. If primary repair is not possible, sensory nerve transfers have been described using the third webspace of the median nerve and side-to-side bridge grafts with nerve grafting in the palm. Table 2 provides an overview for ulnar nerve tendon and nerve transfers.
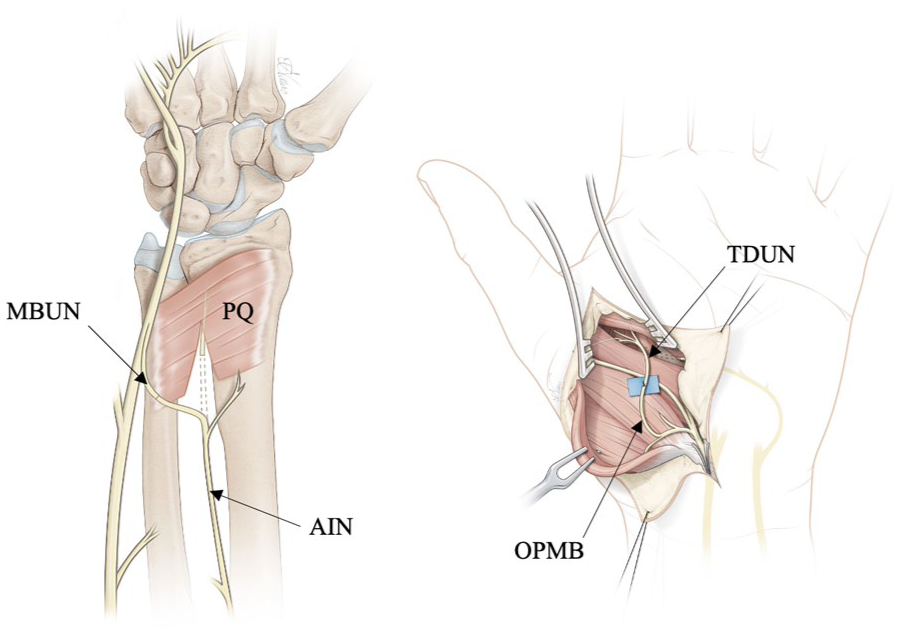
Nerve transfers for high ulnar nerve injury.
High ulnar nerve reconstructive options.
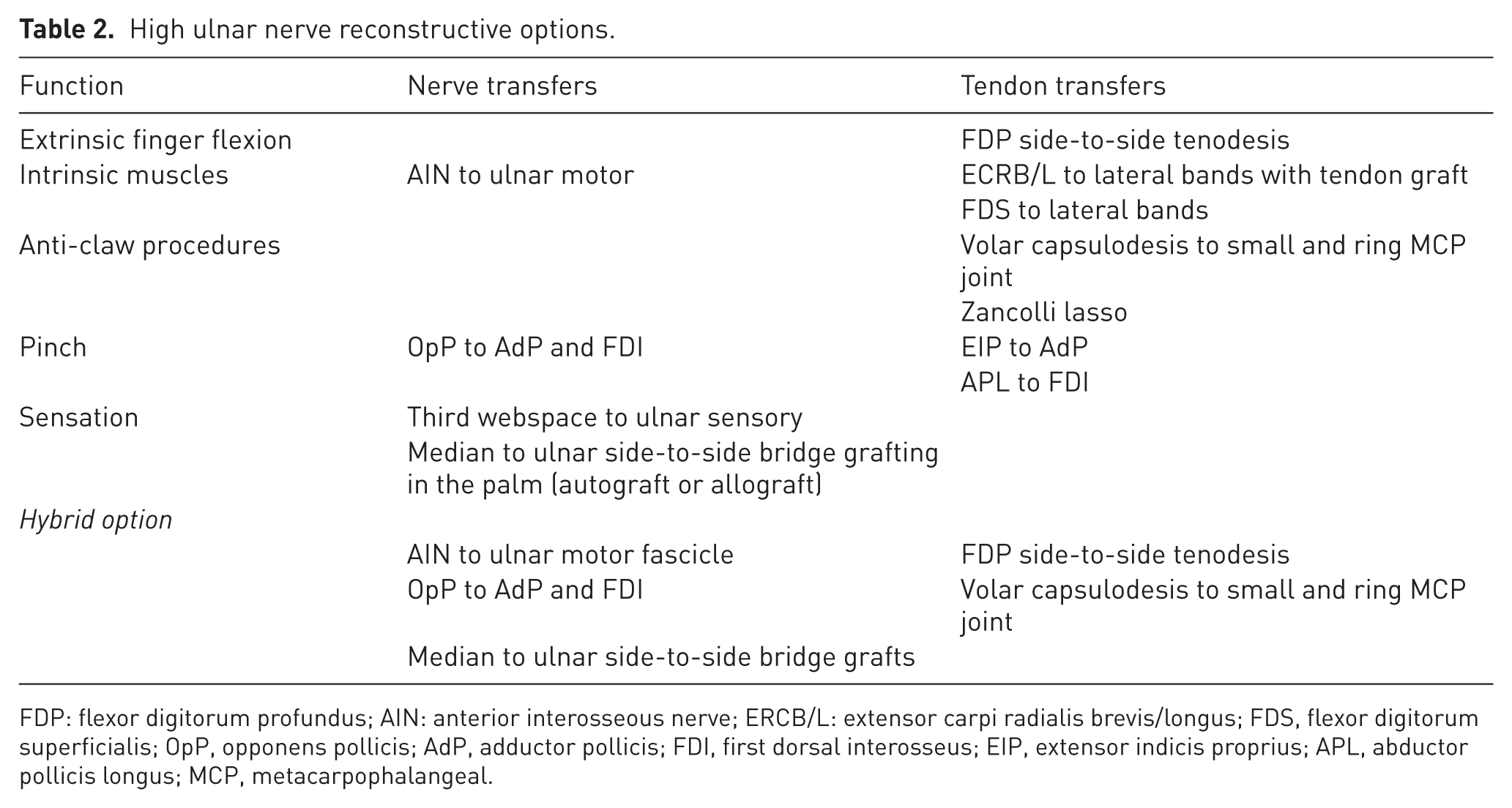
FDP: flexor digitorum profundus; AIN: anterior interosseous nerve; ERCB/L: extensor carpi radialis brevis/longus; FDS, flexor digitorum superficialis; OpP, opponens pollicis; AdP, adductor pollicis; FDI, first dorsal interosseus; EIP, extensor indicis proprius; APL, abductor pollicis longus; MCP, metacarpophalangeal.
Median nerve
High median nerve lesions are defined as injuries proximal to the anterior interosseus nerve origin. Loss of pronator teres, flexor digitorum superficialis and profundus to the index and middle fingers proximally, and loss of thumb flexion and opposition distally, can be observed. On attempted fist formation, the most striking findings are paralysis of the thumb interphalangeal and index distal interphalangeal joints, along with thumb adduction owing to preserved ulnar innervation of the adductor pollicis and the deep head of the flexor pollicis brevis (Duraku et al., 2022). Grasp and pinch weakness are present in all cases. Despite denervation of both the pronator teres and quadratus muscles, forearm pronation is typically preserved up to 50° owing to the action of brachioradialis (Bertelli et al., 2016). Sensory deficits involve the palmar skin of the middle and distal phalanges of the index and middle fingers, and the distal phalanx of the thumb.
Proximal median nerve reconstruction can be performed to restore proximal function and protective sensation, and for the treatment of pain. Similar to the ulnar nerve, restoration of intrinsic function and sensation is unlikely with high median nerve injuries. If the patient presents outside of the nerve reconstruction time frame, tendon transfer of the brachioradialis to the flexor pollicis longus improves thumb interphalangeal joint flexion. This can be combined with a side-to-side flexor digitorum profundus tenodesis to the ulnar innervated deep flexors of the ring and little fingers. An extensor carpi radialis longus tendon transfer to index flexor digitorum profundus can also be performed for isolated index finger flexion (Isaacs and Ugwu-Oju, 2016).
Thumb opposition is essential for hand function. Thus, opponensplasty tendon transfers and nerve transfers exist to restore this essential thumb positioning and should be considered early for improved hand function after high median nerve injuries at the time of primary nerve reconstruction. Opponensplasty tendon options include using the extensor indicis proprius or ring finger flexor digitorum superficialis to abductor pollicis brevis for palmar abduction (Seiler et al., 2013, Soldado et al., 2016).
Hybrid tendon and nerve transfer strategies are now being considered with the design of proximal and distal nerve transfers. In patients referred more than 12 months post-injury, tendon transfers remain the mainstay of treatment. However, when reinnervation is feasible within 6 months of injury, nerve transfers may be combined with side-to-side flexor digitorum profundus tenodesis. Restoration of thumb and index finger flexion can be achieved via extensor carpi radialis brevis branch to anterior interosseus nerve transfer, increasing grasp and pinch strength (Figure 3). Additional grasp power may be gained by transferring a supinator nerve branch to the nerve to the flexor digitorum superficialis (Bertelli, 2015). As pinch strength relies on both extrinsic and intrinsic function (Kozin et al., 1999), restoring thenar muscle activity is essential. For this purpose, the motor branch to the abductor digiti minimi nerve can be transferred to the thenar branch of the median nerve, improving opposition. Additional tendon transfer to the abductor pollicis brevis may be reserved for those failing to regain useful thumb positioning using this approach.
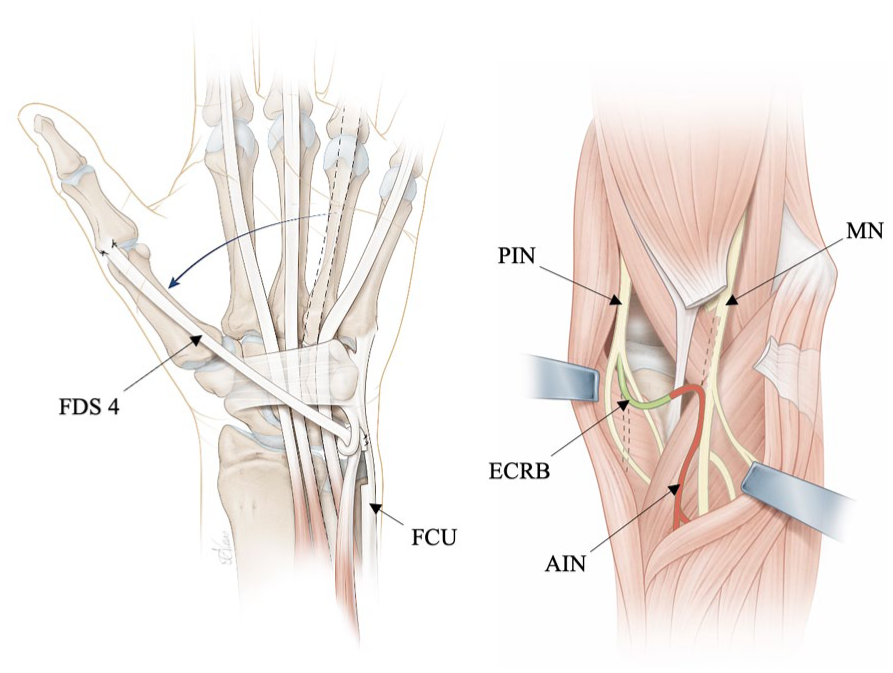
Hybrid option for high median nerve injury.
A frequently underestimated problem after high median nerve injury is loss of discriminatory sensation in the thumb and index fingertip pulps. To avoid this, sensory radial to median nerve transfers distal to the metacarpophalangeal joints can be performed, with minimal risk of introducing neuropathic pain (Bertelli and Ghizoni, 2011). Recent studies confirm that these distal transfers offer good fascicular size match and favorable clinical outcomes (Orlando et al., 2025, Schaeffer et al., 2025). Importantly, neurotization of a single digital nerve may be sufficient, as cross-over innervation can restore full pulp sensibility (Weinzweig, 2000). Unlike motor nerve transfers, the optimal timing for sensory transfers is unclear but we believe that they can still be effective in delayed cases to rebalance sensory-motor hand function. For an overview on median nerve tendon and nerve transfers see Table 3.
High median nerve reconstructive options.
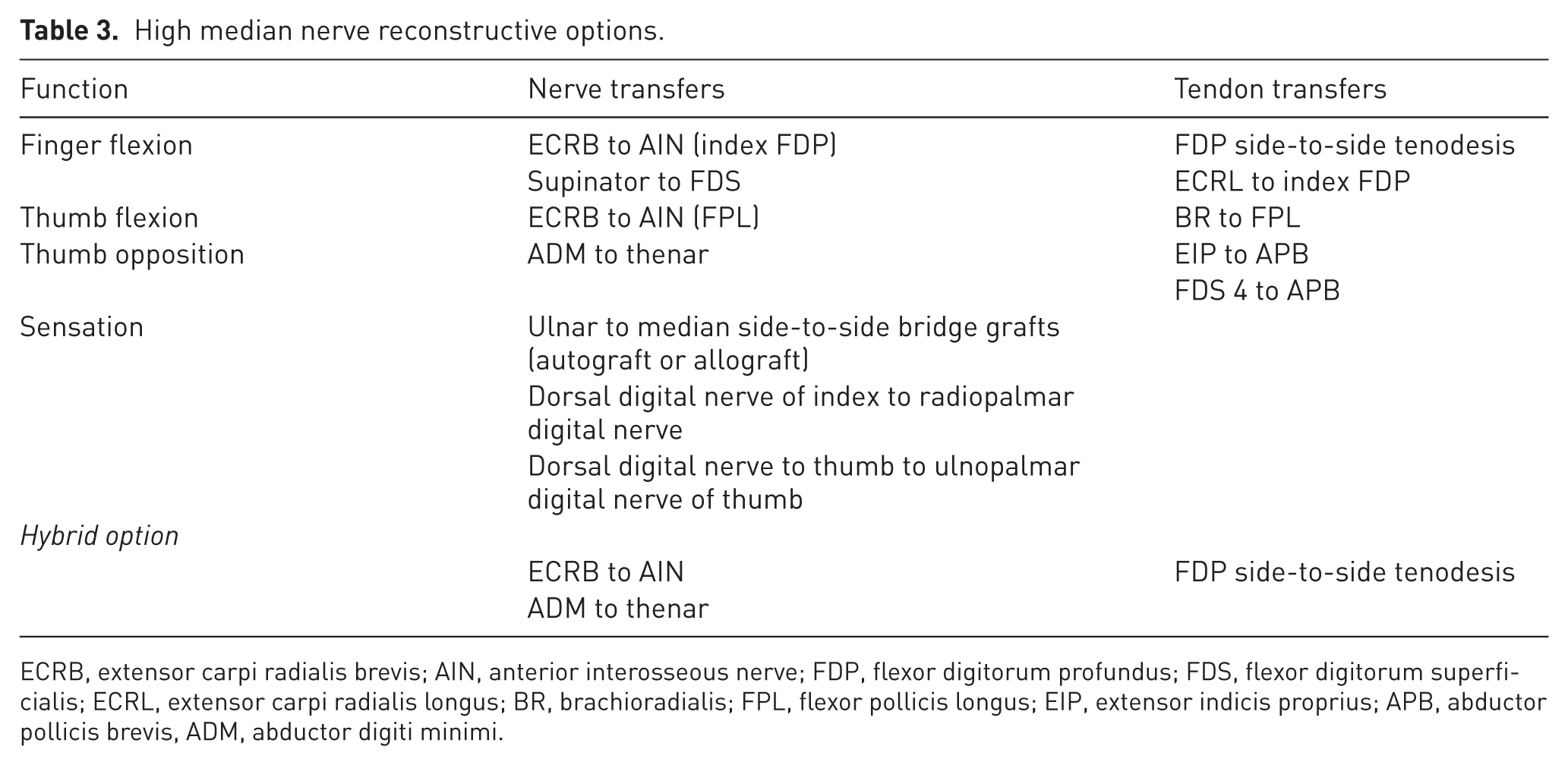
ECRB, extensor carpi radialis brevis; AIN, anterior interosseous nerve; FDP, flexor digitorum profundus; FDS, flexor digitorum superficialis; ECRL, extensor carpi radialis longus; BR, brachioradialis; FPL, flexor pollicis longus; EIP, extensor indicis proprius; APB, abductor pollicis brevis, ADM, abductor digiti minimi.
Discussion
Prompt recognition and early repair are essential in the management of high peripheral nerve injuries in the upper limb, providing a route for proximal muscle reinnervation and proprioceptive feedback. For the median and ulnar nerves with a major sensory component, there is the possibility of useful protective sensation restoration and reduction in neuropathic pain. However, nerve recovery after high nerve reconstruction can be unpredictable and thus it is important to utilize all options available. As techniques are developed and our predictions of outcomes improved, hybrid approaches that combine both tendon and nerve reconstruction should be considered.
Time from injury remains a critical decision point when determining options for nerve and/or tendon reconstruction. Tendon transfers for proximal functions may be used when there is no useful motor recovery from the proximal nerve repair or when presentation is later than 12 months from injury and useful proximal motor recovery is unlikely. When presenting less than 6 months from injury, nerve transfers remain a viable option. It is important to consider the patient appropriateness, expectations and access to postoperative hand therapy.
Whether there are functional advantages of hybrid approaches encompassing nerve repair, nerve transfer and tendon transfer is unproven; however, the poor results of nerve repair alone for distal function restoration and the limitations of tendon transfers when used for key motor functions are well documented. A pragmatic approach to nerve injury management is needed, accepting the current limitations of surgical repair and utilizing all available tools for functional restoration. Early repair combined with distal nerve and tendon transfers facilitates earlier functional use of the hand in selected patients.
Clinicians involved in the management of high peripheral nerve injuries should achieve consensus on outcomes reporting and by agreeing a core outcome dataset, meta-analysis of clinical outcomes will help to elucidate the nuances of individualized hybrid approaches. The role of sensory nerve transfer is not yet well defined, and the evidence to support adoption of these techniques is limited to a few small case series. Nevertheless, reconstructive surgeons should be aware of these possibilities in cases where proximal nerve repair is not possible, or where sensory deficit persists despite reconstruction.
In conclusion, balancing hand function through combining nerve repair with nerve transfer (when indicated) and tendon transfer surgery may maximize muscle reinnervation and early functional hand use. This balanced approach to the management of high peripheral nerve injuries recognizes the limitations of existing approaches and the fallibility of any single reconstructive technique used to treat these disabling injuries. Future research on the outcomes of hybrid approaches is needed, but when considering the challenges of restoring both motor and sensory function, focusing on the use of all options is essential for optimizing patient outcomes after high peripheral nerve injuries.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed consent and ethical approval
This was not sought for this article because it does not contain experimental or clinical data.